
記住我
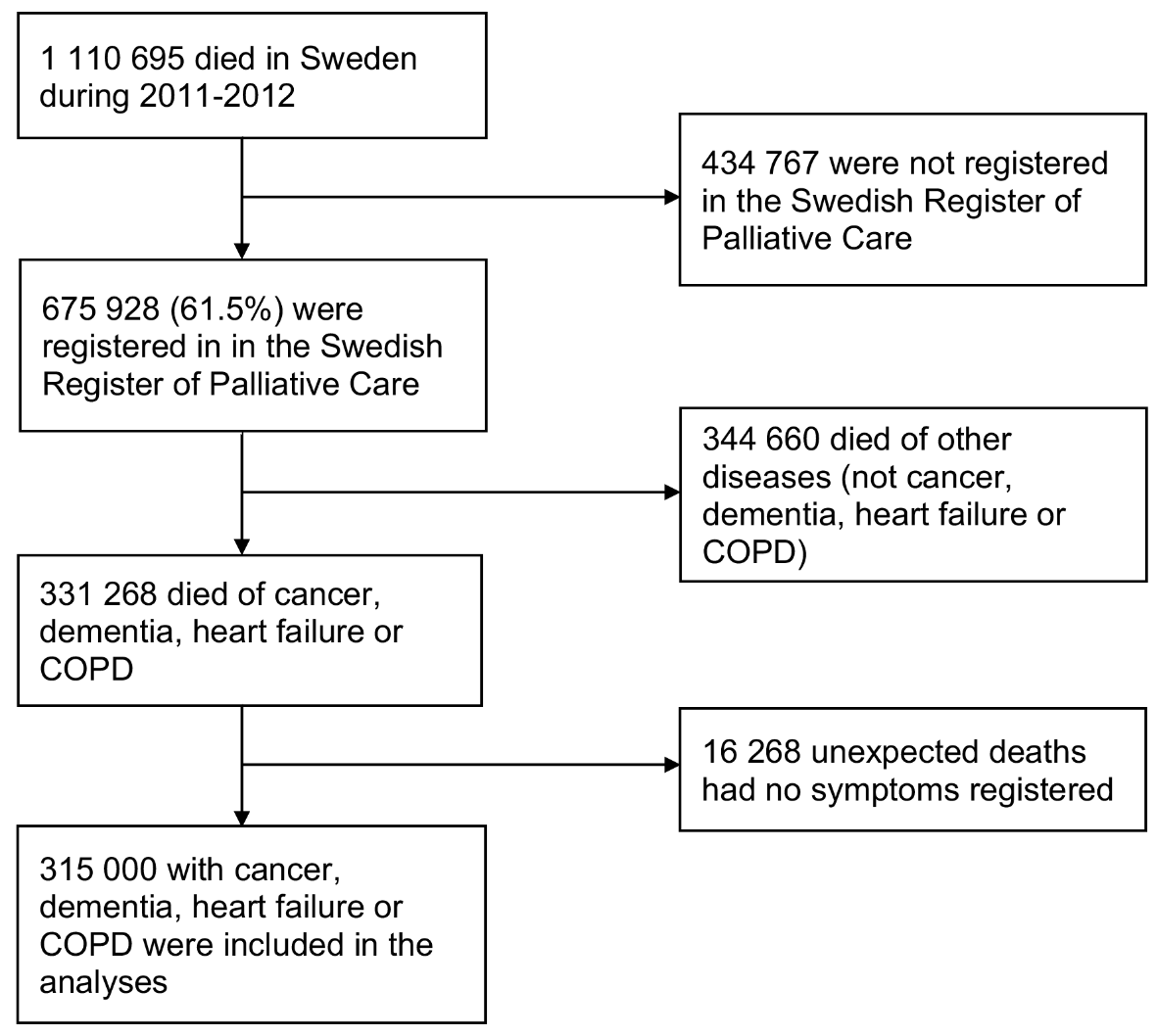
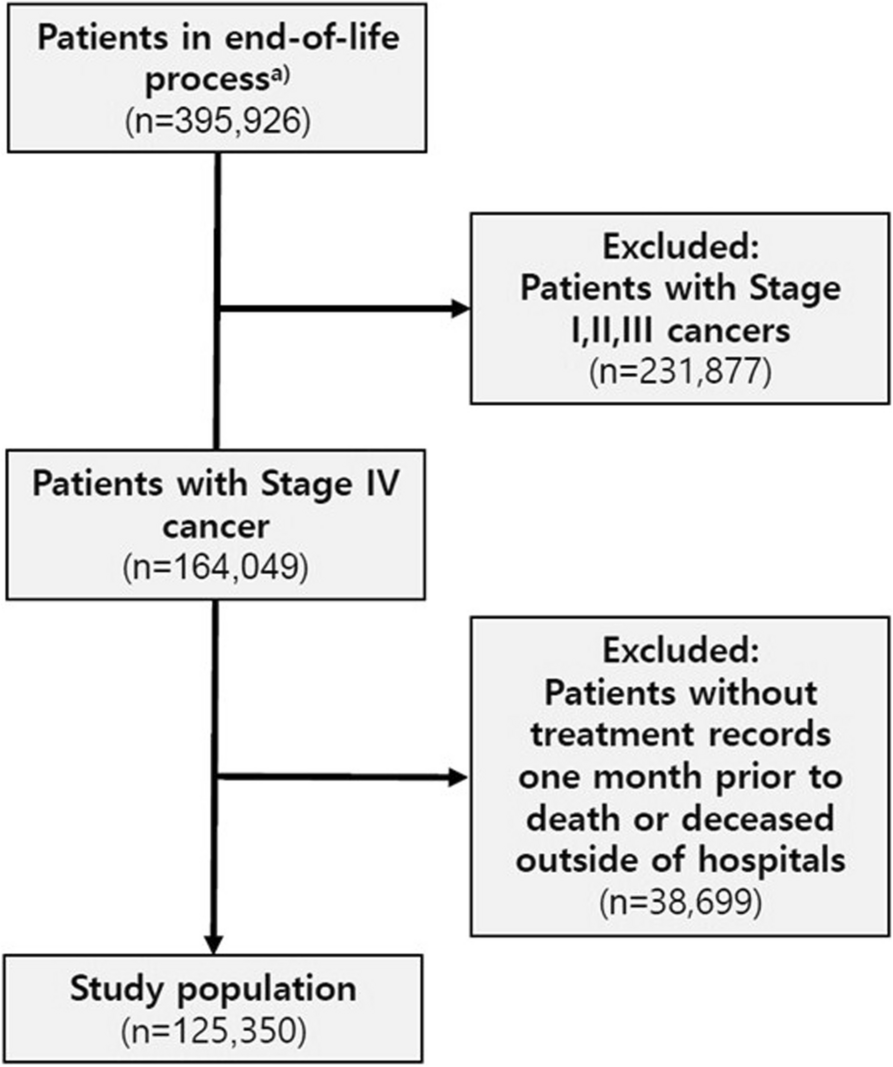
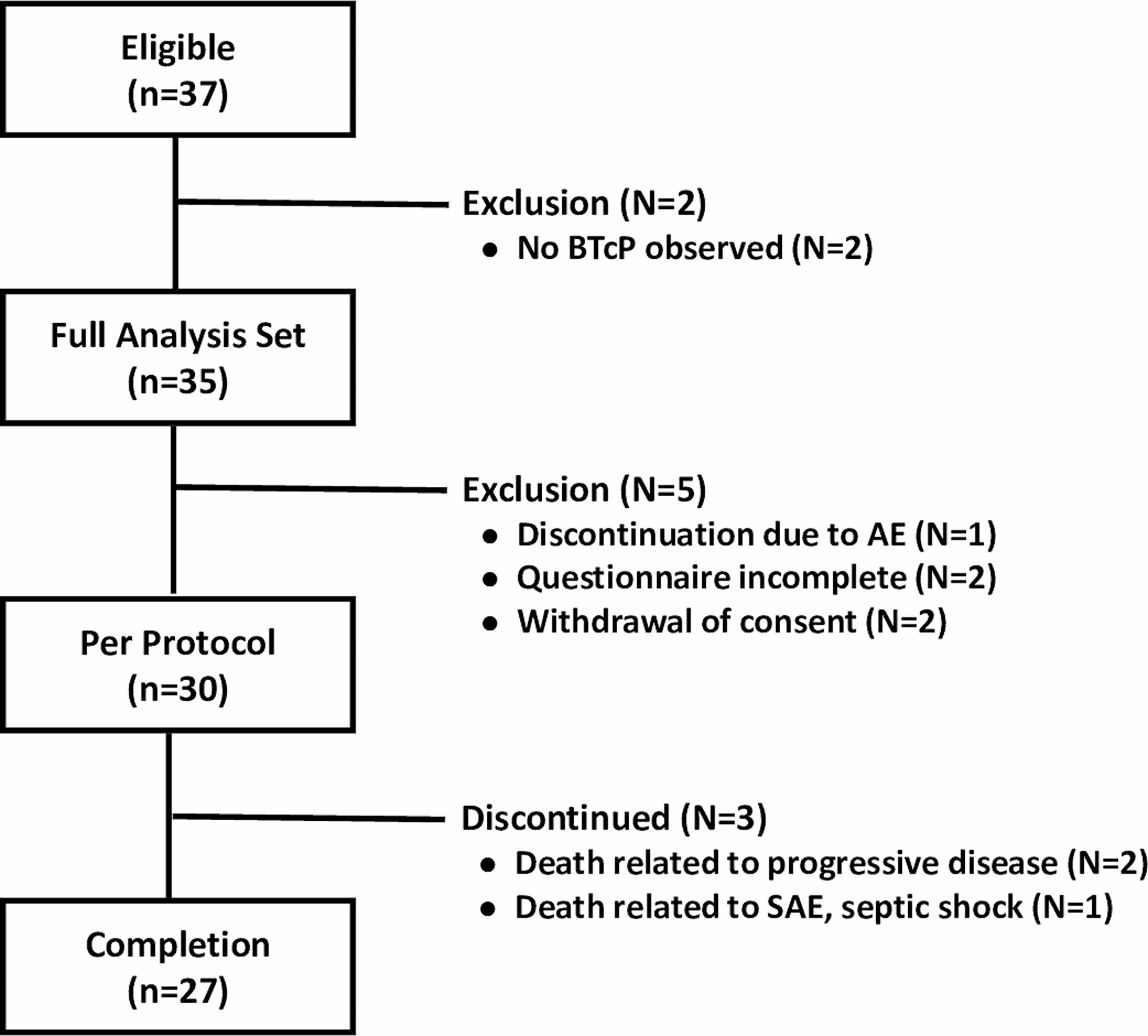
A total of 971 articles were identified by databases searching. A total of 916 were excluded because they were duplicated or were excluded by title and abstract because they were considered not related with barriers and facilitators for public engagement. Fifty-five articles were taken to full-text screening but 6 were excluded because they did not match eligibility criteria and 49 were selected and two main authors reviewed in deep each of the full texts in relation to the inclusion criteria. Reviewers excluded 36 articles in a discussion session because they did not offer relevant information. We obtained 13 articles for the final analysis. Fig. 1 represents the selection process.
