
記住我

Central line-associated bloodstream infections (CLABSIs) and catheter-associated thrombosis (CAT) are common complications caused by inappropriate central venous catheter (CVC) maintenance.1 Furthermore, incorrect removal of CVCs can lead to adverse outcomes, catheter breakage, or air embolism.2 The implementation of evidence-based practice has been widely acknowledged as an effective approach to improve the health care outcomes of patients; however, there are still reports of poor compliance with evidence-based practice. Initiating high-quality implementation research could facilitate evidence dissemination, and consequently, improve CVC-related outcomes, reducing potential complications.3 A systematic review indicates that implementation studies in the field of nursing science are more likely to select methods such as conventional education lectures, audits, and feedback; only a few of have been conducted using targeted and comprehensive strategies.4
Selecting a well-established theoretical framework can guide the implementation of new clinical evidence more efficiently. We carefully considered ten recommendations from methodological experts on the use of theoretical frameworks in implementation research5 and selected the Integrated Promoting Action on Research Implementation in Health Services (i-PARIHS). Originally known as PARIHS, the framework was first developed by Kitson et al. (1998) and included three core elements: (1) evidence, (2) organizational context, and (3) facilitation. The PARIHS was updated in 2016 to i-PARIHS,6 with the addition of a fourth element and a revision of the terminology, as follows: (1) proposed innovation, (2) recipients of the innovation, (3) organizational context inside and outside the implementation site, and (4) facilitation.7 Facilitation is the “active ingredient” of the i-PARIHS framework and is considered key to the successful implementation of innovation.
We used the i-PARIHS framework to guide all phases of the project, from facilitation planning, obtaining baseline data, identifying change facilitators and barriers, formulating the evidence implementation strategy at the micro level, and evaluating the implementation outcomes.8-9
This project was conducted across several sites, namely, six tertiary children's hospitals in China. The project focused on the clinical application of evidence bundles for CVC maintenance. Evidence bundles were derived from reliable scientific sources that were adaptable to the project sites. Three processes were followed: (1) baseline audit, (2) identification of facilitators and barriers, and (3) implementation of strategies. The main outcome measure was nurses’ compliance with evidence-based practice for CVC maintenance.
This project contributes to the literature by providing a research paradigm based on a theoretical model for the entire implementation stage. It also demonstrates the implementation of complex interventions, applied across multiple sites with different organizational cultures.
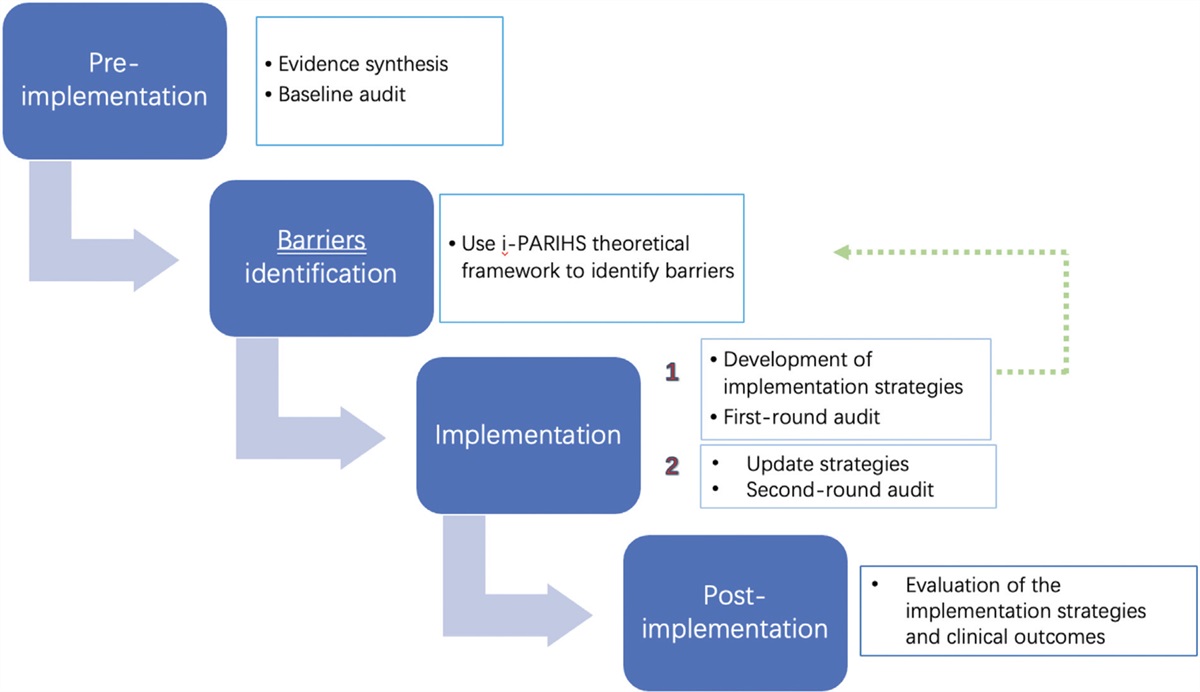
METHODS DesignWe conducted a pre-post control study, with a baseline audit performed from November 4 to 24, 2019. The criteria for the baseline audit were derived from an evidence bundle that we created in a previous project to review the current level of CVC maintenance. Based on the audit results, we identified barriers and facilitators of implementation using three areas of the i-PARIHS framework: innovation, recipients, and organizational context. Implementation strategies were then formulated for each site (see Figure 1). The i-PARIHS framework allowed us to clearly outline the four stages of innovation implementation, as shown in Figure 2.
 Figure 1:
Figure 1: Implementation stages.
 Figure 2:
Figure 2: Facilitator's toolkit.
SettingThis multi-site study was carried out in the pediatric intensive care units (PICUs) of six tertiary children's hospitals (S1–S6) in Shanghai, Zhejiang, Anhui, Guangzhou, Shenzhen, and Xiamen, China. The total number of beds in S1–S6 ranged from 20 to 35, and the number of nurses ranged from 19 to 90. The average number of working years of the nurses was 5 (01 ± 4.39). All the implementation sites had experience of introducing changes, which indicated that employees would be willing to accept innovations.
