
記住我

What is already known
Dysphagia is a common and life-threatening comorbidity in acute stroke patients. Aspiration pneumonia is the leading cause of mortality in post-stroke dysphagia patients. Early dysphagia screening can decrease not only pneumonia but also mortality, dependency, and length of stay in stroke patients.What this paper adds
Key barriers included the lack of a standardized protocol and training for dysphagia screening, leading to gaps in the quality of dysphagia screening. Education sessions with a standardized dysphagia screening protocol promoted compliance with best practices. Team and leadership support provided effective help in implementing improvement strategies. INTRODUCTIONStroke is a neurological condition characterized by a sudden, non-convulsive loss of function due to brain ischemia or intracranial hemorrhage. A nationwide community-based study, NESS-China, indicated that ischemic stroke accounts for approximately 70% of all incident stroke cases, with intracerebral hemorrhage accounting for 24%, subarachnoid hemorrhage accounting for 4%, and undetermined or other types accounting for the remaining 2% of cases.1 Stroke is the second leading cause of death worldwide and the leading cause of death in China, with over 2 million new cases occurring annually in China.2 The burden of disease is expected to increase further as a result of the aging population and the ongoing high prevalence of risk factors, such as hypertension, diabetes, smoking, lack of exercise, and inadequate management.3 With improved access to overall health services, stroke mortality was generally stable or even slightly decreased from 1985 to 2013, despite the increase in incidence.1 Although survivors usually have different functional disabilities, dysphagia is one of the most common and life-threatening comorbidities associated with acute stroke.
Dysphagia refers to difficulty in swallowing, and can be classified into two distinct types: oropharyngeal dysphagia and esophageal dysphagia. Stroke is closely linked to oropharyngeal dysphagia, affecting 29% to 81% of acute stroke patients.4 Although many stroke patients recover from swallowing within the first weeks after the onset of stroke, 11% to 50% can still suffer from dysphagia up to 6 months after stroke.5 Dysphagia can increase the risk of complications, such as aspiration pneumonia, dehydration, and malnutrition, thus leading to increased mortality, disability, length of hospital stay, financial burden, and poor quality of life in stroke patients.6
Aspiration pneumonia due to dysphagia is one of the leading causes of mortality in post-stroke patients.7 Patients who experience dysphagia are approximately five times more likely to develop pneumonia than those without dysphagia.8 Dysphagia screening in stroke patients is therefore critical to prevent adverse outcomes, such as pneumonia, longer hospital stay, dependency, and increased mortality.9,10 Clinical practice guidelines on stroke recommend that patients should be screened for dysphagia as soon as possible after hospital admission.11-13 However, a cross-sectional study of 965 nurses showed that only 36.52% of stroke patients were screened based on guidelines after hospital admission in China14 because of poor knowledge and attitudes of the nurses. Nurses who are available to patients 24 hours a day in the hospital are in a prime position to screen and identify patients with swallowing or deglutition disorders so that early interventions can be provided. Training nurses in dysphagia screening can effectively lower the risk of chest infections and death.15
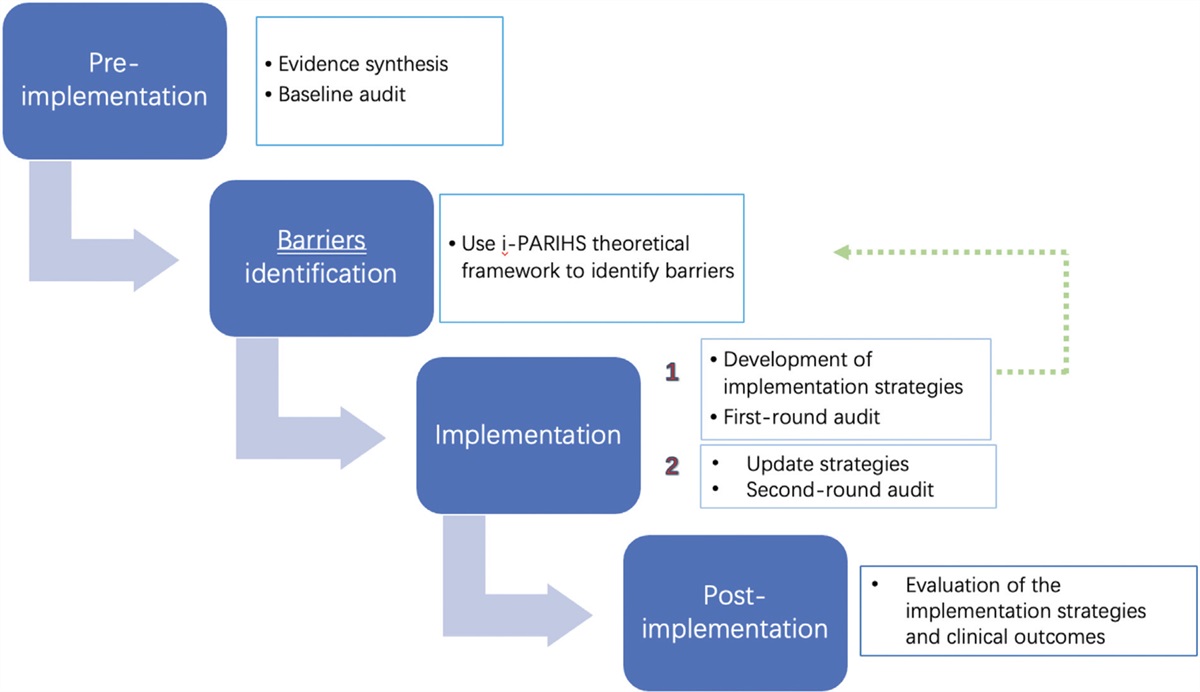
