
記住我
In this comprehensive review, we conducted a systematic literature search using PubMed and the Scopus Index as primary resources to explore the modulation of the IC in the context of TNP. Our search strategy involved a computerized examination of journal articles without restricting the publication date, employing a broad spectrum of keywords such as “pain,” “trigeminal neuropathic pain,” “insular cortex,” “orofacial pain,” and “trigeminal neuralgia” to ensure comprehensive coverage of the topic.
To thoroughly investigate the functional role of the IC in TNP, our review included studies encompassing both animal models and human subjects. The inclusion of animal studies allowed to understand foundational biological processes and experimental therapeutics, while human studies provided insights into clinical manifestations, imaging findings, and therapeutic outcomes. This dual approach enabled a holistic understanding of the IC’s role across different experimental and clinical settings.
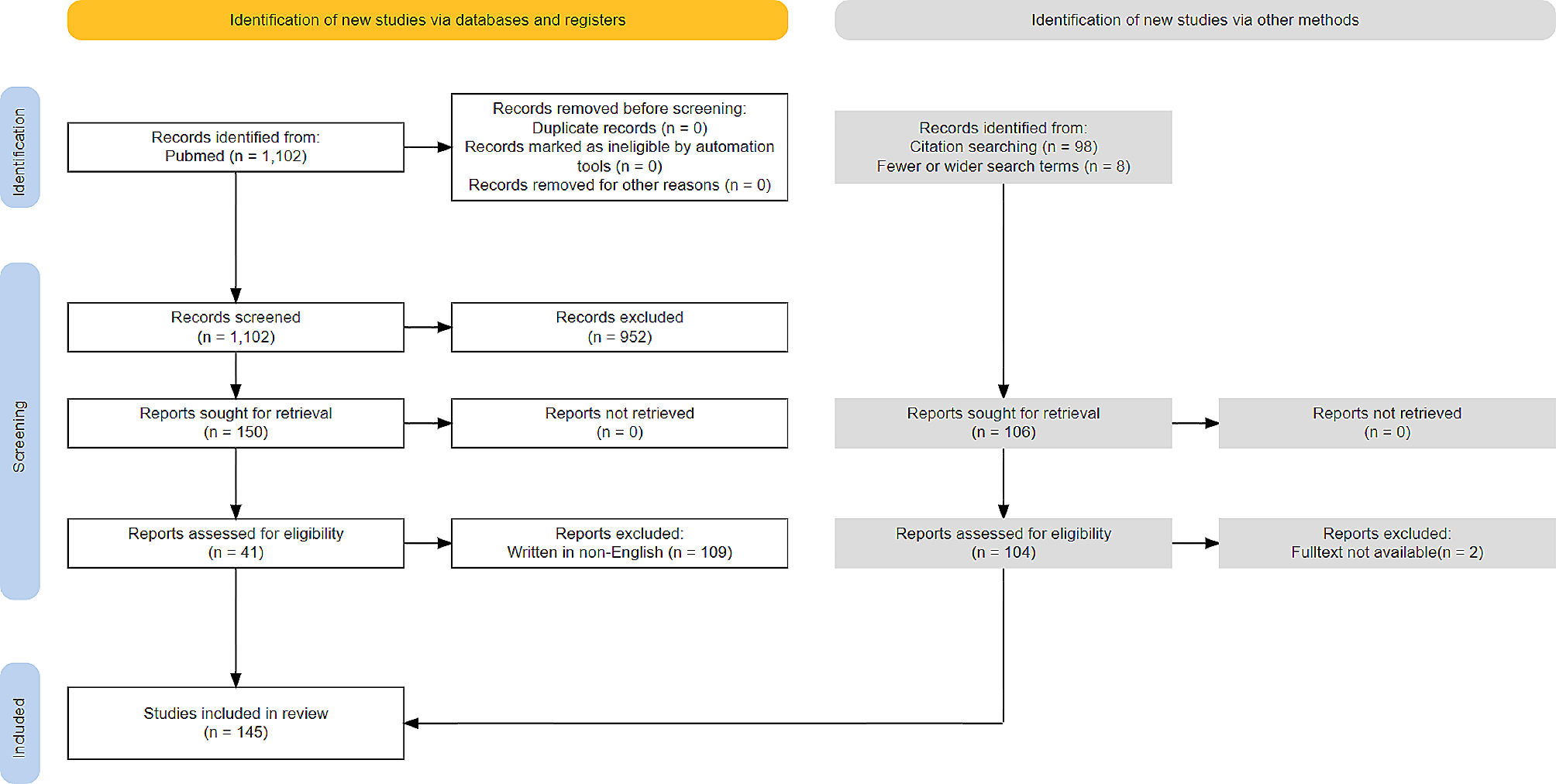
We selected 164 non-duplicated entries, employing a rigorous criterion that focused on the relevance to our area of interest, and the novelty of findings related to the role of the IC in TNP. An initial screening of titles and abstracts, primarily conducted by the first author, identified 107 studies that significantly contributed to our understanding of the IC’s involvement in TNP. These articles were chosen based on their discussions about alterations to the IC following the condition and the various neuromodulation techniques targeting the IC. Our review synthesizes findings associated with the IC in the context of TNP, which encompasses orofacial pain, trigeminal neuropathic pain, and trigeminal neuralgia, ensuring a scientifically robust selection of literature.