Fig. 1
Flow-chart of study retrieval and selection process
The characteristic of the selected articles is summarized in the Table 1. After analysis of the studies, they were broadly categorized into four categories to facilitate the description of the selected studies: 1. Public health and public engagement; 2. Community attitudes towards palliative care, death and preferences at the end of life; 3. Importance of volunteers in public engagement programs; 4. Compassionate communities. Finally, the factors that influenced public engagement in palliative care as barriers and facilitators for this engagement were identified and summarized in Table 2.
Table 1 Summary of the studies selectedTable 2 Barriers and Facilitators for public engagementPublic health and public engagementSallnow et al. [5] published in 2016 a Systematic Review on the impact of a new Public Health approach to end-of-life care. Three main themes emerged: making a difference to practice which describes the impact that public engagement can have on end-of-life experiences; individual learning and growth which describes the personal reflection, development and confidence that those involved embark on; and community capacity building, which refers to the impact of the work beyond the individuals involved, to the wider community where sustainable change can occur. The quantitative results were in line with the meta-ethnography and demonstrated that the involvement of communities can lead to improved outcomes for caregivers, such as decreased fatigue or isolation, increased size of caregiving networks, and that broader social networks can influence factors such as place of death and involvement of palliative care services. They argue that there is evidence of the impact of public engagement in end-of-life care, with important implications for policy makers, practitioners and researchers.
Kumar refers in his study to there being no general consensus on what is meant by community-based approaches to palliative care, yet public engagement is the only realistic model for achieving palliative care coverage for two-thirds of the world's terminally ill, especially as there is too much focus on the medical treatment of these patients [17]. Public engagement is described as a social process in which groups with shared needs living in a "defined geographical area" actively identify needs, make decisions and establish mechanisms to achieve solutions. For most communities at the local level, the level of involvement in palliative care programs will be at level 5 or lower in Pretty's typology [18, 19]. These projects usually have some form of community advisory board or committee, although they have limited decision-making capacity as these are dictated by the funding agencies. This makes it difficult to sustain the programs, as doing so, beyond funding, without the community having a real sense of involvement in decision-making is very difficult.
For the palliative care programs with higher levels of community participation, Suresh Kumar [17] detects some barrier focus on proactively building support networks within communities:
- Inadequate preparation: there are social and political challenges in setting up a community participation programme, including the diversity and inequalities in communities, knowing the social and political dynamics of the community, understanding and defining how communication between the facilitating team and the community will take place, knowing the values, beliefs and policies of external stakeholders (the facilitating organisation/institution/group, including funders and the global palliative care community, as well as the neighbourhood). This requires acquiring competencies through training programs.
- Different stages of the community development process: Different challenges within and outside the program structure that require different skill sets and approaches from facilitators.
- Organic nature of the community: It is difficult to decide who represents the community as it is not homogenous and is made up of different and sometimes conflicting interests. The main obstacles to developing and sustaining community partnerships are the voluntary nature of community participation, the enormity of the task and the natural conflict between community groups with different agendas and priorities. Community interventions are related to the social dynamics of the community, including power relations, economic conditions and vulnerabilities. Ongoing dialogue, learning and review mechanisms are necessary as communities evolve, adapting to changing interventions and contextual realities.
- Time constraints: Time constraints linked to grants often mean that there is insufficient time to adequately understand the community, engage multiple stakeholder groups with competing priorities and maintain project dynamism.
- Political issues and conflicts of interest: Differences in priorities and values between external experts/facilitators and the local community can lead to struggles for power and control of programs.
- Community participation policy: Empowerment of the local community is necessary. Empowerment is a multi-level concept that describes a process of social action to put people in control of their lives, their organisations and the lives of their communities. Through organisation and mobilisation, communities can achieve the social and political changes necessary to address their difficulties.
- Evaluation: It is not easy to track, document and monitor the process of community mobilisation. It is often not possible to do this using a standard research methodology (cause-effect) but rather a cascade methodology to measure impact.