PRE-IMPLEMENTATION Intervention / evidence bundle preparationThe changes to be implemented were derived from health care bundles developed through rigorous literature searches and quality appraisal. Thus, following a comprehensive search of five scientific databases, evidence summaries were obtained.10-13 We extracted 44 recommended pieces of evidence from these summaries, and 17 pieces of evidence were finally accepted after checking for duplicates. A stakeholder group at each implementation site convened to discuss and revise each intervention using the FAME framework (Feasibility, Appropriateness, Meaningfulness, and Effectiveness).14 The retained evidence was converted into 22 clinical audit criteria, as presented in Table 1.
Table 1 - Sources, evidence bundles, and audit criteria Source Evidence bundle Audit criteria Central venous catheter (CVC): Dressing and flushing 1. Dressing should be assessed daily. (Level 5, Grade B) 1. Dressing should be assessed daily. 2. Either gauze and tape or transparent polyurethane dressings are acceptable types of dressings. Preferably, a sterile, transparent, semi-permeable polyurethane dressing should be used to cover the catheter site. (Level 5, Grade A) 2. Either gauze and tape or transparent polyurethane dressings are acceptable types of dressings. Preferably, a sterile, transparent, semi-permeable polyurethane dressing should be used to cover the catheter site. CVC (primary and community care): Infection control 3. If a patient has profuse perspiration or if the insertion site is bleeding or oozing, a sterile gauze dressing is preferable to a transparent, semi-permeable dressing. A gauze dressing should be replaced by a transparent dressing as soon as possible. (Level 5) (Grade B) 3. If a patient has profuse perspiration or if the insertion site is bleeding or oozing, a sterile gauze dressing is needed. A gauze dressing should be replaced by a transparent dressing as soon as possible. 4. CVC dressings should be changed 24 hours after insertion, and then weekly thereafter unless there is a specific indication to change it (such as leaking site). (Level 5, Grade B) 12. CVC dressings should be changed 24 hours after insertion. 13. CVC dressings should be changed weekly unless there is a specific indication to change it (such as leaking site). 5. Preferably, sterile 0.9% sodium chloride injections should be used to flush and lock catheter lumens. (Grade B) 4. Sterile 0.9% sodium chloride injections should be used to flush catheter lumens. 5. Sterile 0.9% sodium chloride injections should be used to lock catheter lumens. Evidence summary. Intravascular therapy: Maintaining catheter lumen patency 6. A pulsated flushing technique (1 ml at a time) by maintaining positive pressure is recommended to create turbulence within the catheter lumen, removing debris from the catheter wall. (Grade B) 6. A pulsated flushing technique (1 ml at a time) by maintaining positive pressure has been used to flush the catheter lumens. 7. A pulsated flushing technique (1 ml at a time) by maintaining positive pressure has been used to lock catheter lumens. CVC: Skin antisepsis 7. More than 0.5% chlorhexidine preparation before insertion and during dressing changes is recommended. If there is a contraindication to chlorhexidine, tincture of iodine, an iodophor, or 70% alcohol can be used as alternatives. (Grade A) 8. More than 0.5% chlorhexidine preparation before insertion has been used. (If there is a contraindication to chlorhexidine, tincture of iodine, an iodophor, or 70% alcohol can be used as alternatives). 