In the Neurology Ward of Zhongshan Hospital of Fudan University, China, dysphagia screening is conducted by nurses; however, not all patients with stroke are screened for dysphagia, which may potentially increase the number of complications related to dysphagia. This specific clinical area was chosen as the focus of the current implementation project, not only due to a lack of awareness regarding dysphagia screening among nursing staff, but more importantly, to improve patient outcomes. However, translating research evidence into clinical practice can be challenging. To assist with this process, the JBI Evidence Implementation Framework was used to guide this project and the JBI Practical Application of Clinical Evidence System (JBI PACES) was used to conduct baseline and follow-up audits.
OBJECTIVESThis project aimed to promote evidence-based dysphagia screening among stroke patients, thus improving the clinical outcomes of patients and the knowledge and practice behaviors of nurses.
The specific objectives were to:
1. Determine compliance with best practice recommendations in the Neurology Department. 2. Develop strategies to address areas of low compliance with best practice recommendations. 3. Implement strategies that promote best practice and align with the FAME (Feasible, Appropriate, Meaningful, and Effective) approach. 4. Measure changes in clinical practice related to dysphagia screening through a follow-up audit. ETHICSThe project was registered as a quality improvement initiative at the hospital; therefore, ethical approval was not required. However, the project ensured confidentiality and anonymity of patients. All patients involved in the project were informed that their records would only be used as data for the project, and informed consent was obtained.
METHODSThe project was conducted in the Neurology Department, Zhongshan Hospital, Fudan University, Shanghai, China. There are 16 beds in the neurology ward for stroke patients. Approximately 50 patients with stroke are admitted each month. The inclusion criteria were patients aged 18 years or above who were diagnosed with stroke, determined by checking medical records. The exclusion criteria included patients who were unable to complete a dysphagia screening test independently (e.g., patients with cognitive impairment or movement disorders). The period of the baseline audit coincided with the COVID-19 pandemic, and fewer patients were admitted to hospital than previously; therefore, the duration of the baseline audit was longer than the follow-up audit. The neurology ward is run by a head nurse, with 22 nursing staff providing direct care to stroke patients. The JBI Evidence Implementation Framework was used to provide authoritative methodological guidance for the project.16 The JBI framework is grounded in the audit and feedback process, along with a structured approach to identifying and managing barriers to compliance with recommended clinical practices. The framework consists of seven phases.
Phase 1: Identification of practice area for changeDysphagia can cause severe outcomes in patients with stroke; however, not all patients with stroke undergo dysphagia screening in the neurology ward.14 After discussions with the nursing manager and head nurse, dysphagia screening for all stroke patients was selected as a practice area for improvement.
Phase 2: Engaging change agentsAll relevant stakeholders, including project team members, physicians, nursing staff, and patients were considered to be change agents. The project team consisted of six members: one nurse manager, one head nurse, and four clinical nurses. This team was involved in promoting the implementation of the project.
