
記住我

What is known about the topic?
The use of a central venous catheter (CVC) is the most common intervention for critical illnesses. CVC occlusion can increase the risk of catheter-related bloodstream infections (CRBSI) and lead to fatal consequences for patients. CVC obstruction is a common problem in acute care.What does this article add?
Strategies to improve compliance with evidence-based criteria regarding nurses’ education may include literature-based teaching combined with video tutorials and the use of Objective Structured Clinical Examination (OSCE). It may be possible to address the healthcare cost barrier through leadership and cross-department coordination. CVC obstruction is directly related to patient safety and requires enhanced monitoring of relevant indicators. INTRODUCTIONA central venous catheter (CVC)—a type of central venous access device (CVAD)—is widely used to treat certain critical illness.1 A CVC is an indwelling device placed in a large vein (most commonly the internal jugular, subclavian, or femoral vein) for real-time hemodynamic monitoring, rapid fluid challenge, or infusion of hyperosmotic solutions.2 In the United States, approximately 5 million patients receive a CVC insertion each year.3 According to statistics from the National Health Insurance Administration, Ministry of Health and Welfare in Taiwan, the number of CVCs used in 2021 was 209,338.4
Occlusion of a CVC means that the patient cannot receive immediate treatment; it may also cause a catheter-related bloodstream infection (CRBSI), leading to septic shock or even death.5 Thus, it is critical to avoid CVC occlusion. CVC occlusion can be partial or complete.1 When partial occlusion occurs, drugs can still be administered, but blood cannot be aspirated from lumen. If the catheter is completely occluded, it needs to be removed and repositioned.6 One study showed that the average occlusion rate of a CVC ranges from 14% to 36%.5 Thus, CVC occlusion can be considered a common issue and is important for patient safety.
There are three main causes of CVC occlusion: mechanical, drugs, and clots, the last of which is the most common reason.7 To avoid the occlusion of CVCs, proper catheter flushing and locking are the primary interventions due to their ability to reduce blood reflux into the lumen.1 The Infusion Nurses Society suggests that hospitals should build a standard operating procedure (SOP) for flushing and locking a CVC. The SOP should include flushing solutions, flushing/locking timing specifications, and flushing techniques.8,9 In terms of flushing solutions, a single-dose vial or pre-filled syringe of preservative-free 0.9% sodium chloride or heparin can be used. Furthermore, the minimum flushed volume should be twice the internal volume of the catheter system. If the administered medication is incompatible with 0.9% sodium chloride, then the CVC should be flushed with 5% dextrose followed by 0.9% sodium chloride.9 With regard to flushing and locking timing, nurses should perform the flushing after each infusion or medication administration and then proceed to lock the lumen. In terms of flushing technique, the pulsatile flushing technique (PFT) may be effective in avoiding lumen occlusion. PFT is a multi-positive pressure-pushing technique that is considered more effective in reducing the build-up of materials such as blood clots or a protein layer on the lumen wall compared with conventional continuous flushing.10
OBJECTIVESThis aim of this project was to audit and decrease the CVC occlusion rate in acute care based on a JBI evidence summary. The specific objectives were to:
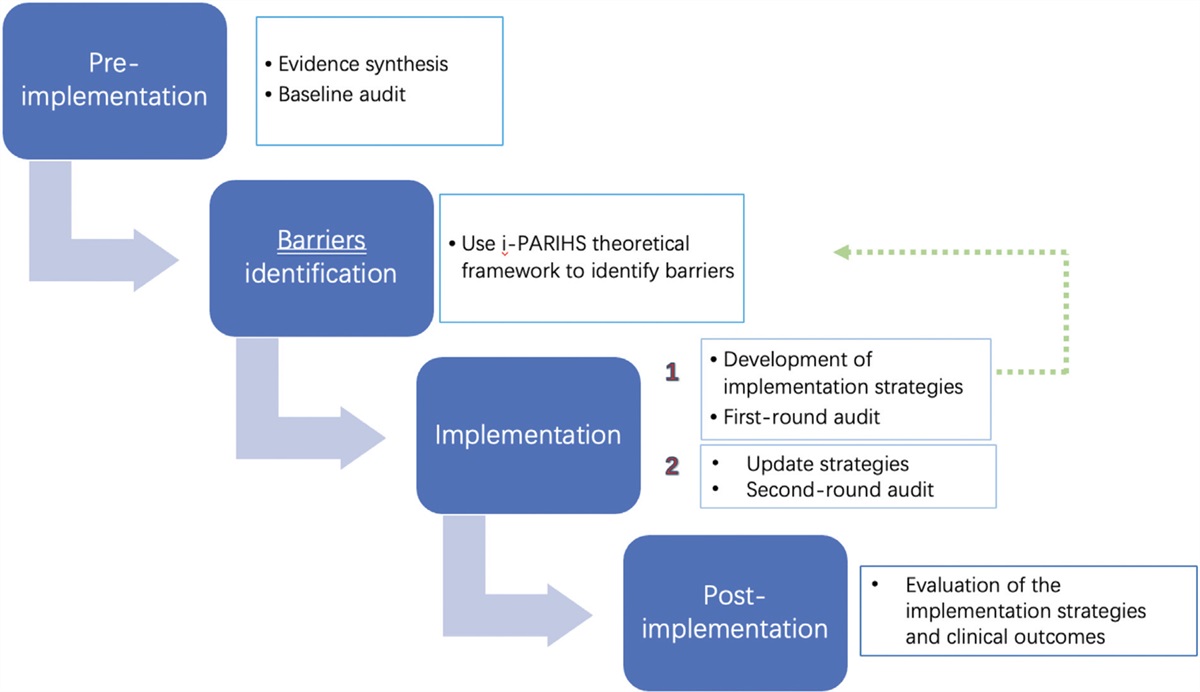