9. More than 0.5% chlorhexidine during dressing changes has been used. (If there is a contraindication to chlorhexidine, tincture of iodine, an iodophor, or 70% alcohol can be used as alternatives). CVC (primary and community care): Infection control 8. Before accessing or dressing central vascular catheters, hands must be decontaminated either by washing with an antimicrobial liquid soap and water or by using an alcohol hand rub. (Grade A) 10. Before accessing central vascular catheters, hands must be decontaminated either by washing with an antimicrobial liquid soap and water or by using an alcohol hand rub. 11. Before dressing central vascular catheters, hands must be decontaminated either by washing with an antimicrobial liquid soap and water or by using an alcohol hand rub. 9. Hands that are visibly soiled or contaminated with dirt or organic material must be washed with soap and water before using an alcohol hand rub. (Grade A) 16. Hands that are visibly soiled or contaminated with dirt or organic material must be washed with soap and water before using an alcohol hand rub. 10. In general, administration sets in continuous use do not need to be replaced more frequently than at 72-hour intervals unless they become disconnected or if a catheter-related infection is suspected or documented. (Grade A) 14. Administration units in continuous use do not need to be replaced more frequently than at 72-hour intervals unless they become disconnected or if a catheter-related infection is suspected or documented. 11. Administration sets used for total parenteral nutrition (TPN) infusions should generally be changed every 24 hours. If the solution contains only glucose and amino acids, administration sets in continuous use do not need to be replaced more frequently than every 72 hours. (Grade B) 15. Administration sets used for total parenteral nutrition (TPN) infusions should generally be changed every 24 hours. If the solution contains only glucose and amino acids, administration sets in continuous use do not need to be replaced more frequently than every 72 hours. Central venous access device (CVAD): Removal 12. The patient should lay flat during CVC removal to avoid an air embolus. (Grade B) 17. The patient should lay flat during CVC removal. 13. The platelet count should be more than 50 × 109 per liter and the INR less than 1.5 before catheter removal. (Grade B) 18. The platelet count should be more than 50 × 109 per liter and the INR less than 1.5 before catheter removal. 14. The catheter should be inspected carefully after removal to ensure it is intact. (Grade B) 19. The catheter should be inspected carefully after removal to ensure it is intact. 15. After removal, pressure should be applied to the site for a minimum of 5 minutes and an occlusive dressing placed over the exit site to avoid air embolism. (Grade B) 20. After removal, pressure should be applied to the site for a minimum of 5 minutes and an occlusive dressing placed over the exit site to avoid air embolism. 16. If removed because of suspected infection, the catheter tip should be sent to the lab for culture. (Grade B) 21. If removed because of suspected infection, the catheter tip should be sent to the lab for culture. 17. The patient should perform the Valsalva maneuver during removal (or hold their breath if unable to perform the Valsalva maneuver) to prevent air embolism. (Grade B) 22. The patient should perform the Valsalva maneuver during removal (or hold their breath if unable to perform the Valsalva maneuver) to prevent air embolism.All six implementation sites reported unsatisfactory evidence-based practices related to CVC maintenance; however, there were notable differences in terms of policies, regulations, and internal context across the six institutions. In addition, the innovations that we were planning to implement were relatively complex, and involved many participants and stakeholders. Because of this complexity,15 it was agreed that a baseline audit was necessary. Baseline audits make it easier to identify barriers and facilitators and map these to a theoretical model. This also means that implementation outcomes can be compared and evaluated. The audit was conducted when catheters were being inserted or removed, or when dressings were changed during each day shift. Specialist nurses in each setting took responsibility for the audit, and the results were summarized daily. Compliance for each audit criterion was calculated as "the number of cases that completed or reached the criteria requirements/the total number of cases audited for this criteria∗100%.”
