
記住我






The particles most commonly used in EBRT are negatively charged electrons, which are accelerated in conventional medical linear accelerators to be applied directly or to hit a target that generates bremsstrahlung, which is used for therapy. However, electrons are particles that are not affected by the strong nuclear forces but are only subject to electromagnetic forces and belong to the family of lepton particles. The mass of an electron is 9.109 383 7015 × 10−31 kg [2], which is about 1/1800 the mass of a proton or neutron.
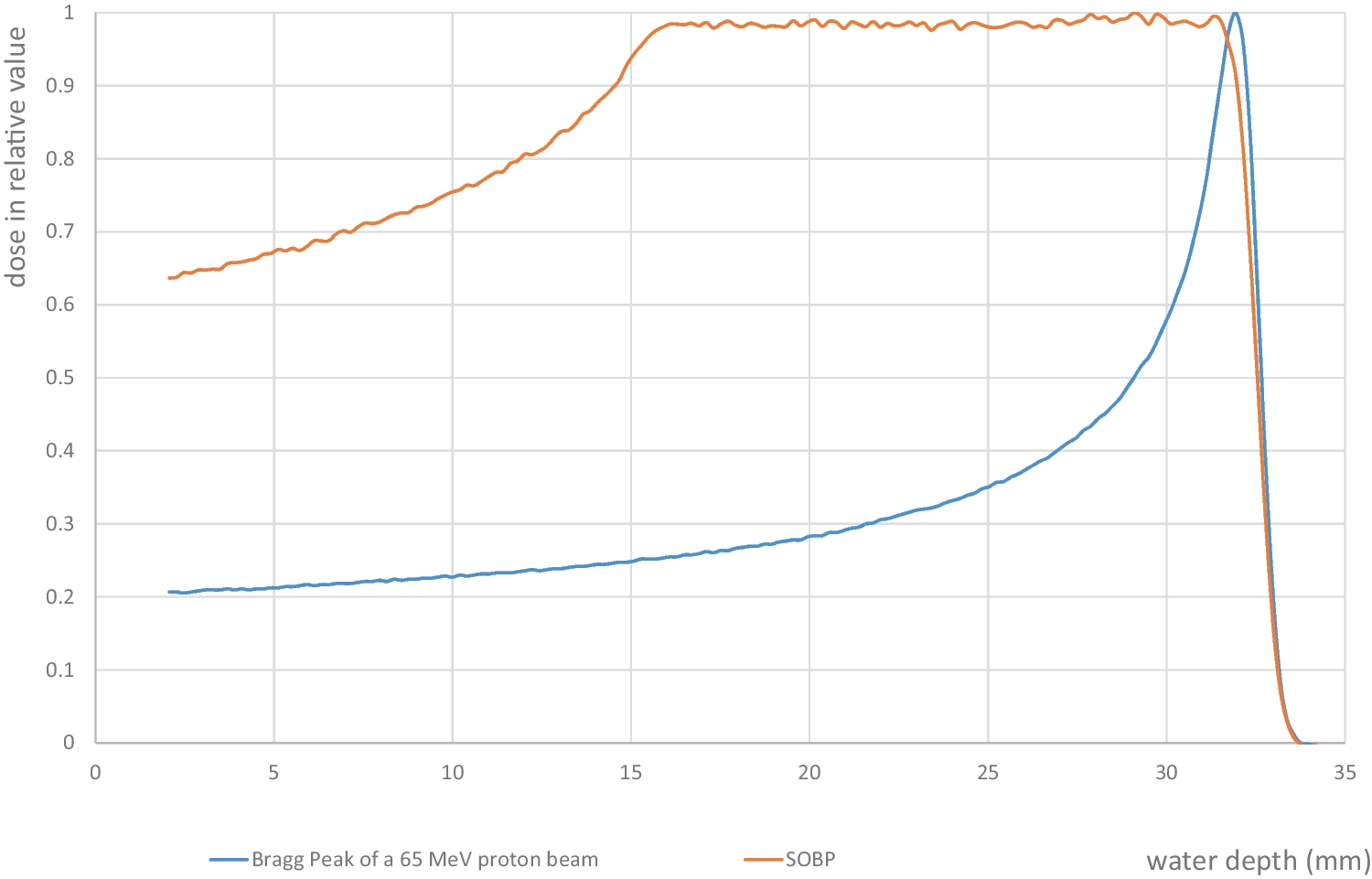
Hadrons, which are currently used for cancer therapy, are charged particles such as protons and composite particles (e.g. helium ions, carbon ions) on the one hand and uncharged particles, namely neutrons, on the other (Table 1). Possible therapeutic advantages of using charged particles result from their physical properties, especially in the depth dose distribution. The energy deposited in the tissue increases non-linearly; as the kinetic energy of the charged particles decreases, it reaches an explosive maximum ("Bragg peak") at a depth dependent on the initial energy, followed by a steep drop in dose (Fig. 1).
