Quality improvement programs are critical for hospitals to improve the quality of care, resulting in better patient outcomes, reducing health care costs, and improving the efficiency of staff.1 Clinical audit has been advocated as an effective quality improvement approach to identify practice gaps and improve the quality of care.2 In recent years, multi-site audit projects have been increasingly used to translate evidence into practice at scale through collaboration between health care organizations.3 The JBI Model of Evidence-based Healthcare (EBHC) was initially developed in 2005 and updated in 2016, representing a developmental framework for EBHC.4 Within this model, the JBI Evidence Implementation Framework further articulates the steps of EBHC in a pragmatic way. Grounded in the audit, feedback, and re-audit process, the framework provides a structured approach to evidence implementation in health care.4–6 JBI's approach has been widely used in small (single-site) or large (multi-site) audit projects to implement evidence in clinics.3,7 This editorial discusses the role of the JBI implementation approach in guiding the project management of a massive multi-site audit project.
Preparing for a muti-site audit project involves numerous steps, starting with the recruitment of participants, identifying the priority clinical problem, and determining the lead entity. Engaging participating hospitals or health authorities and improving their compliance during the evidence implementation process are essential for the success of a massive multi-site audit project.
Many other factors must be considered in each phase of a muti-site audit project. First, given the diverse needs and the heterogeneity of the contexts at each site, it is important that the subject be of interest; but not only that, it must also address a clinical problem that each participating group can identify with. Different approaches can be used to identify a priority clinical audit problem, such as surveys, interviews, or consensus voting. Once the clinical problem has been determined and the context has been assessed at each site, the focus shifts to what evidence will underpin the project. The development of evidence-based audit criteria is important for systematic evaluation and monitoring. Through partnership with a global evidence organization such as JBI, evidence-based summaries and audit criteria can be accessed through the JBI EBP Database and the JBI PACES software tool.8 To date, numerous multi-site audit projects drawing upon criteria from the JBI EBP Database have had a significant impact on improving patient outcomes and the quality of care.3,8
Second, we need to consider two aspects of leadership in a massive multi-site audit project. The first aspect is the leadership of the lead entity in the project. A trusted, influential, respected, and believable lead entity is essential to engage the participating hospitals or health authorities. The second aspect is the leadership of the leaders at each participating site, which can also influence the success of multi-site projects.9 This is because unlike original studies (such as multi-site randomized controlled trials), the interventions and procedures of the research cannot be standardized across participating centers. Due to the heterogeneity of the contexts, culture, or health care policy in each participating entity of a multi-site audit project, the key barriers identified and the implementation strategies will differ. Given this situation, in addition to the lead entity, each participating site should also have a respected and committed leader who can help to break down barriers and ensure the change is successful. Therefore, it is important to carefully select the key leaders of the participating entities early in the recruitment process.
For a multi-site audit project, it is unlikely that all participating entities will have enough knowledge about clinical audit.2,9 Hence, providing the entities with a very clear and structured project process upfront is crucial. This must be followed by training for each step of the project. Both these steps are key elements in effective project organization.
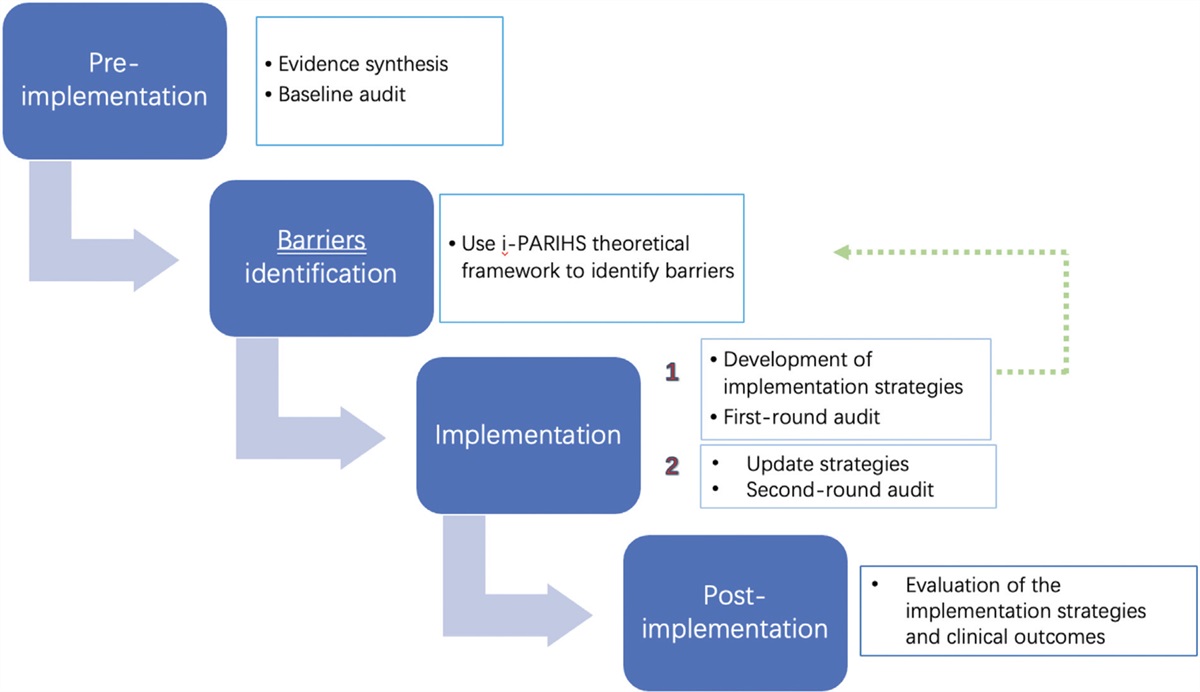
The JBI implementation approach consists of seven steps for audit and feedback, with a structured approach to the identification and management of barriers to compliance with recommended clinical practices.5,6 This approach has been widely used in evidence implementation training programs to guide clinicians step-by-step to implement evidence in health care. For example, in the last 5 years, the Guangdong Nursing Association Evidence-based Nursing Committee in China used the JBI implementation approach to train clinical nurses, where more than 600 nurses from 139 hospitals finished the course and a total of 446 audit projects was conducted.10
It should be noted that although we need to standardize the process of a multi-site audit project to ensure synchronization, we also need to allow each participating site to have its own specific strategies, given the variety of contexts and the complexities of implementation. For example, different participating entities could tailor their implementation strategies to their own context using JBI's Getting Research into Practice (GRiP) tool. Moreover, given the pragmatic nature of the JBI implementation approach,5 users can choose to follow the seven steps alone or consider adding other theories, frameworks, or models.11 For instance, in Step 3 of the JBI approach, users can consider the Consolidated Framework for Implementation Research (CFIR) to provide theory-based constructs for identifying potential barriers and facilitators in an audit project.12
Furthermore, how to maximize the advantages of a massive multi-site audit project should be considered by the project management. In addition to the usual advantages of multi-site projects, such as increasing the credibility and generalizability of the findings,13 several aspects can be considered compared with a single-site audit project.