IMPLEMENTATION Identification of barriersThe findings of the baseline and first-round audits were discussed by the stakeholders from the six sites and mapped to the i-PARIHS framework.16 Specifically, the barriers identified through stakeholder group discussions and interviews with nurses were categorized as follows:
Innovation barriers: Evidence related to CVC removal was not part of regular nursing practice at all the project sites and a daily evaluation checklist and process for CVC insertion/removal and dressing were not available. The PICU nurses failed to understand practical recommendations during CVC maintenance and removal and some elements of the new evidence-based bundle created additional workflows for the nurses, which was contrary to what the nurses had originally understood about the intervention.
Recipient barriers: Some nurses did not consider the use of evidence to be valuable because no serious adverse events had occurred in the past. Some nurses were also concerned about the risk of adverse events in some of the evidence, such as dressing change 24 hours after insertion may increase the incidence of skin injury due to dressing removal. Insufficient knowledge about the mechanism of CLABSI (central line-associated bloodstream infection), skills in the Valsalva maneuver during CVC removal, and inter-departmental communication and negotiation between the different implementation sites still needed to be refined.
Context barriers: There was no management system or implementation plan to specifically drive reform and innovation. In the process of authorizing management, the rights and responsibilities of each level of management were not sufficiently clear. The lack of concrete measures to strengthen change was evident at all project sites.
Development of implementation strategiesWe requested facilitators from the six sites to conduct multiple rounds of discussion to develop the implementation strategies. These strategies were as follows:
Revise the existing CVC maintenance process, develop a standardized process for CVC removal, and clearly indicate the level of evidence and recommendations for each nursing practice. Develop a daily assessment checklist for the CVC insertion site and dressing and integrate this into the hospital information system. Include key members of the PICU nursing team in the regular meetings at each site and provide feedback on project progress to key staff. Listen to the feedback from nursing staff through formal and informal consultation, understand the current status of work following the implementation, and modify and improve implementation strategies over time. Enhance PICU nurses’ ability to implement the strategies. Adopt a variety of training methods (eg, theoretical training combined with skills training). Use the training method of in situ scenario simulation to reduce the concerns of nurses and share training materials between the six sites, such as videos demonstrating CVC maintenance and removal or videos demonstrating key points (ie, pulsed tube flushing, Valsalva maneuver for CVC removal). Enhance PICU nurses’ willingness to implement innovations. Improving nurses’ knowledge and willingness to implement the strategies through a literature review of case reports, (eg, air embolism after CVC removal without the Valsalva maneuver) or by referring back to the original research of the evidence, and interpreting the research findings. Establish a system of regular multi-center meetings to openly discuss issues and project progress in greater depth. Develop strategies to support the changes and summarize the clinical benefits, patient experience, and academic achievements brought about by the changes in a timely manner. Set up a regular reporting system to obtain more support and resources and create a culture that promotes innovation and change. Conducting the implementationSix sites implemented the strategies from March to April 2020. The first-round audit was conducted in September 2020 and lasted 2 to 4 weeks. Based on the results of this audit, we identified barriers and implemented strategies to address these barriers.
POST-IMPLEMENTATION Evaluation of the implementationWe conducted a second-round audit in December 2020, which lasted 2 to 4 weeks. The same criteria were used as for the baseline audit. We compared the results of this audit with the baseline and first-round audits to evaluate the implementation outcomes.
RESULTS Baseline auditData collection for the baseline audit was performed at 8 AM each morning shift, during treatment hours (10–11 am, 3–5 pm, 9–11 pm), when CVC insertion, removal, or dressing changes usually occurred. In total, 661 episodes of nurses’ CVC maintenance were reviewed in 293 patients. The percentages for the catheter insertion sites were as follows: femoral vein (64.16%), internal jugular vein (33.79%), and subclavian vein (2.04%). The top three diseases were intracranial space-occupying lesions (14.33%), severe pneumonia (9.22%), and tumors (8.19%).