The project team was led by Guojing Shen, who was responsible for protocol writing, data analysis, and report writing. Nurse manager Ying Wang was responsible for process control. The head nurse, Jue Wang, was responsible for project coordination and supervision. Nurses Qingyi Xia, Xiaoling Zhang, and Ping Xue were responsible for data collection. All team members were engaged in scheduling and developing strategies and helping to implement them to improve dysphagia screening. The nursing staff were engaged in planning and reviewing strategies and were responsible for implementing dysphagia screening for stroke patients. The results of the screening were reported to physicians for subsequent measures.
Phase 3: Assessment of context and readiness to changeA team session was held to present the aims of the project, review the project stages, inform stakeholders about the best practice recommendations, and specify individual responsibilities in the project. Feedback was obtained from stakeholders for each item. Furthermore, we reached consensus with the manager and staff about the feasibility of probable changes in practice, their commitment to change, and the availability of resources to support implementation.
According to a preliminary investigation, there were three favorable conditions to support implementation: eight nurses with more than 10 years of work experience in the neurology ward; a validated tool used in the ward; and some nurses who had undergone prior training.
Phase 4: Review of practice against evidence-based audit criteriaFrom May 4 to June 30, 2022, a baseline audit was conducted involving a group of 22 nurses and 48 patients. This audit identified the difference between current practice and best practice recommendations based on clinical guidelines related to dysphagia screening in stroke patients. The baseline audit criteria were derived from the best evidence.13,17,18Table 1 shows the audit criteria, sample size, and the methods used to measure compliance.
Table 1 - Audit criteria, audit guide, sample, and method used to measure compliance Audit criterion Audit guide Sample Method used to measure compliance with best practice Dysphagia screening is conducted by a trained health care professional. • “Yes” if nurse received training.A checklist was created to help conduct the audits. Three nurses on the project team were responsible for data collection and marking Yes, No, or N/A on the checklist. In addition, a questionnaire with robust psychometric properties was administered to survey nurses’ knowledge, attitudes, and behaviors toward dysphagia screening in the baseline and follow-up audits, respectively.19
Phase 5: Implementation of changes to practiceIn July 2022, one team session lasting approximately 2 hours was held, using the JBI Getting Research into Practice (GRiP) framework to reflect on the baseline audit results and identify perceived barriers, potential improvement strategies, and the resources required. The project team compared baseline audit findings against best practice recommendations to identify barriers to screening implementation. Semi-structured interviews were also conducted with five nurses by the project leader to explore barriers. Finally, three action strategies were developed: (1) selection of validated tools (reviewing evidence-based research and organizing a team session); (2) provision of training for nurses (i.e., educational slides and training sessions); and (3) development of a standardized dysphagia screening protocol and checklist. Each action strategy took around a week to implement.
Phase 6: Re-assessment of practice using a follow-up auditFrom August 1 to September 10, 2022, the follow-up audit was carried out with a group of 19 nurses and 48 patients. The same evidence-based criteria were used as in the baseline audit. However, since two nurses had been rotated to other wards and one was on sick leave, there were three less nurses than in the baseline audit. Follow-up audits were performed by the same nurses who collected the baseline data. Both baseline and follow-up data were entered into the JBI PACES program to compare compliance at the two stages.
Phase 7: Consideration of the sustainability of practice changesA second follow-up audit 12 months after the initial follow-up audit was considered to assess sustainability. Some interventions can be used to maintain project sustainability. For instance, regular training sessions will increase the number of trained staff, which will ensure that dysphagia screening criteria are met. Moreover, regular supervision and competency assessment by the head nurse will ensure the implementation quality of dysphagia screening.
ANALYSISThe data collected for this project were entered into Microsoft Excel. Statistical analyses were performed using SPSS 22.0. To compare the quantitative variables between the baseline and follow-up audits, we used the t-test when normal distribution was observed. The data were considered statistically significant at p < 0.05.
RESULTS Implementation planningBefore implementing this project, some of the nursing staff were trained on knowledge of dysphagia to reduce the training pressure on nurses. The head nurse promoted coordination among team members. Furthermore, the JBI Evidence Implementation Training Program was used to provide systematic knowledge on how to implement evidence-based practice. All these preparations ensured the smooth implementation of the project.