Sirianni et al. [20] explored the possible difficulties in adopting a comprehensive approach in the community. They found "fragmented care" and difficult access resulting in instability and point to the need for policy involvement at all levels, state, provincial and local, along with the involvement of quasi-governmental agencies and non-profit organizations. They state that there is a need for the integration of a comprehensive, multi-level, multi-system approach to pallative care with well-resourced, palliative care-trained health care staff, public investment in palliative care services, financial support for patients/families, significant public literacy about the role of palliative care, and the implementation of a Compassionate Communities model at the national level. This approach involves a health promotion perspective on palliative care, harm reduction and early care for the patient and caregivers, with the involvement of health care providers, non-profit groups, faith-based groups, community organizations and public health providers to address both holistic patient care and public education about dying. They suggest that this comprehensive public health approach to palliative care can help with access, equity and cost.
Community attitudes towards palliative care, death and preferences at the end of lifeCollins et al. [21] described community understanding and attitudes towards palliative care and explore the characteristics significantly associated with favourable attitudes towards palliative care, understanding it as an enabler for public engagement. They found firstly, that public education programs can change attitudes towards, and thus community participation in, palliative care, and secondly, that there are knowledge gaps about palliative care in the community, which may limit access.
Abba et al. [22] conducted a follow-up study of a community intervention aimed at improving communication of end-of-life preferences and normalising death as a topic of conversation. Their intervention consisted of presentations and workshops aimed at community groups and people working in health and social care. Participants completed a survey in three phases: at baseline, after and three months after the intervention. There was a statistically significant association between increasing age group and having talked about end-of-life wishes. Most participants were already comfortable talking about the end of life.
Tieman et al. [23] state that ageing population, progressive diseases and end-of-life needs in hospitals and healthcare systems have a major impact on society. This has led to calls for public engagement with death and dying to encourage active participation in decision-making, community care and acceptance of death as a natural part of the life cycle. They carried out an intervention with the aim of allowing participants to discuss and learn in an open and supportive way about death-related issues, explore societal views and determine the effect that the online learning and discussions offered through the mediation had on participants' feelings and attitudes towards death and dying. The results showed that the mediation provided an opportunity to capture the views and perceptions of the community around death and dying, which they consider indispensable for the development of community resources and engagement.
Graham-Wisener et al. [6] consider that the main issue to involve the community in palliative care is the conversation about death and dying, which is aligned with the 'new public health approach' within palliative care. A key aspect is the normalisation of dying and the preparation of communities for the end of life. However, a significant proportion of adults report not feeling comfortable discussing death and dying with family and friends. This normalisation involves becoming 'death literate', which is defined as a set of knowledge and skills that enable end-of-life and death care options to be accessed, understood and acted upon.
Importance of volunteers in public engagement programsThree of the selected studies specifically discuss the importance of volunteers from the perspective of a public engagement approach to palliative care.
Pesut et al. [24] stated that volunteers providing supportive navigational services during the early phase of palliative are a feasible way to foster a compassionate community approach to caring for an ageing population. They piloted a compassionate community approach to early palliative care in several communities in Canada. They tested a capacity-building model in which volunteers and a nurse partnered to provide navigation support from the early palliative phase for adults living in the community, with the goal of improving quality of life by developing independence, engagement and community connections. Seven volunteers partnered with 18 clients. Throughout the trial year, volunteer navigators made home or phone visits every two to three weeks. Volunteers felt well prepared and found the role fulfilling and meaningful. Clients and their families felt that the service was very important to their care because the volunteer helped them to make the difficult experiences of ageing and advanced chronic illness more bearable. The most important benefits cited by clients were making good decisions for both the present and the future, having a substitute social safety net, supporting engagement with life, and ultimately transforming the experience of living with the disease.