1. Determine current compliance with evidence-based criteria regarding flushing and locking management, an approach to maintain CVC patency in the ED and ICU. 2. Identify barriers and facilitators to achieve compliance with evidence-based criteria regarding flushing and locking management, an approach to maintain CVC patency in the ED and ICU. METHODSThis project used the JBI Evidence Implementation Framework, which involves an audit and feedback process and addressing barriers to compliance with recommended clinical practices in a structured manner.11 The framework consists of seven stages: identification of practice areas for change, engaging change agents, assessment of context and readiness to change, review of practice against evidence-based audit criteria, implementation of changes to practice, reassessment of practice using a follow-up audit, and consideration of the sustainability of practice changes.
The project activities involved three phases: (i) establishment of team members and conducting a baseline audit based on criteria derived from a JBI evidence summary; (ii) designing and implementing strategies to address non-compliance, informed by the baseline audit and JBI's Getting Research into Practice (GRiP) software; and (iii) in line with Deming's theory, a preliminary follow-up audit was conducted to assess changes in compliance. Based on the identified areas of non-compliance, strategies were developed and implemented to address these issues. Subsequently, a final audit was conducted to evaluate compliance and assess improvement in clinical practice.
This project was developed in the emergency department (ED) and adult intensive care unit (ICU) of the Hualien Armed Forces General Hospital (HAFGH), a regional military hospital with 377 beds in Eastern Taiwan. The ED has 8 beds with 10 nurses, and the adult ICU has 12 beds with 20 nurses. The sample consisted of 30 nurses, including all nurses in the ED and the adult ICU. Sepsis shock is the predominant diagnosis among patients (68%) in the ED and ICU. The total number of CVC insertions in the ED and adult ICU was 987, which accounted for 98% (987/1002) from 2021 to August 2022. However, the CVC occlusion rate in the ED and adult ICU was 33%.
Ethical considerationsThe project was registered as a quality improvement activity within the HAFGH Hospital. Upon review by the Medical Quality Committee of the HAFGH, ethical approval was not required. All data were obtained through retrospective medical record review in an anonymous manner.
Phase 1: Stakeholder engagement and baseline auditIn the first phase (September 19 to 30, 2022), we established a quality improvement team for the ED and adult ICU. The team identified the setting and sample size for conducting a baseline audit (pre-implementation audit). The audit criteria were based on an evidence summary developed by JBI.12
Establishment of the project team. The project team comprised a nursing supervisor who is a professor, four directors (ED, adult ICU, Nursing Department [ND], and Department of Medical Supplies [DMS]), two head nurses (ED and adult ICU), and one nurse (quality team leader of ED). We considered that the military rank of the team members would influence the success of this project, so we included directors who were colonels. Each team member had sufficient experience in managing critically ill patients to provide an expert opinion on potential implementation strategies, participated actively in the project, and influenced the unit's policy decisions. The nursing supervisor served as the team co-leader and was responsible for project coordination, organizational leadership, facilitating communication, data analysis, and writing protocols and reports. The directors of the ED and adult ICU were responsible for the consultation between the two units and the unified strategies. The head nurses of the ED and adult ICU were responsible for educational programs and training in the units. One nurse assisted in data collection. All team members also performed the baseline, 1-month post-implementation, and post-implementation audits of the project. Due to the COVID-19 pandemic, the project team leader conducted two weekly virtual meetings using Google Meet or Line (a remote communication software application in Taiwan).