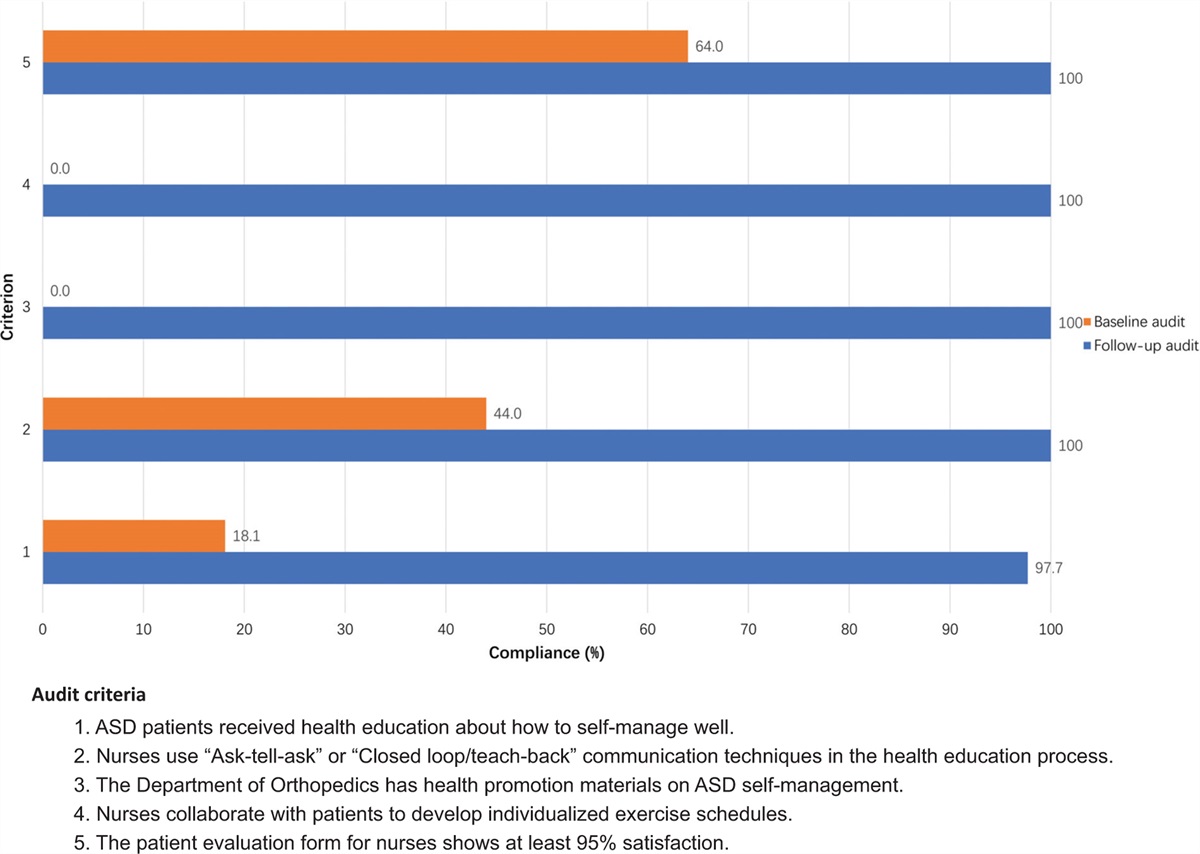
Baseline assessment and implementationThe baseline audit was undertaken from May 4 to June 30, 2022, involving 22 nurses and 48 patients. Medical records were reviewed for Criteria 2, 3, and 4, while interviews with nurses were used to obtain data for Criterion 1. It should be noted regarding Criterion 4 that if screening is not conducted upon admission after checking medical records, nurses need to interview patients or caregivers if screening is conducted before giving any oral food, fluid, or medication. At baseline, compliance with Criterion 2 (Dysphagia screening is conducted using a validated screening tool) was 100% because of the validated tool already being used before the audit. The compliance rate for Criterion 1 (Dysphagia screening is conducted by a trained health care professional) was 72.7%. For both Criterion 3 (Dysphagia screening is conducted as soon as possible after hospital admission [within 4 hours]) and Criterion 4 (Dysphagia screening is conducted before giving any oral food, fluid, or medication), compliance was 20.8%.
Following the baseline audit, combined with the results of the questionnaire survey and interview, the project team held one session to identify barriers and develop strategies to overcome barriers. The analysis of barriers demonstrated educational and organizational factors that hindered compliance with best practice. The baseline questionnaire survey indicated that nurses’ knowledge and attitudes toward dysphagia were unsatisfactory, resulting in a low compliance rate for dysphagia screening. At the organizational level, based on the results of semi-structured interviews, some nurses were skeptical about the validity of the Water Swallowing Test (WST), stating that screening results varied between two consecutive tests. They were concerned that this discrepancy may result in a false sense of security. The GRiP analysis conducted in this project is presented in Table 2. The results of the questionnaire survey are presented in Table 3.