Structure of insular cortexThe IC, integral to the processing of multimodal inputs, is delineated by its anatomical location and cytoarchitecture across species. IC is divided into two parts: AIC and PIC. The AIC is comprised of three short gyri which are involved in processing emotions, empathy and social awareness. On the other hand, PIC is comprised of two long gyri which are implicated in perception, motor control, self-awareness and sensory integration [34, 48, 92]. In rats, it lies over the claustrum, bordered rostrodorsally by the lateral frontal and primary somatosensory cortices (SI), caudodorsally by the secondary somatosensory cortex (SII), ventrally by the piriform cortex, and caudally by the perirhinal cortex [60, 86]. In primates, it resides within the lateral sulcus’s fold, comprising anterior and posterior sections with distinct connectivity profiles [96]. Cytoarchitecturally, the IC in primates, including humans, is divided into granular, dysgranular, and agranular areas. The agranular insular cortex (aIC), situated in the AIC, is characterized by its prominent layers II–III, V, and VI, and is mainly associated with efferent functions. The dysgranular insular cortex (dIC), found between the granular and agranular areas, has fewer granule cells in layer IV and a significant layer V. It plays a role in integrating sensory and emotional information, with both afferent and efferent functions. The granular insular cortex (gIC), primarily located in the PIC, is known for its pronounced layer IV and is more associated with afferent pathways [3, 33, 61].
Functions of insular cortexFunctionally, the insula is implicated in diverse processes. It acts as the primary gustatory cortex [14], visceral [88], and thermosensory cortex [20], embodying the primary interoceptive cortex that reflects the body’s physiological and homeostatic conditions [61]. The PIC, specifically, is known to receive substantial sensory input from cortical sources, highlighting IC’s integral role in comprehensively processing somatosensory information [38]. This extensive sensory integration indicates the capability of IC to mediate complex interactions between different sensory modalities and the neural network involved in higher-order processing. Its role also extends to embodying consciousness and self-recognition, evidenced by activation upon viewing one’s images [28] during awareness of heartbeat, bodily control, and emotions [19]. Its integration with the limbic system underlines its crucial role in emotional processing, including negative behaviors like fear and anxiety [32, 52] and positive emotions such as happiness [61].
Cognitively, the IC is involved in aversive and affective learning, as shown in rat studies [53, 85], aligning with its role in the salience network [94]. It participates in anticipating future states, prediction error computation, and risk estimation, responding predictively to relevant physiological stimuli [6, 40, 67]. This mediation between physiological states and motivated behaviors underscores its significance in both normal and pathological conditions [6, 21, 79].
Pathologically, variations in insular function and structure are linked to anxiety disorders [82], major depression [5, 76], autism spectrum disorders [95], schizophrenia, obesity, and addiction [30], highlighting its pivotal role across a spectrum of mental health and behavioral conditions. In addition, the IC plays a multifaceted role in motor control by integrating sensory, emotional, and cognitive information to influence motor functions, including planning, execution, learning, and adaptation. It coordinates with other motor control areas, processes pain, and modulates autonomic responses, highlighting its integral role in the complex interplay between motor activities and internal states [87].