Nurses showed a high level of practice (compliance rate > 80%) for only six audit criteria (2, 4, 8, 9, 10, and 13), while seven criteria (3, 5, 14, 15, 17, 18, and 22) had room for improvement (compliance rate < 60%). The compliance for three criteria (criterion 15 – 24.37%, criterion 18 – 4.55%, and criterion 22 – 2.38%) was poor in all six hospitals; only two criteria (2, 10) had a compliance rate of more than 75%. Figure 3 presents the evaluation results, while Table 2 presents details of the percentages. Data on CLABSI incidence in each setting were collected separately at the end of each research phase and statistically compared to illustrate the clinical effectiveness of the project.
 Figure 3:
Figure 3: Compliance with evidence-based practice in the baseline, round 1, and round 2 audits.
Table 2 - Compliance (%) with evidence-based practice in the baseline, round 1, and round 2 audits Audit criterion Baseline audit (%) Round 1 audit (%) Round 2 audit (%) 1 74.25 96.77 94.84 2 98.88 99.64 96.33 3 43.21 84.73 89.08 4 86.35 100.00 95.97 5 51.91 96.11 96.62 6 74.92 91.29 92.45 7 69.71 92.12 88.68 8 83.75 92.13 84.06 9 80.50 94.63 87.63 10 86.80 92.68 85.52 11 74.75 95.02 94.83 12 71.63 89.42 92.31 13 91.44 99.05 96.68 14 42.00 83.63 75.75 15 24.37 83.05 85.58 16 79.02 77.02 100.00 17 53.33 93.10 89.29 18 4.55 54.84 68.33 19 75.56 83.33 95.00 20 64.44 100.00 96.55 21 76.92 94.74 88.89 22 2.38 71.43 71.92We convened facilitators and stakeholder representatives from the six sites to discuss the baseline audit results. The three core elements of the theoretical model—innovation, recipients, and organizational context—fully covered the identification of barriers and facilitators. To minimize barriers and enable facilitators, we developed micro-level implementation strategies to better support the implementation strategies. These included reminders, management supervision, clinical innovation leaders, interdisciplinary education, educational outreach, educational meetings, educational materials, monitoring, clinical incident reporting, audit and feedback, and organizational level innovation.
Evaluation of the implementationThe implementation strategies were formally applied from May to August 2020. The first-round audit was conducted from September to October 2020 to evaluate these strategies and the clinical outcomes. Nurses’ compliance with evidence-based practice in the second-round audit was still below 80% for three audit criteria (14, 18, and 22). However, 17 audit criteria (1–8, 11–12, 14–20, and 22) showed a significant improvement in the second-round audit, which was statistically significant (p < 0. 05).
For 12 audit criteria (1–7, 9–11, and 19–20), compliance with intervention guidelines reached more than 80% at the six sites; however, compliance for four audit criteria (14, 15, 18, and 22) showed significant variations between each site. Compared with the baseline, the results of the second-round audit showed that compliance with more than ten audit criteria had significantly improved in all sites except S3, and the difference was statistically significant (p < 0.05) (see Figure 3).
DISCUSSIONCompliance with the daily assessment of CVCs (ie, dressings and insertion site), use of normal saline for flushing and locking, frequency of administration set replacement, and CVC removal was relatively low. Notably, these were all critical steps in CVC maintenance. Based on the identified barriers, conclusions could be drawn at the recipient and organizational levels: each hospital did not have the latest evidence-based guidelines to update its systems and processes, leading to a gap between clinical practice and evidence-based guidelines. Therefore, when evidence was first introduced into the clinic, interpersonal relationships and major process changes were the biggest obstacles encountered at the beginning of the project. Particularly, low willingness to accept the innovation by “local opinion leaders” at some of the implementation sites represented one of the major obstacles. Local opinion leaders were usually the heads of a nursing shift team or senior nurses in the ward. In the second round of innovation, through communication and listening to their suggestions, the local opinion leaders’ negative attitude toward change was turned into a positive attitude, thereby becoming a facilitator of change. This problem has not been addressed in previous evidence implementation projects. We also found that barrier identification in the organizational context dimension of i-PARIHS was easily ignored. Due to the various understandings at each site and the different medical environments in the different provinces, the specific barriers in the organizational context dimension were also different.