Table 2 - Getting Research into Practice (GRiP) analysis Barrier Strategy Resources Outcomes Lack of knowledge and awareness of dysphagia screening. • Provision of training sessions for nursing staff about dysphagia screening. • Dysphagia screening literature.To address the identified barriers, the following strategies were implemented.
Validated tools for screening dysphagia: To address nurses’ concerns regarding the validity of the screening tool, the project leader conducted an in-depth review of evidence-based research and made a PowerPoint presentation about the content of different dysphagia screening tools. The PowerPoint presentation was then shown to the team to examine the varying validated tools. Finally, the team members agreed that the WST should be retained, but combined with simultaneous oxygen saturation monitoring to predict dysphagia risk. A pulse oximeter is a sensitive tool that can monitor silent aspiration when oxygen saturation decreases by more than 3%.20
Development of a standardized dysphagia screening protocol and checklist for swallow screening: The project team developed a standardized dysphagia screening protocol. Upon admission, stroke patients were asked to swallow 30 mL of water without disruption and passed if possible while their oxygen saturation was monitored in a sitting position at the same time. Patients were observed for signs of choking during swallowing and a “wet voice” after swallowing. If oxygen saturation declined by more than 3% or if the WST scores ranged from 2 to 4 points, the patients were asked to swallow four types of liquids with different viscosities to evaluate the safety and effectiveness of swallowing. Based on the protocol, a checklist was created to guide the screening implementation.
Provision of training for all nursing staff: A PowerPoint presentation was developed by the project leader. It included information on the anatomy and physiology of swallowing as well as dysphagia prevalence, types, complications, screening tools, and screening protocol.
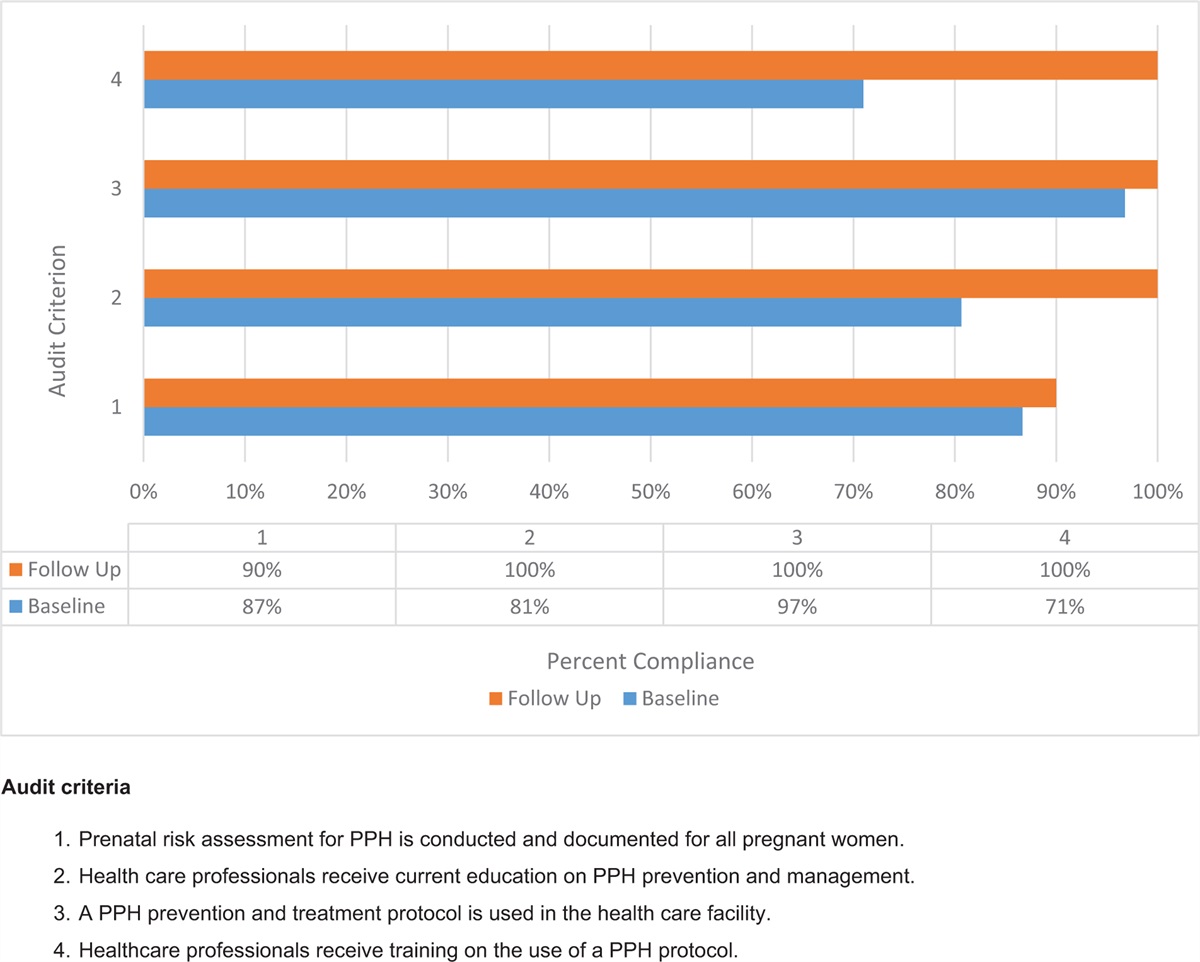
Impact evaluation and sustainabilityA follow-up audit was carried out from August 1 to September 10, 2022, using the same audit criteria as in the baseline audit and involving a group of 19 nurses and 48 patients. Figure 1 shows the results of the follow-up audit compared with the baseline audit. The results of the follow-up audit showed a 100% compliance rate for Criterion 1 (Dysphagia screening is conducted by a trained health care professional). For Criterion 3 (Dysphagia screening is conducted as soon as possible after hospital admission [within 4 hours]) and Criterion 4 (Dysphagia screening is conducted before giving any oral food, fluid, or medication), the compliance rate was 97.9% For Criterion 2, as the WST was already in use as a screening tool, the compliance rate remained at 100%.