Audit criteria and conducting the baseline audit. The JBI evidence summary lists seven audit criteria for CVC flushing and locking management.12 The project team adopted six of the seven criteria, based on an evaluation of the feasibility of these criteria in nursing practice and cultural factors in Taiwan (Table 1). The criterion, “the CVAD lumen was flushed after each infusion” was excluded because it is not applicable to Taiwan's clinical practice. From September 19 to 23, 2022, baseline audit criteria data were collected by the team through direct observation of 30 nurses. After the audit was completed, the data were entered into the JBI Practical Application of Clinical Evidence System (PACES).
Table 1 - Audit criteria, sample, and method for measuring compliance with best practice Audit criterion Sample Method used to measure compliance with best practice 1. The organization has a standardized flushing and locking solution protocol. Baseline: SOPCVAD, central venous access device; PFT, pulsatile flushing technique.
We presented the baseline audit to the project team using the JBI Getting Research into Practice (GRiP) tool and discussed potential barriers and opportunities for improving compliance with the audited criteria. This phase lasted from October 1 to November 11, 2022 (11 weeks). Based on Deming's theory,13 we used the PDSA (Plan-Do-Study-Act) concept to design our interventions, aiming for continuous improvement by implementing corrective actions for any criteria that were not met.
The baseline audit findings were presented to all nurses in the ED and ICU. The discussion was conducted according to the JBI GRiP framework, which involves identifying perceived barriers, potential strategies for improvement, and the necessary resources. The GRiP framework was applied to each audit criterion separately, and then consolidated to avoid redundancy and increase effectiveness. One month later, the team conducted the first follow-up audit (October 24 to 31, 2022). For criteria that were still not being fully adopted, the team identified previously unidentified barriers through verbal questioning of the nursing staff and formulated additional strategies to address these issues.
Phase 3: Follow-up auditThe second follow-up audit was conducted using the same criteria as the baseline audit, and took place from January 9 to 16, 2023 (10 weeks after the baseline audit).
DATA ANALYSISData on changes in compliance were measured using JBI PACES in the form of percentage changes from baseline. The CVC occlusion rate was calculated through retrospective review of medical records.
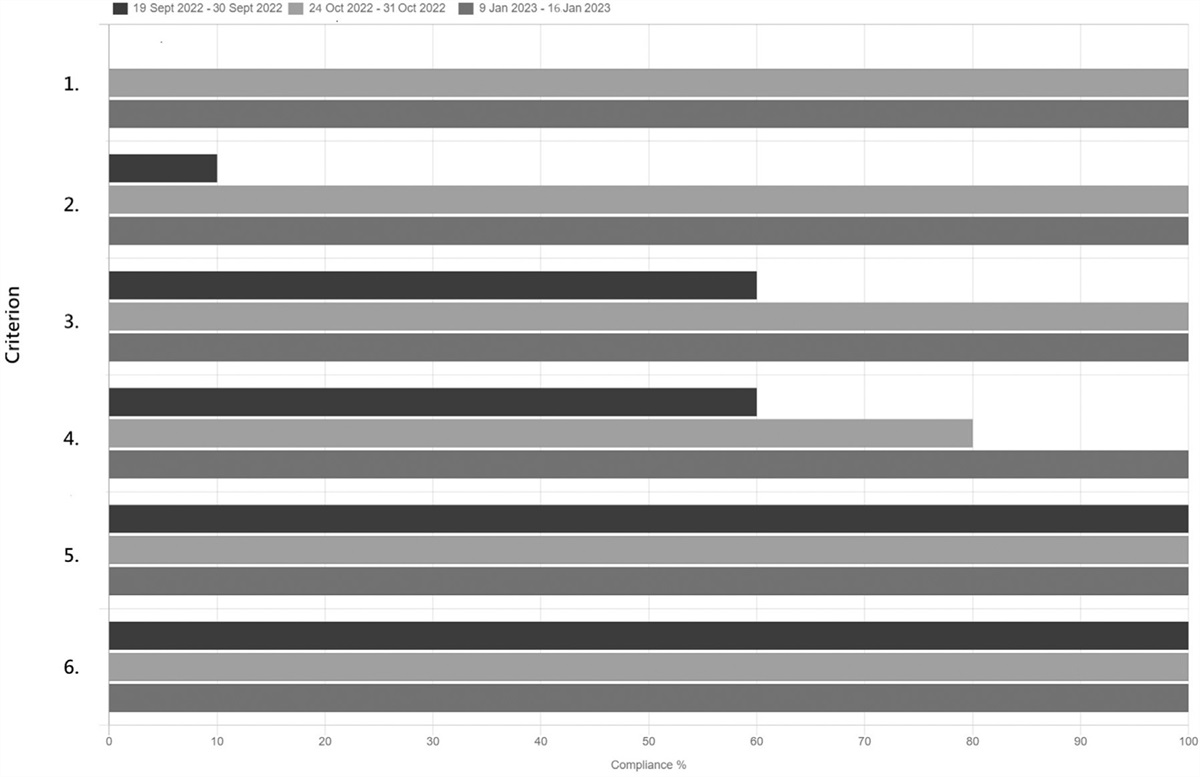
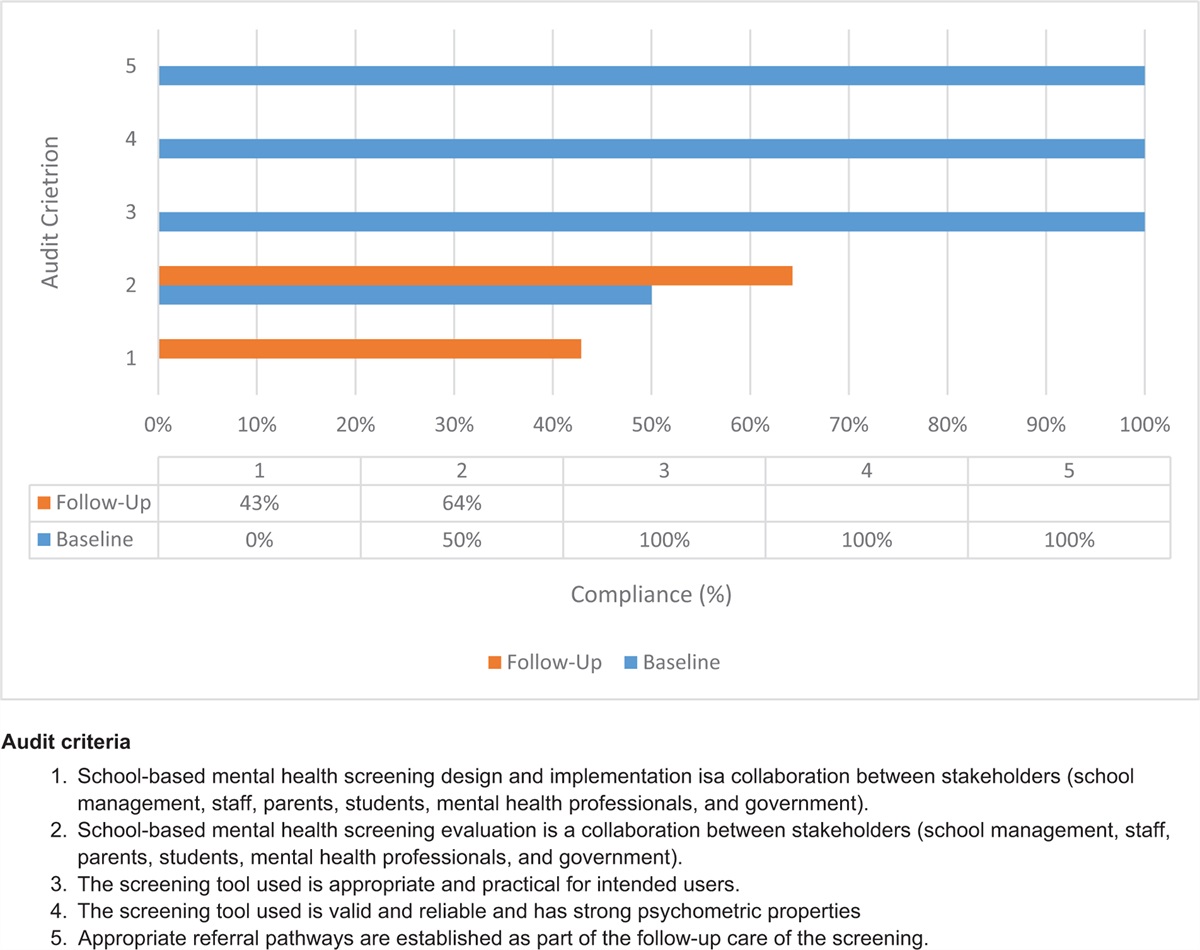
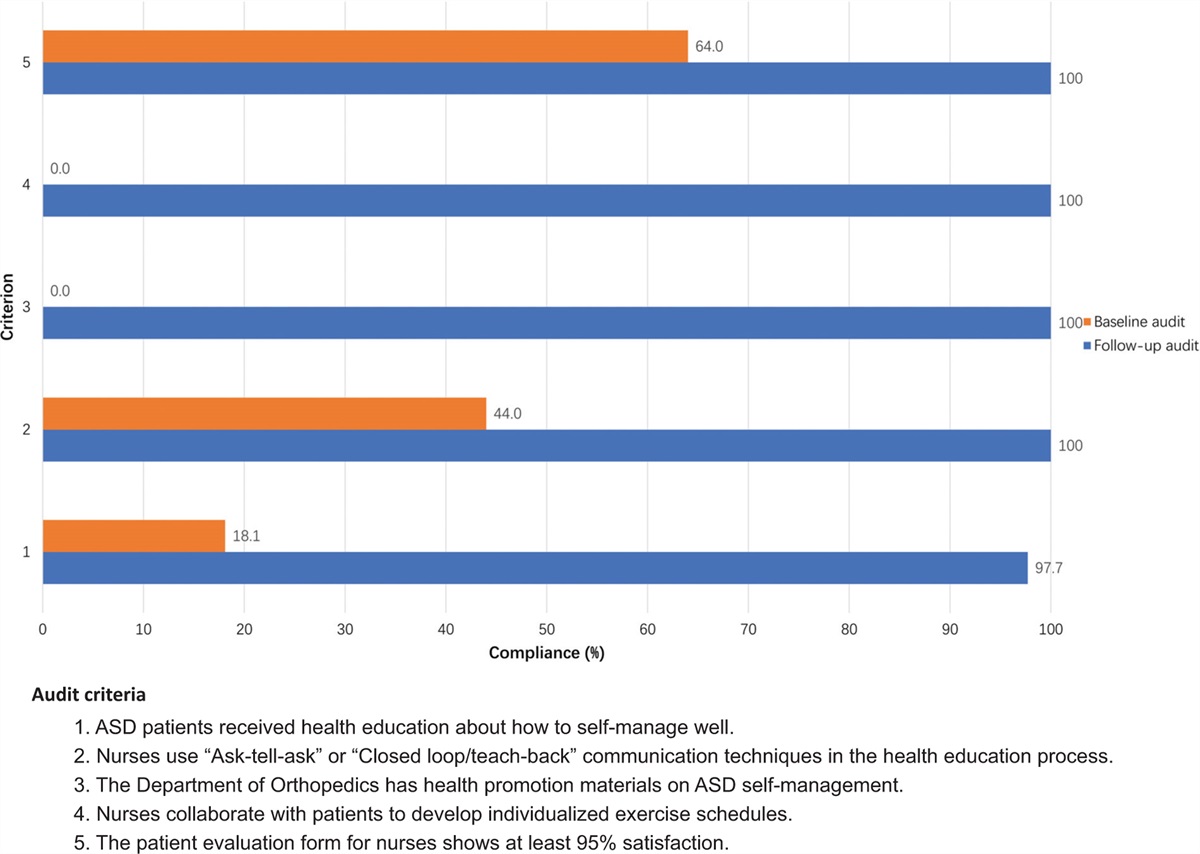
RESULTS Phase 1: Baseline auditThe team utilized audit forms to assess nurses’ adherence to the audit criteria. Of the six criteria, Criteria 5 and 6 showed excellent compliance (100%). For Criterion 1, the hospital's CVC SOP included only the need to flush a CVC line with normal saline but did not provide clear guidelines on the flushing time, PFT, or locking procedures, resulting in a compliance rate of 0%. For Criterion 2, only 10% of the nurses (n = 3) locked the catheter after final medication administration. For Criterion 3, 40% of the nurses (n = 12) did not use the single-dose system for locking the CVAD. In addition, for Criterion 4, 40% of the nurses (n = 12) did not meet the criteria. Among them, seven performed CVC flushing without PFT, three did not perform CVC flushing, and two used norepinephrine medication in the line and flushed it only with 5% glucose. Figure 1 shows the audit results for the six audit criteria used in the baseline audit.