First, it is essential to set up an online education, presentation, and timely feedback platform, especially for international multi-site organizations. Platforms such as JBI PACES are a useful tool for the lead entity to gather and analyze all the audit data from the participating entities.8 The entities can also report the results of their audit and share their experiences, strategies, or lessons in overcoming barriers. Because this is done through an online platform, it allows other entities to learn from each other. In this way, each participating entity can also exchange its implementation materials, such as videos, training manuals, or patient education pamphlets. This greatly saves on resources while enriching the diversity of implementation strategies in a multi-site audit project.
Second, given the different culture, context, or health policy in each entity in a multi-site audit project, participating in a such a project could improve the understanding of different contexts and cultures and their influence on the translation of evidence. Participating in such a project could also be more motivating (or encouraging) when one site meets challenges, and other sites share their experiences to provide support. Thus, during each presentation, a healthy culture of helping each other will be promoted among the participating entities. Those entities that may be lagging will benefit from higher-performing centers, allowing them to improve standards and make progress.11 This kind of culture is hard to come by in a single-site audit project.
In conclusion, massive multi-site audit projects are advocated to promote and scale up evidence implementation. However, the preparation, organization, and management of a multi-site audit project is much more complex than a single-site project. The JBI implementation approach is an effective model to facilitate this, while the associated PACES software can be used to guide the whole project. Given the complexity of multi-site audit projects and the increasing demand for evidence implementation, we should use this information to iterate the next series of improvements to better carry out such projects in clinics.
1. Weiner BJ, Alexander JA, Shortell SM, Baker LC, Becker M, Geppert JJ. Quality improvement implementation and hospital performance on quality indicators. Health Serv Res 2006; 41 (2):307–334.
2. Hut-Mossel L, Ahaus K, Welker G, Gans R. Understanding how and why audits work in improving the quality of hospital care: a systematic realist review. PLoS One 2021; 16 (3):e0248677.
3. Stephenson M, McArthur A, Giles K, Lockwood C, Aromataris E, Pearson A. Prevention of falls in acute hospital settings: a multi-site audit and best practice implementation project. Int J Qual Health Care 2016; 28 (1):92–98.
4. Jordan Z, Lockwood C, Munn Z, Aromataris E. The updated Joanna Briggs Institute Model of Evidence-Based Healthcare. Int J Evid Based Healthc 2019; 17 (1):58–71.
5. Munn Z, McArthur A, Porritt K, Lizarondo L, Moola S, Lockwood C. Evidence implementation projects using an evidence-based audit and feedback approach: the JBI Implementation Framework. In: Porritt K, McArthur A, Lockwood C, Munn Z, editors. JBI Manual for Evidence Implementation [internet]. JBI; 2020. Available from:
https://implementationmanual.jbi.global.
6. Porritt K, McArthur A, Lockwood C, Munn Z. JBI's approach to evidence implementation: a 7-phase process model to support and guide getting evidence into practice. JBI Evid Implement 2023; 21 (1):3–13.
7. Wu Y, Li W, Stephenson M, Cong W, Zhou C. Pre-treatment assessment for patients with breast cancer undergoing chemotherapy: a best practice implementation project. JBI Evid Synth 2020; 18 (1):212–223.
8. Harvey G, Kitson A, Munn Z. Promoting continence in nursing homes in four European countries: the use of PACES as a mechanism for improving the uptake of evidence-based recommendations. Int J Evid Based Healthc 2012; 10 (4):388–396.
9. Lai J, Brettle A, Zhang Y, Zhou C, Li C, Fu J, et al. Barriers to implementing evidence-based nursing practice from the hospitals’ point of view in China: a regional cross-sectional study. Nurse Educ Today 2022; 116:105436.
10. Zhou C, Wu Y, Zhao H, et al. Strategies to improve evidence-based practice ability of nurses. Chin J Nurs Educ 2021; 18 (10):888–892.
11. Munn Z, McArthur A, Klugar M, Stannard D, Cooper AS, Enuameh Y, et al. Providing a scaffold for considering theoretical frameworks in evidence implementation projects: the JBI approach to evidence implementation. JBI Evid Implement 2023; 21 (4):386–393.
12. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009; 4:50.
13. Basu U. An idea to explore: introduction to research methods. Biochem Mol Biol Educ 2023; 51 (5):566–573.


留言 (0)