 Figure 1:
Figure 1: Compliance (%) with best practice for dysphagia screening in the baseline and follow-up audits.
DISCUSSIONThe aim of the project was to promote evidence-based practice regarding dysphagia screening in patients with stroke. After reviewing the baseline data, all the criteria needed to improve. Three barriers to compliance were identified and strategies were implemented. Ultimately, the project achieved improvements in compliance with all criteria, following an audit and feedback cycle. Compliance of Criterion 2 remained at 100% after project implementation, although the screening tools had changed. This was because the screening tools used before and after project implementation were all validated, and only one tool was added to further increase the validity of screening.
The baseline audit results revealed that compliance rates for best practice19 dysphagia screening were relatively poor. A similar study showed that the barriers that hindered swallow screening of stroke patients included lack of knowledge and attitude among staff, screening tools, and lack of paper reminders.21 Correspondingly, in our project, lack of knowledge and awareness, skepticism regarding screening tools, and lack of a standardized dysphagia screening protocol were identified as barriers to achieving best practice recommendations.
The baseline audit consisted of a questionnaire survey. Although the results demonstrated that most of the nurses had received training before, the knowledge scores were still relatively low. Thus, tailored educational materials were needed to improve the quality of training. The results also indicated that more than half of the nurses agreed that dysphagia screening should be conducted by physicians or speech language therapists, while the remaining nurses thought it was their duty to carry out dysphagia screening. However, physicians were not available outside weekdays, and speech language therapists were not present in the ward, indicating that early screening was usually performed by nursing staff. One study showed that dysphagia screening conducted by trained nurses could effectively lower the risk of chest infections and death.15 Therefore, an explanation of the importance and reasons for swallow screening should be offered to change attitudes of nursing staff toward dysphagia screening.