Chemoarchitectural features of IC involved in trigeminal pain processingThe IC significantly influence TNP through its complex chemoarchitectural characteristics. The extensive expression of neurotransmitter receptors situated in the IC, including opioid, cannabinoid, dopaminergic, and glutamate receptors, enzymatic activities, and specific neurocytological profiles underpins its critical function in the TNP [39, 62]. aIC and dIC, known for their reduced myelination and distinct acetylcholinesterase activity, suggest a unique substrate that may influence signal propagation speed and integration, particularly relevant to the processing of TNP signals [36]. The presence of µ-, δ-, and κ-opioid, along with nicotinic acetylcholine receptors in the IC, highlights its role in modulating pain relief, reward, and addiction. In addition, cannabinoid receptors and serotonergic receptors such as 5-HT1A, 5-HT2A, 5-HT2C, 5-HT3, and potentially 5-HT4, 5, 6, 7, within the IC influence the perception of TNP [62, 93].
In TNP, alteration in dopaminergic neurotransmission circuitry affects multiple brain regions such as IC and nucleus accumbens core (NAcc). Since IC has output projections towards NAcc and NAcc modulation have been found to be involved in TNP, IC dopaminergic neurotransmission can influence TNP [15, 38, 39, 49].
Studies have further elucidated that glutamatergic mechanisms within the IC contribute to central sensitization and the modulation of TNP. Alterations in glutamate receptor expression, such as NMDAR and AMPAR, have been associated with TNP, suggesting the pivotal role of excitatory neurotransmission and synaptic plasticity within the IC [50, 59]. GABAergic mechanisms within the IC have also been increasingly recognized for their contribution to neuroplasticity and neuromodulation, particularly in the context of emotional regulation and interoceptive awareness [39].
In addition, increased Phospho-Extracellular Signal-Regulated Kinase (pERK) activation in the IC is associated with central sensitization of TNP [3, 98].
Relationship between insular cortex activity and trigeminal neuropathic pain in human studiesRecent evidence demonstrated the critical involvement of both AIC and PIC in the TNP processing pathway, with alterations in GMV commonly observed in TNP cases [26, 27, 42, 47, 64, 72]. Functional imaging techniques, such as Positron Emission Tomography (PET) and functional Magnetic Resonance Imaging (fMRI), have confirmed the activation of IC in response to nociceptive orofacial stimuli, with the AIC implicated in higher-level pain interpretation and the PIC in basic sensory pain processing [10, 11, 31, 71, 89]. Furthermore, individuals with trigeminal neuralgia (TN) showed significant functional connectivity changes and microstructural integrity alterations in the white matter volume (WMV) of the IC [100, 107]. The role of IC extends beyond processing orofacial sensations to integrating sensory inputs from both primary (SI) and secondary (SII) somatosensory cortices [57]. In the IC, there is a distinct pattern of intra-insular outputs, with a greater number from the PIC than the AIC, suggesting a directional, caudal-to-rostral flow of information within the IC [39]. Therefore, interruptions in connectivity between the AIC and PIC, whether due to lesions or neuromodulation, have been associated with impairments in trigeminal pain and temperature sensations [31].
The AIC not only processes pain intensity and the emotional dimensions of pain experiences but also plays a crucial role in anticipating pain and facilitating human awareness [7, 31]. Intriguingly, after effective treatment for TN, the ventral AIC often shows a normalization of GMV and cortical thickness, suggesting neuroplastic adjustments that correlate with clinical improvement [26, 27].
On the other hand, PIC is essential for processing pain and tactile sensations, serving as a primary cortical hub for integrating internal and external bodily signals [10, 38]. Its role in somesthesis is underlined by its connections with the spinothalamic tract and the reception of nociceptive and thermoceptive information via the lamina-I-spinothalamocortical pathway from the posterior thalamic nuclei, which are crucial for the sensory discriminative aspects of trigeminal pain [71, 83].
Relationship between insular cortex activity and trigeminal neuropathic pain in preclinical studiesRecent preclinical studies have been pivotal in elucidating the insula’s role in trigeminal pain perception, building on the findings from human research. Rodent and monkey studies confirm the IC’s response to trigeminal pain through its activation to oralfacial nociceptive stimulation [3, 57, 71, 89]. Furthermore, animal studies reveal that IC lesions can mitigate neuropathic and inflammatory pain [44].