Table 1 An overview of particles used for irradiating malignanciesFig. 1
The blue line represents the Bragg Peak of the 65 MeV proton beam of the MEDICYC facility at the Centre Antoine Lacassagne in Nice. The orange line is the depth dose distribution of a SOBP covering a volume of 1.5 cm thickness. The graphs are measured using a silicon diode in a water tank
The LET capacity for protons is low and is around 0.5 keV/µm at the beginning of the travel distance in the tissue, where the velocity is highest. However, on the last µm of the range it reaches a maximum of approx. 100 keV/µm. For helium ions, the maximum is reached at approx. 200 keV/µm. In order to be able to irradiate a tumor with a given extent, the entrance energy is modulated in such a way that a spectrum results whose Bragg peaks are evenly distributed over the target volume, whereby a homogeneous dose distribution is achieved in the target volume (Fig. 1). This is called a spread-out Bragg-Peak (SOBP). The depth dose distribution of a monoenergetic proton beam looks extremely attractive, very low dose prior to the Bragg-Peak and no dose at all behind. However, the sum of different energies to cover the entire tumor also add up to increase the entrance dose. Moreover, protons lack the build -up effect therefore the dose to the superficial 3–5 mm of skin can be higher than that of photons. The dose to skin of a 15 MV photon beam is about 30% of the maximum dose, the dose to skin of a proton beam to treat a larger, deep-seated tumor is between 60 and 80% of the maximum dose. A clear advantage of protons is the steep drop in dose after the Bragg peak and the low lateral penumbra, both of which lead to a reduction in dose in normal tissues. The path of helium ions in tissue at depth is remarkably straighter compared to protons and this explains the increasing interest in this particle for a further optimized dose distribution compared to protons.
Carbon ions were introduced into clinical practice in 1994 by the National Institute of Radiological Sciences (NIRS) in Chiba, Japan, with the Heavy Ion Medical Accelerator (HIMAC). Carbon nuclei are 12 times heavier than protons and have a high LET value, which makes them a fascinating modality for the treatment of large, hypoxic and radioresistant tumors. Moreover, carbon ion LET can be considered high only in the last portion of their path so they can be used to apply high LET radiation in the target volume without exposing the uninvolved tissue in the entrance channel to high LET. Compared to fast neutron therapy, which was the first high-LET radiation modality used to treat cancer [3], the dose distribution can be applied with higher precision. Compared to protons and helium ions, the depth dose distribution of carbon ions is more complex and the end of the range after the SOBP is less precise due to the fragmentation of some of these large particles into smaller ions. The LET of a carbon ion beam is different from one voxel to another, which explains the need for using models to calculate the applied dose. Unfortunately, different models are used for calculating the RBE-weighted dose which make it difficult to compare the dose values reported in the different countries [4, 5]. Currently carbon ion beams are available in only few countries (South-East Asia and Europe). They have been used with excellent results in many tumors where local control was difficult to achieve with other modalities [6, 7].
For clinical applications, 2 different qualities of neutrons must be distinguished by their kinetic energies, which lead to different interactions with matter. Fast neutrons (for medical purposes in the range of 1 MeV -18 MeV) essentially interact through elastic and inelastic scattering. The effect of elastically scattered neutrons on the water molecules in tissue produces recoil protons, which in turn represent the ionizing radiation that causes biological effects. Thermal neutrons (E ≤ 0.5 eV) lead to nuclear reactions. Both neutron qualities are used for cancer treatment Fast Neutron Therapy (FNT) and Boron Neutron Capture Therapy (BNCT) respectively. Already shortly after the discovery of the neutron by Chadwick in 1932 [8], their use against cancer has been proposed. Stone and Larking carried out the first treatments with FNT as early as 1938, which led to poor results [9, 10]. After very extensive radiation biological investigations, FNT restarted in the 1960s with great enthusiasm and amazing good tumor response [11]. The challenge in fast neutron therapy was the selection of the tumor entities that are expected to benefit from the differential action of high LET radiation on tissues. An evidence-based advantage of FNT over low LET irradiation has been established in clinical trials for well-differentiated salivary gland tumors [11]. However, an increased appearance of unexpected late effects on normal tissues observed after an observation period of some years was used as an argument against FNT [3]. These late severe toxicities were controlled by advanced treatment planning and optimized beam delivery (e.g. isocentric gantries, multileaf collimators, intensity modulated fast neutron therapy). Nevertheless, the bad reputation of fast neutrons was overruling the good results obtained by a rapidly decreasing number of centers and carbon ions are replacing them [12, 13]. Nowadays only one place in the world offers a fast neutron beam fulfilling all modern requirements (University of Washington Medical Cyclotron Facility).
Thermal neutrons are needed for Boron Neutron Capture Therapy (BNCT). The basic idea to use neutron capture reactions in cancer treatment was published by Locher in 1936 [14]. Early BNCT trials in the 1950ies also were not leading to clinical success [15]. After successful pioneering work in Japan by Hiroshi Hatanaka using thermal neutrons at a research reactor for intraoperative BNCT [16, 17] international efforts restarted [16]. Despite promising clinical observations, the impact of BNCT has so far remained low, as the required radiation quality was only available at research reactors [18]. Recent developments in accelerator technology are now making BNCT facilities available in hospitals, marking a new and hopefully successful start for this auspicious modality. We are observing a rapidly growing number of such systems and hope to see the results of modern controlled, prospective clinical studies.
留言 (0)