 Figure 1:
Figure 1: Compliance (%) with best practice audit criteria in the baseline, first follow-up, and final follow-up audits.
Phase 2: Design and implementation of strategies to improve practiceDuring the second phase (October 1 to November 11, 2022), the project team engaged in discussions and incorporated ideas to validate the three barriers identified in the baseline audit. The team developed change strategies based on the GRiP framework, and resources were allocated to overcome these barriers (Table 2). The strategy was to modify the CVC SOP to address Barrier 1 in the table. The team referred to the JBI evidence summary to review the hospital's existing CVC SOP and identified the missing components:
(1) Flushing solution: The 0.9% normal saline was used to flush the CVC lumen. When medications were not compatible with 0.9% normal saline, 5% glucose was used for flushing, followed by saline 0.9% normal saline for flushing. (2) Flushing timing: Flushing the CVC lumen after the last administration of medication and performing routine flushing of the CVC lumen every shift and securing it with a single-use lock. (3) Flushing technique: Using a PFT for flushing the CVC lumen. Table 2 - Getting Research into Practice matrix Barriers Strategies Resources Outcomes 1. Lack of SOP for flushing and locking management for CVCs (Criterion 1) • Modification of CVC SOPCVC, central venous catheter; ED, emergency department; ICU, intensive care unit; ND, nursing department; OCSE; objective structured clinical examination; PFT, pulsatile flushing technique; SOP, standard operating procedure.