Grace Warner et al. [25] conducted a qualitative study with the aim of using the Consolidated Framework for Implementation Research (CFIR) to explore barriers and facilitators to the implementation of a community-based volunteer program called Nav-CARE (Navigation-Connecting, Accessing, Resourcing, Engaging) for older adults with a serious health condition. They conducted qualitative individual and group interviews to examine the implementation of Nav-CARE in a Canadian community. Participants were individuals who conducted or managed NAv-CARE research, and stakeholders who provided services in the community. The results were organized into five themes that reflect participants' perceptions of Nav-CARE implementation:
1. Intra-organisational perceptions. Volunteers felt that they could provide information, new knowledge and a decrease in social isolation. Staff felt that the incorporation of volunteers could redistribute some of the workload, improve access to psychosocial support for the patient and their family. They expressed concern about boundary issues between the roles of volunteers and health professionals.
2.Public and health professionals' perceptions of palliative care. Stereotypical perceptions of palliative, misunderstandings in the community and health sector about who can access palliative, when and what palliative care involves. The public understands palliative care as synonymous with near death. Consequently, the programme associated with palliative care may be misinterpreted as appropriate only for people who will die in the near future. They see a need to "reframe" the perception of palliative care through community education and training. In addition, health professionals seemed to believe that palliative care should only be considered in the last months of life. Professionals recognised that it was their responsibility to educate the community about the need for early palliative care and the role of hospices. They emphasised that they should take a leadership role in promoting connections between hospices and community organisations to reduce fragmentation of care.
3. Partnerships and relationships between organisations. Participants expressed the need to educate and build relationships with community partners (e.g. pharmacists) with programmes (e.g. recreation centres) and with community groups that provide related services, such as a local caregiver support group. Building stronger partnerships between primary care and advanced palliative care teams with the idea of a 'shared care' model that is part of a palliative approach to care. Also, increased awareness in primary care practices of the need for end-of-life discussions. Engagement declined over time and health professionals did not fully understand the role of volunteers in patient care and that they lacked professional qualifications.
4.Factors at EU and national level. Development of resources, guidelines and training to help implement a palliative care approach in primary care. Creation of national legislation on medical assistance in dying (AMD). Lack of services made it difficult for primary care providers to consider referring patients to the programme.
5.Suggested changes to the programme. Several participants suggested several modifications to increase participation, such as facilitating paperwork, increasing training and internships, and increasing accessibility through Health Centres and churches. Loth et al. [26] published an exploratory study of palliative volunteers across Africa. They invited palliative care experts from 30 African countries to participate in an online survey consisting of 58 questions on: socio-demographics, activities, motivation and coordination of volunteers, and an assessment of recent developments in volunteering. Twenty-five respondents from 21 countries participated and the results showed a wide range of volunteering in palliative care. They identified volunteers as people between 30 and 50 years old, mainly non-professional women, motivated by altruism, a sense of civic engagement and personal benefit. They state that palliative care benefits from volunteers who take on a heavy workload and are close to patients and point to the main challenges of volunteer programs, problems of funding and motivation in the long term.
Compassionate communitiesThe key elements for Compassionate Communities or Cities development models shared by several authors are social awareness and education programs on compassion and networks of care [27, 28], programs for training caregivers, neighbourhood network in palliative care [29] to provide home-based palliative care involving volunteers and the community and networks of care round people at the end-of-life initiatives with the implication of inner and outer networks, communities and service delivery organizations [2].
Silvia Librada-Flores et al. [30] evaluated models of Compassionate Communities and Cities (CCC) development at the end of life and their methods, processes and measures to enable evaluation of the intervention. They conducted a systematic review (from 2000 to 2018) in which they selected 31 articles, 17 descriptive studies, 4 intervention studies, 4 reviews and 6 qualitative studies. A total of 11 studies were on models of BCC (Behaviour change communication) development at the end of life, 15 studies were on the evaluation of BCC programs and 5 studies were on protocols for the development of BCC programs. This review reflects the growing development of CCC that has been launched. The model described by Kellehear A [1, 31] has helped to orient these initiatives towards the elements that characterise the development of a Compassionate City. Published recommendations and coalitions on BCC development also reflect the empowerment of this movement from public health and palliative care policy in an integrative health-social-community care model.