In addition, we found that whether organizations have a culture that is open to innovation is highly correlated with the speed at which they remove barriers. A positive culture can promote the application of innovation, thereby facilitating change. One barrier in S2 was the lack of CVC maintenance kits. Through negotiation between the nursing department and the materials supply department, CVC maintenance kits were introduced to that hospital to increase compliance with evidence-based practice. S5 introduced a glucose alcohol chlorhexidine solution in the same way. In addition, both S1 and S5 received patients from the operating room. The facilitator from the nursing department ensured that the strategy was correctly implemented in the operating room by communicating with the anesthesiology department (eg, selection of skin antiseptic solution and application of the dressing). We also found that the organizational context dimension usually acted as a facilitating force in our project, which is due to the stable health care system and the consistency in strategic priorities of the wider health system.
After the implementation of the project, although 81.8% of the clinical audit criteria had significantly improved, some items did not reach the expected targets. For example, “no more frequently than at 72-hour intervals” was not clearly specified (audit criterion 14: Administration units in continuous use do not need to be replaced more frequently than at 72-hour intervals unless they become disconnected or if a catheter-related infection is suspected or documented). Therefore, the clinical nurses were not given precise information on replacement frequency. Similarly, audit criterion 18 (The platelet count should be more than 50 × 109 per liter and the INR less than 1.5 before catheter removal) was not easy to comply with because some hospitals could not easily obtain the patient's platelet or INR laboratory test report (no PDA or bedside computer, or the patient did not have that particular blood test). Moreover, the source of the evidence was obtained from the patient results in the hematology department and S6 queried whether audit criterion 18 was also applicable to the patients in the non-hematology department. For audit criterion 22 (The patient should perform the Valsalva maneuver during removal, or hold their breath if unable to perform the Valsalva maneuver), infants are unable to perform this maneuver independently; therefore, the nurse had to observe the infant's abdominal breathing rhythm when the CVC was removed. For non-mechanically ventilated children who are able to communicate, the nurse had to teach them the Valsalva maneuver. In cases of mechanical ventilation, nurses needed to observe the expiratory phase of the ventilator to determine the best time to remove the CVC. Therefore, the Valsalva maneuver had relatively high requirements for nurses’ clinical practice. For audit criterion 12 (Dressings for CVCs should be changed 24 hours after insertion), S2 and S6 proposed that it would increase the incidence of skin injury related to dressing adhesion and that nurses may hesitate to comply with this criterion. More concrete and innovative measures should be developed in our future research.
StrengthsAlthough most implementation studies report on compliance with the implemented changes, they do not necessarily indicate that the implementation strategy was applied effectively. For this reason, our study directly audited the behavioral compliance of the recipients (ie, the nurses) regarding the quality of the implementation strategies.17 Another strength of our study was the diversity of the implementation strategies. According to a systematic review, most implementation studies use education and training as the main strategies18 and select only two to four types of strategies. As our study involved multiple sites, the regional and institutional cultures were relatively complex. To cater for this complexity, 11 intervention strategies were selected, which diversified and enriched the intervention.
LimitationsWe intended to use the i-PARIHS framework for the entire implementation project. However, we were unable to ensure that the barriers were identified clearly at each site and that the strategies were implemented equally at all sites. The was because of the complexity in identifying stakeholders and the large number of participating sites. Further research would be required to consider the safety culture of each organization as well as local policies when developing the implementation strategies.
CONCLUSIONSThe i-PARIHS framework is an effective tool for developing targeted, evidence-based implementation strategies. Evidence was applied to clinical practice through a carefully thought out implementation strategy. The quality of the nurses’ clinical practice improved during CVC maintenance as a result of the project. However, there is no certainty that these positive results can be maintained, and long-term data are needed to verify this.
ACKNOWLEDGMENTSThis study was conducted with the support of all the nurses in six tertiary children's hospitals in Shanghai, Shenzhen, Guangzhou, Zhejiang, Anhui, and Xiamen, China. WCW (project coordinator) from Shanghai, XC, YYS, YXZ, and JPL were the coordinators of the implementation sites.