After completing the revision of the SOP, the directors and nursing leaders of the ED and ICU reviewed its feasibility. The ND Director conducted the final review and approved the revised SOP. To overcome Barriers 2 and 3, the team designed an education program on CVC flushing and locking management. Prior to the class, we administered a ten-item online questionnaire designed to fit the educational program to all nurses, with a total score of 100. The mean pre-test score was 60. Additionally, we used dyed water as the flushing solution and determined that the correct operation rate of the PFT by nurses was 20%. We then conducted an education program that comprised the flushing solution, flushing timing, and PFT and incorporated instructional videos on YouTube for classroom lectures. After completing the program, we asked all nurses to complete the online questionnaire and to repeat the PFT. The post-test mean score was 100 and the correct operation rate of the PFT was 100%.
To address Barrier 3, which is a complex and time-consuming process of preparing materials for flushing a CVC using traditional methods, the team purchased pre-filled saline syringes. We conducted a cost analysis using the traditional method, which includes empty syringes, sterile saline, and pre-filled saline syringes. After several meetings with procurement officers from the ER, ICU, and ND, it was determined that the price difference was too large, resulting in opposition to the use of pre-filled syringes. To achieve our procurement goal, that is, reduce the cost difference, the team included the cost of nurse operating time and cost of additional blood draws or peripheral intravenous catheterization due to CVC occlusion (Appendix, https://links.lww.com/IJEBH/A141). In addition, owing to the hierarchical nature of military organizations, we recognized the need to involve higher-level decision makers. Therefore, we proposed this procurement issue at a hospital-level meeting and negotiated with the directors of the ER, ICU, ND, and DMS. This ensured we successfully reached our procurement goals.
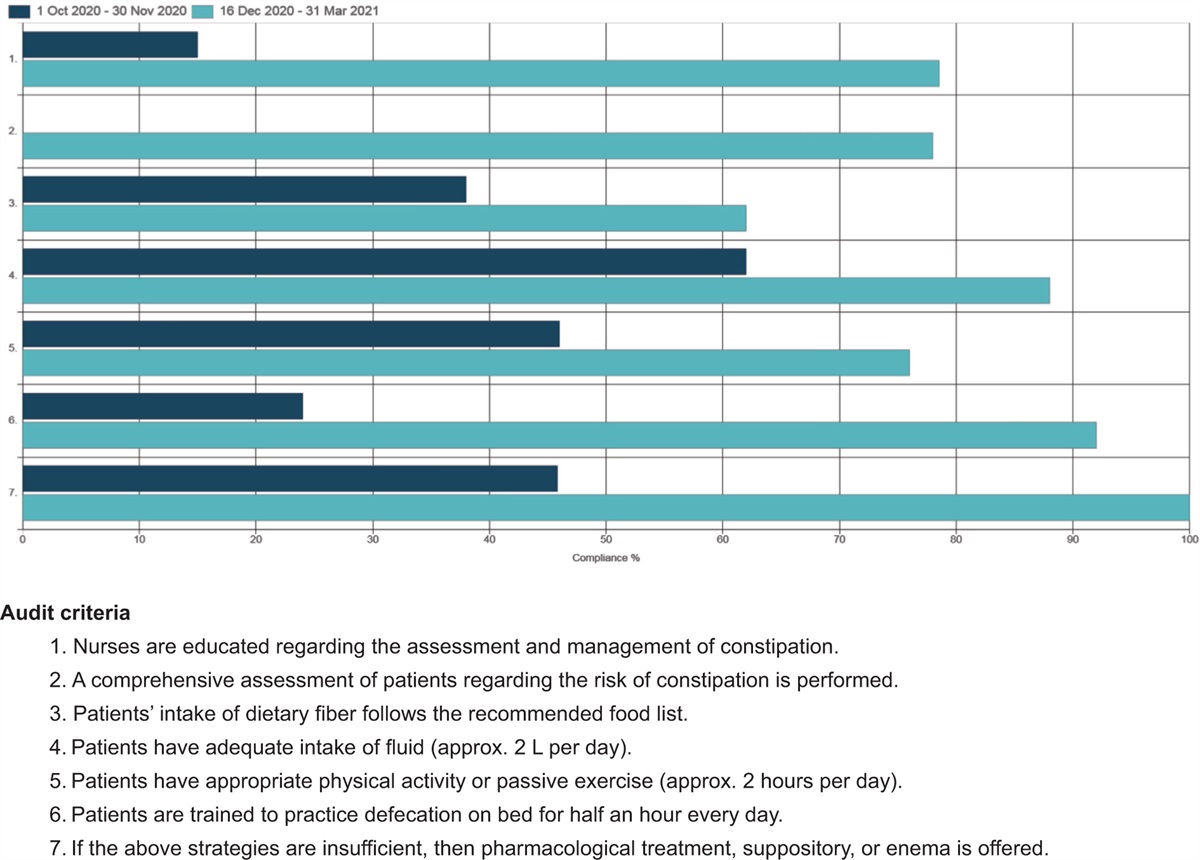
Phase 3: Follow-up auditThe first post-implementation audit results were evaluated from October 24 to 31, 2022. Thirty nurses in the ED and adult ICU demonstrated 100% compliance, except for Criterion 4. This criterion increased to 80%; however, some nurses (n = 6) still did not execute the flushing and locking procedure properly. Through verbal inquiry, we learned that the preparation of flushing tools was too complicated and time-consuming. Therefore, we proposed the purchase of pre-filled saline syringes. The final post-implementation audit results were evaluated from January 9 to 16, 2023, eventually achieving 100% compliance (Figure 1). Moreover, we monitored the occlusion rate of CVCs and found that, after the project was implemented (October 1, 2022 to January 9, 2023), the average occlusion rate of CVCs decreased from 33% (2021 to August 2022) to 5% (Figure 2).
 Figure 2:
Figure 2: Occlusion rate of CVCs (%).
DISCUSSIONCVC insertion is a common medical procedure in clinical practice and the quality of CVC care is highly valued by the Taiwanese government. However, much of the focus has been on preventing CRBSI, instead of occlusion of CVCs. Our data showed that nearly 30% of patients required additional venipuncture or peripheral venous catheterization due to CVC occlusion. This project used the JBI evidence implementation framework to improve the clinical CVC occlusion rate. We modified the hospital's CVC SOP and incorporated related education and training into annual training plans for the nurses. We also included Objective Structured Clinical Examination (OSCE) training to ensure that the nurses could correctly perform the PFT. As a result, the nurses’ compliance with all criteria reached 100%, and the CVC occlusion rate was reduced from 33% to 5%.