Although this review provides interesting information on recommendations and an approach to models, methods and evaluation systems for BCC, the quality of this evidence is low or very low. Most are descriptive or proposals for future interventions based on literature reviews. There are no studies with representative samples and/or randomised methodology to provide more accurate information on the benefits of these interventions. The evolution of some of these programs, whether they are pilot programs or still ongoing, is unknown. No studies have been identified that demonstrate the opportunities or difficulties in implementing compassionate cities and communities’ projects. Furthermore, a comparison between the different initiatives developed cannot be made due to the method used and the absence of quantitative results. Despite all these limitations, these results serve to guide models on the benefits of these programs and further research is needed to clarify and improve our knowledge. As this is an emerging movement, the described experiences should also go in this direction to guide other cities and organisations [30].
The Spanish Society of palliative Care (SECPAL) published in 2020 a Monograph on Compassionate Communities at the End of Life, where more than 30 authors contribute their knowledge and experiences to create accompanying networks in schools, universities, neighbourhoods and other social organizations in order to provide support to patients with a life-limiting illness and their families [32].
The substantial difference of a Compassionate Communities Program from isolated public engagement initiatives is the articulation of an Integrated Health, Social and Community Care Model for advanced illness and end of life under an organizational system that manages, coordinates and evaluates it and with a methodology for implementation, monitoring and evaluation [33].
For the development of this Model, it is necessary to have [34]: Promoter leadership in technical, professional and economic terms; Definition of an area of coverage; Annual work plan, with a program of actions and specific objectives; Institutional collaboration; Generation of community intervention structures; Community intervention protocols and design of tools; Arrangement and activation of a network of promoting agents with material and human resources; Design of an evaluation system; Communication and dissemination of the program; and Publication of tools and results.
The aim is to raise awareness, train and intervene in the creation of networks (internal and external) and in the action of these networks for people with advanced illnesses and at the end of their lives; managing to evaluate their impact and results in terms of patient and family satisfaction, professional satisfaction, impact on health (improvement of quality of life, reduction of carer overload, reduction of depression and anxiety and increase in the average number of carers). Of this way avoiding duplication and inefficiencies in the use of available resources in the specific geographical area in which they are developed, and generating new community structures (such as community connectors, the community promoter, the dynamic commission and the socio-health commission) [34]. Several of the Compassionate Cities that are currently underway describe the barriers and facilitators to their development in the Compassionate Communities at the End-of-Life monograph [30, 32, 35]. These barriers and facilitators are collected in the Table 3.
Table 3 Barriers and Facilitators for Compassionate Communities (CC)Public Health Palliative Care International (PHPCI) [8] recommend that for a public engagement and involvement a Compassionate City should develop and support 13 key social changes and activities. PHPCI [43] recommends that, to achieve public engagement and involvement, a Compassionate City should develop and support 13 key social changes and activities. Both schools and workplaces should have guidelines, reviewed annually, on bereavement, death, bereavement and care. Churches and houses of worship should have at least one group dedicated to end-of-life care support. Hospices and nursing homes should have community development programmes that involve citizens in end-of-life care activities and programs. They should also involve museums and art galleries, hold memorial parades, promote compassionate communities programmes to engage local neighbourhoods or streets in direct care activities for their local residents living with health, aging, caregiving and bereavement crises. Create incentives to celebrate and highlight the most creative and compassionate organisations, events and individuals. Also publicly showcase through media, social media, public events by policy makers, compassionate initiatives undertaken or underway that help raise awareness about ageing, death, loss or caregiving. Establish social and political alliances that take into account the diversity of populations within the same city, neighbourhood or street. Finally, to encourage and invite evidence that institutions and organisations are working together to promote and support the development of a common understanding of ageing, death, bereavement and caregiving.
留言 (0)