AVAILABILITY OF DATA AND MATERIALSThe datasets used in this study are available from the corresponding author upon reasonable request.
FUNDINGThis study was funded by the Scientific Research Foundation of Shanghai Local High-Level University Construction Project – Evidence-based Nursing Innovation Research Institute: Multi-Center Evidence-Based Innovation Practice Project (Grant number: FNDGJ201904).
AUTHOR CONTRIBUTIONSYG was responsible for the design, training of the nurses, and securing funding the project. WJS YLX, LJW, XC, YYS, JPL, and YXZ were responsible for data collection, barrier identification, and guideline implementation. WCW and QF were responsible for data analysis, and WCW was responsible for the first draft of the manuscript. All the authors have read and approved the final manuscript.
ETHICSThis study was approved by the Pediatric Research Ethics Board of the Children's Hospital of Fudan University (approval number: IRB2020427).
REFERENCES 1. Aminzadeh Z, Simpson P, Athan E. Central venous catheter associated blood stream infections (CVC-BSIs) in the non-intensive care settings: epidemiology, microbiology and outcomes. Infect Dis Health 2019; 24 (4):222–228. 2. Bernard LA, Katzman A, Mathew DK, Oller KL. Prevention of central venous catheter removal-associated air embolization. Am J Med 2018; 131 (3):e12. 3. Ray-Barruel G, Xu H, Marsh N, Cooke M, Rickard CM. Effectiveness of insertion and maintenance bundles in preventing peripheral intravenous catheter-related complications and bloodstream infection in hospital patients: a systematic review. Infect Dis Health 2019; 24 (3):152–168. 4. Spoon D, Rietbergen T, Huis A, Heinen M, van Dijk M, van Bodegom-Vos L, et al. Implementation strategies used to implement nursing guidelines in daily practice: a systematic review. Int J Nurs Stud 2020; 111:103748. 5. Moullin JC, Dickson KS, Stadnick NA, Albers A. Ten recommendations for using implementation frameworks in research and practice. Implement Sci Commun 2020; 1:42. 6. Kitson AL, Harvey G. Methods to succeed in effective knowledge translation in clinical practice. J Nurs Scholarsh 2016; 48 (3):294–302. 7. Harvey G, Kitson A. PARIHS revisited: from heuristic to integrated framework for the successful implementation of knowledge into practice. Implement Sci 2016; 11:33. 8. Hunter SC, Kim B, Mudge A, Hall L, Young A, McRae P, et al. Experiences of using the i-PARIHS framework: a co-designed case study of four multi-site implementation projects. BMC Health Serv Res 2020; 20 (1):573. 9. Huang M, Gu Y, Zhang YX, Hu Y, Zhou Y. Development and evaluation of reliability and validity of Clinic Readiness to Evidence-based Nursing Assessment scale. Chin J Evid Based Pediatr 2017; 12 (2):121–125. 10. JBI recommended practice. Central venous access device: accessing and line patency. The JBI EBP Database 2016; JBI-RP-4157-4. 11. JBI recommended practice. Central venous access device: dressing change. The JBI EBP Database 2019; JBI14276. 12. Porritt K. Evidence summary. Central venous access device: removal. The JBI EBP Database 2019; JBI14273. 13. Obeid S. Evidence summary. Central venous catheterization (primary and community care): infection control. The JBI EBP Database 2017; JBI1543. 14. Pearson A, Wiechula R, Court A, Lockwood C. The JBI model of evidence-based healthcare. Int J Evid Based Healthc 2005; 3:207–215. 15. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ 2021; 374:n2061. 16. MacGregor A, Rutherford A, McCormack B, Hockley J, Ogden M, Soulsby I, et al. Palliative and end-of-life care in care homes: protocol for codesigning and implementing an appropriate scalable model of needs rounds in the UK. BMJ Open 2021; 11 (2):1–9. 17. Slaughter SE, Hill JN, Snelgrove-Clarke E. What is the extent and quality of documentation and reporting of fidelity to implementation strategies: a scoping review. Implement Sci 2015; 10:129. 18. Straus SE, Sales A, Wensing M, Michie S, Kent B, Foy R. Education and training for implementation science: our interest in manuscripts describing education and training materials. Implement Sci 2015; 10:136.
留言 (0)