During the project implementation, we faced some challenges. One of the challenges was the time-consuming process of traditional flushing preparation. However, the cost of pre-filled saline syringes was much higher than the traditional method, making procurement difficult. We conducted a cost analysis and included the cost of additional peripheral venous catheterization and empty syringes due to CVC occlusion in the patient fee. With the help of department heads and effective communication with stakeholders, we were able to successfully procure pre-filled saline syringes, which was one of the key factors in the successful implementation of this project. The second challenge was that some night shift nurses were unable to participate in on-site training education. To overcome this, we used an e-learning approach. Thirdly, when performing PFT, it was initially difficult to evaluate whether the nurses were performing the procedure correctly when using normal saline. Therefore, we added red dye to the saline solution, which allowed us to clearly observe the effect of needle injection during PFT execution.
The literature demonstrates that implementing standardized protocols for CVC flushing and locking can effectively reduce the incidence of CVC occlusion,12,14 which aligns with the results of our project. Regarding the choice of flushing solution, while some studies suggest the use of low molecular weight heparin,15,16 we opted to use normal saline considering the cost implications in our hospital.
Maintaining the patency of the CVC is very important, and guidelines must be followed for pre-implantation preparation, site selection and care, routine care, and flushing and locking; otherwise lumen occlusion or CRBSI can easily occur.17 There have been other CVC-related projects published in the past. Ferreira et al. studied recommendations on CVC insertion, such as hand hygiene, CVC placement, and ultrasound-assisted placement.18 Hsieh et al. reported on CRBSI reduction, including routine care interventions for CVAD.19 Our project focused on the flushing and locking management part of CVC care. The project showed that correctly implemented evidence-based practices effectively improve the patency of CVCs, thereby reducing the incidence of CVC occlusion. The hospital includes the CVC occlusion rate as one of the medical quality indicators of the ED and adult ICU, and continues to monitor and track it.
CONCLUSIONSThe CVC is the most frequently used vascular device in clinical settings. Through effective leadership and cross-departmental collaboration, together with the design of an innovative PFT education program, it was possible to effectively enhance the knowledge and compliance of nurses in CVC flushing and locking management. The project achieved 100% compliance for all six criteria. Ultimately, we significantly reduced the hospital's CVC occlusion rate. We hope to promote this routine to other CVADs, such as the peripherally inserted central catheter (PICC) or double lumen, as well as other critical care units within the hospital, such as the anesthesia department and the neonatal ICU. Furthermore, the authors hope that this project's success will bring attention to the issue of CVC occlusion and encourage government agencies to prioritize this issue.