At the molecular level, trigeminal nerve injuries activate the ERK-CREB pathway in the IC, leading to an upregulation of glutamate receptors (AMPA and NMDA) and a downregulation of inhibitory potassium channels activity, which promotes neuronal long-term potentiation associated with trigeminal pain [98]. Enhanced excitatory neural responses in the dorsal IC following sensory stimulation have been observed in rats with trigeminal neuropathy [35]. Furthermore, plastic changes in neuronal circuitries from the IC to the trigeminal nucleus caudalis (TNC) may amplify responses to peripheral noxious stimulation [78].
The AIC is significantly responsive to alterations in nociceptive inputs from trigeminal afferents. Enhanced phosphorylation of ERK-1/2 in layers II-III, areas known for housing nociceptive-specific neurons, indicates the active involvement of AIC in TNP processing [3]. Additionally, the AIC influences spinal cord activities through top-down modulation, likely mediated by noradrenergic outputs from the locus coeruleus (LC), which interacts with inhibitory inputs from the lateral parabrachial nucleus (PBN) and raphe magnus nucleus (RMN). This complex interplay indicates the integral role of AIC in both initiating and modulating the pain response, particularly in conditions like TN where neurovascular compression is a significant factor [16, 56].
On the contrary, the PIC plays a critical role in TNP by regulating orofacial sensory-motor functions, and serving as a hub for thalamic sensory inputs [2, 81, 103]. Research in monkeys shows the PIC receives specific thermal and pain signals, integrating them with broader autonomic and limbic systems [20]. Additionally, the PIC processes a diverse array of information, including sensory discrimination, highlighted by increased brain activity in conditions like brush-evoked allodynia. This demonstrates its capacity for neuroplasticity and neuromodulation, as evidenced by studies on somatosensory-evoked potentials [10, 23].
Further, the PIC integrates sensory, autonomic, motor, associative, and limbic inputs, maintaining strong internal connections that facilitate its involvement in varied stimuli and emotional states [38, 84]. In the chronic constriction injury of the Infraorbital neve (CCI-ION) rat model for TNP, increased activity of dysgranular PIC (dPIC) glutamatergic neurons (dPICg) in response to the nerve injury had been observed, which was associated with enhanced expression of pERK and CREB in the dPIC. This suggests the nociceptive processing role of dPIC involving glutamatergic neural networks during TNP [50].
Table 1 Overview of clinical and preclinical studies on the insula in trigeminal neuropathic painProjections of insular cortex to and from other trigeminal neuropathic pain-associated brain regionsThe IC is a hub for processing multisensory information, with each of its subdivisions playing distinct roles in handling various types of sensory data. Beyond receiving inputs from several brain areas, the IC has excitatory projections to different brain structures as well, enriching its multisensory processing capabilities with emotional and affective context (Fig. 1). This convergence ensures that sensory information processed within the IC is seamlessly integrated with limbic information, highlighting its comprehensive role in sensory perception and emotional regulation. However, it is important to note that most of the studies documenting these functions and projections are based on animal models, which could have implications for direct translational relevance to human anatomy and pathology.
Fig. 1
Connections of IC with different brain regions. (A) Projections of IC with other brain regions. (B) Altered projections of IC with other brain regions in TNP. IC = insular cortex, OFC = orbitofrontal cortex, PFC = prefrontal cortex, MC = motor cortex, SSC = somatosensory cortex, NAc = nucleus accumbens, Str = striatum, Thal = thalamus, Hyp = hypothalamus, Amyg = amygdala, PAG = periaqueductal gray, RMN = raphe magnus nucleus, PBN = parabrachial nucleus, LC = locus coeruleas, RVM = rostral ventromedial medulla, TNC = trigeminal nucleus caudalis
Trigeminal nucleus caudalisIn TNP research, significant insights have been gained into the functional anatomy of the IC and its connections to the TNC and the trigeminal subnucleus oralis (Vo) [3, 98]. Descending projections from the IC, specifically targeting lamina I of the medullary dorsal horn and Vo, underscore the IC’s pivotal role in conveying orofacial nociceptive information [2, 20, 104]. The gIC and dIC have been shown to project to both the rostral and caudal parts of TNC laminae I/II, as well as to Vo, through the corticotrigeminal pathway [2, 25, 78,
留言 (0)