The project leader created educational slides based on a thorough review of the research. During the training session, nursing staff learned about dysphagia and how to perform screening using the checklist provided to them. Abnormal screening findings would be reported to a physician for further treatment. After the training, and nurses’ knowledge, attitude, and behavior scores for dysphagia screening increased compared with the baseline audit (Table 3). This was in line another evidence implementation project, which showed that education on dysphagia can increase nurses’ knowledge and skills.22
The results of the semi-structured interviews were important for identifying barriers. The interview results showed that two nurses were skeptical about the validity of the WST because the results of this test varied over two consecutive tests; thus, it could fail to identify patients at risk of dysphagia. A systematic review showed that there was no single swallow screening tool with both 100% sensitivity and specificity.5 The WST is a simple and validated bedside screening tool for aspiration in stroke patients,23 and oxygen saturation monitoring is time-saving; hence, the increased workload was almost negligible for nursing staff. In addition, the combination of the WST and oxygen saturation monitoring can improve psychometric properties,20,24,25 especially sensitivity, as false-negative results are much worse than false-positive results. If the swallow screening test fails to identify dysphagia, the patient will continue oral intake and may experience the aforementioned complications. Therefore, during the team session, it was agreed to combine the WST with simultaneous oxygen saturation monitoring to better predict aspiration risk. Because oxygen saturation monitoring was added to the screening tools, the WST was still used during project implementation, and the compliance rate for Criterion 2 (using validated tools) was still 100%.
Another barrier was the lack of a standardized dysphagia screening protocol. The results of the interview revealed that swallow screening was conducted only when the patients expressed that they had difficulty in swallowing water or food; therefore, the screening was not based on objective assessment by nursing staff. Consequently, a standardized screening protocol and checklist were needed to guide the screening procedure. The follow-up audit results demonstrated that the compliance rates for screening within 4 hours of admission and before giving any oral food, fluid, or medication improved from 20.8% to 97.9%. This indicates that a standardized protocol can help improve compliance.
This project had some limitations that should be considered. First, the sample size was small. At the planning stage of the study, we projected to compare the aspiration rate in the pre- and post-implementation stage; however, aspiration did not occur in any of the cases. In the future, as the sample size increases, we expect to observe positive effects on patient outcomes. Second, some stroke patients in the ward were from the emergency department, where there was no dysphagia screening procedure. Therefore, there was a high likelihood that patients admitted from the emergency department had not been screened within 4 hours of admission. In the future, the standardized dysphagia screening protocol and checklist can be applied in the emergency department to improve the holistic compliance rate of dysphagia screening in stroke patients at the hospital.
CONCLUSIONThis project demonstrated clinically important changes in nursing practice related to dysphagia screening. The project was successful not only in increasing the knowledge and changing the attitudes of nurses but also in implementing a standardized process for dysphagia screening. These findings reinforce the importance of a standardized protocol using valid dysphagia screening tools. Furthermore, strategies such as regular training, supervision, and audits of dysphagia screening should be implemented to monitor the process and evaluate the outcomes. In the future, the subsequent management of dysphagia patients, such as comprehensive swallowing function assessment and dietary guidance, should be standardized and integrated into clinical practice.
ACKNOWLEDGMENTSWe acknowledge the nursing staff in the neurology ward for their support and participation in this study. Thanks are also extended to the Adelaide team at JBI, particularly Lucylynn Lizarondo, for providing valuable time, guidance, and wisdom.
AVAILABILITY OF DATA AND MATERIALSThe data supporting the findings of this study and the materials used for strategies (PowerPoint slides and checklist for dysphagia screening) are available in Chinese from the corresponding author upon request.
AUTHOR CONTRIBUTIONSStudy conception: GS, YW, JW. Study design: GS, JW. Acquisition of data: QX, XZ, PX. Analysis and interpretation of data: GS. Manuscript drafting and revision: GS, JW. Final approval: all authors.
FUNDINGThis project was supported by the Zhongshan Hospital Fudan University “JBI Fellowship Best Evidence Implementation Program in 2022.” The funder had no role in the design of the study, the collection or analysis of data, or the decision to publish.
CONFLICTS OF INTERESTThe authors have no conflicts of interest to declare.