ACKNOWLEDGMENTSThe authors extend their appreciation to all nurses in the ED, the adult ICU, ND, and all managers of the HAFGH. The success of our project was based on active participation. The authors are grateful to Prof. Heng-Hsin Tung for assistance with writing this article.
AUTHOR CONTRIBUTIONSCHF, FHC, and HHT contributed to the conceptualization and design of the project. CHF and CNC coded and analyzed the data. CHF and HHT drafted the initial manuscript. All authors participated in the interpretation of the data, and review and revision of the manuscript. All authors approved the final version of the manuscript prior to submission.
REFERENCES 1. Zhong L, Wang HL, Xu B, Yuan Y, Wang X, Zhang YY, et al. Normal saline versus heparin for patency of central venous catheters in adult patients: a systematic review and meta-analysis. Crit Care 2017; 21 (1):5. 2. O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, Let al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 2011; 52(9):e162-93. 3. Swaminathan L, Flanders S, Horowitz J, Zhang Q, O’Malley M, Chopra V. Safety and outcomes of midline catheters vs peripherally inserted central catheters for patients with short-term indications: a multicenter study. JAMA Intern Med 2022; 182 (1):50–58. 4. Administration NHI. 2022 Medical project medical order filing volume. In: Welfare MoHa, ed; 2022. 5. Baskin JL, Pui CH, Reiss U, Wilimas JA, Metzger ML, Ribeiro RC, et al. Management of occlusion and thrombosis associated with long-term indwelling central venous catheters. Lancet 2009; 374 (9684):159–169. 6. Milani A, Mazzocco K, Gandini S, Pravettoni G, Libutti L, Zencovich C, et al. Incidence and determinants of port occlusions in cancer outpatients: a prospective cohort study. Cancer Nurs 2017; 40 (2): 7. van Miert C, Hill R, Jones L. Interventions for restoring patency of occluded central venous catheter lumens. Cochrane Database Syst Rev 2012; 2012 (4):Cd007119. 8. Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, et al. Infusion therapy standards of practice. 8th ed. J Infus Nurs 2021; 44: (1S Suppl 1): S1–S224. 9. López-Briz E, Ruiz Garcia V, Cabello JB, Bort-Martí S, Carbonell Sanchis R, Burls A. Heparin versus 0.9% sodium chloride locking for prevention of occlusion in central venous catheters in adults. Cochrane Database Syst Rev 2018; 7 (7):Cd008462. 10. Ferroni A, Gaudin F, Guiffant G, Flaud P, Durussel JJ, Descamps P, et al. Pulsative flushing as a strategy to prevent bacterial colonization of vascular access devices. Med Devices (Auckl) 2014; 7:379–383. 11. Porritt K, McArthur A, Lockwood C, Munn Z. JBI's approach to evidence implementation: a 7-phase process model to support and guide getting evidence into practice. JBI Evid Implement 2023; 21 (1):3–13. 12. Porritt K. Central venous access device (adult, pediatric and neonates): flushing and locking catheter lumens to maintain patency. JBI EBP Database 2023; JBI-ES-1613-5. 13. Reid RA, Koljonen EL, Bruce Buell J. The Deming Cycle provides a framework for managing environmentally responsible process improvements. Qual Eng 1999; 12 (2):199–209. 14. Conway MA, McCollom C, Bannon C. Central venous catheter flushing recommendations: a systematic evidence-based practice review. J Pediatr Oncol Nurs 2014; 31 (4):185–190. 15. Pelland-Marcotte MC, Amiri N, Avila ML, Brandão LR. Low molecular weight heparin for prevention of central venous catheter-related thrombosis in children. Cochrane Database Syst Rev 2020; 6 (6):Cd005982. 16. Lin PT, Wang SH, Chi CC. Low molecular weight heparin for prevention of microvascular occlusion in digital replantation. Cochrane Database Syst Rev 2020; 4 (4):Cd009894. 17. Practice Guidelines for Central Venous Access 2020: an updated report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiol 2020; 132 (1):8–43. 18. Ferreira JDN, dos Santos KB, Siqueira EC, Gomes EP, Martini L, Fraga JBP, et al. Central venous catheter insertion in adult patients: a best practice implementation project. JBI Evid Implement 2021; 19 (3):296–305. 19. Hsieh HC, Hsieh CC, Chen TY, Cheng CH, Mu PF, Chow LH, et al. Decreasing the incidence of central line-associated bloodstream infection in a medical intensive care unit: a best practice implementation project. JBI Evid Implement 2023; 10:1097.
留言 (0)