REFERENCES 1. Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480687 adults. Circulation 2017; 135 (8):759–771. 2. Wu S, Wu B, Liu M, Chen Z, Wang W, Anderson CS, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol 2019; 18 (4):394–405. 3. GBD 2016 causes of death collaborators. global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390 (10100):1151–1210. 4. Banda KJ, Chu H, Kang XL, Liu D, Pien LC, Jen HJ, et al. Prevalence of dysphagia and risk of pneumonia and mortality in acute stroke patients: a meta-analysis. BMC Geriatr 2022; 22 (1):420. 5. Boaden E, Burnell J, Hives L, Dey P, Clegg A, Lyons MW, et al. Screening for aspiration risk associated with dysphagia in acute stroke. Cochrane Database Syst Rev 2021; 10 (10):D12679. 6. Bath PM, Lee HS, Everton LF. Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst Rev 2018; 10 (10):D323. 7. Teh WH, Smith CJ, Barlas RS, Wood AD, Bettencourt-Silva JH, Clark AB, et al. Impact of stroke-associated pneumonia on mortality, length of hospitalization, and functional outcome. Acta Neurol Scand 2018; 138 (4):293–300. 8. Feng MC, Lin YC, Chang YH, Chen CH, Chiang HC, Huang LC, et al. The mortality and the risk of aspiration pneumonia related with dysphagia in stroke patients. J Stroke Cerebrovasc Dis 2019; 28 (5):1381–1387. 9. Eltringham SA, Kilner K, Gee M, Sage K, Bray BD, Pownall S, et al. Impact of dysphagia assessment and management on risk of stroke-associated pneumonia: a systematic review. Cerebrovasc Dis 2018; 46 (3–4):99–107. 10. Sherman V, Greco E, Martino R. The benefit of dysphagia screening in adult patients with stroke: a meta-analysis. J Am Heart Assoc 2021; 10 (12):e18753. 11. Teasell R, Salbach NM, Foley N, Mountain A, Cameron JI, Jong A, et al. Canadian stroke best practice recommendations: rehabilitation, recovery, and community participation following stroke. Part one: rehabilitation and recovery following stroke. 6th edition update; 2019. Int J Stroke 2020; 15 (7):763–788. 12. Dziewas R, Michou E, Trapl-Grundschober M, Lal A, Arsava EM, Bath PM, et al. European Stroke Organisation and European Society for Swallowing Disorders guideline for the diagnosis and treatment of post-stroke dysphagia. Eur Stroke J 2021; 6 (3):LXXXIX-CXV. 13. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019; 50 (12):e344–e418. 14. Ma K, Guo Y, Dong X, Yang C, Zhang P, Wang M, et al. The status of screening and evaluation of dysphagia in stroke patients by nurses in Henan province. Chinese J Nursing 2020; 55 (8):1196–1200. 15. Hines S, Kynoch K, Munday J. Nursing interventions for identifying and managing acute dysphagia are effective for improving patient outcomes: a systematic review update. J Neurosci Nurs 2016; 48 (4):215–223. 16. Porritt K, McArthur A, Lockwood C, Munn Z, editors. JBI Manual for Evidence Implementation [internet]. JBI; 2020 [cited 2023 Mar 10]. Available from: https://implementationmanual.jbi.global/. 17. Stroke Foundation. Clinical guidelines for stroke management [internet]. Stroke Foundation [cited 2023 Mar 10]. Available from: https://informme.org.au/guidelines/clinical-guidelines-for-stroke-management. 18. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016; 47 (6):e98–e169. 19. Mao X, Wang G, Chen R, Meng X, Yu L. Construction and reliability and validity test of the knowledge, attitude and practice scale for dysphagia after stroke in nurses. Chinese J Nursing 2021; 37 (15):1140–1145. 20. Rofes L, Arreola V, Clavé P. The volume-viscosity swallow test for clinical screening of dysphagia and aspiration. Nestle Nutr Inst Workshop Ser 2012; 72:33–42. 21. Sivertsen J, Graverholt B, Espehaug B. Dysphagia screening after acute stroke: a quality improvement project using criteria-based clinical audit. BMC Nursing 2017; 16:1–8. 22. Liu H, Shi Y, Shi Y, Hu R, Jiang H. Nursing management of post-stroke dysphagia in a tertiary hospital: a best practice implementation project. JBI Database Syst Rev Implement Rep 2016; 14 (7):266–274. 23. Chen PC, Chuang CH, Leong CP, Guo SE, Hsin YJ. Systematic review and meta-analysis of the diagnostic accuracy of the water swallow test for screening aspiration in stroke patients. J Adv Nurs 2016; 72 (11):2575–2586. 24. Smith HA, Lee SH, O’Neill PA, Connolly MJ. The combination of bedside swallowing assessment and oxygen saturation monitoring of swallowing in acute stroke: a safe and humane screening tool. Age Ageing 2000; 29 (6):495–499. 25. Lim SH, Lieu PK, Phua SY, Seshadri R, Venketasubramanian N, Lee SH, et al. Accuracy of bedside clinical methods compared with fiberoptic endoscopic examination of swallowing (fees) in determining the risk of aspiration in acute stroke patients. Dysphagia 2001; 16 (1):1–6.
留言 (0)