
記住我








Abdominal aortic aneurysms (AAAs) have a global prevalence of 4.8%,1 and although the majority are asymptomatic, they are a common finding, detected either incidentally or through screening programs.2,3 Current management of asymptomatic AAA is primarily determined by maximum aneurysm diameter and growth rate, the only aneurysm-specific factors known to be associated with increased risk of rupture,4,5 the mortality of which exceeds 80%.6 Elective surgical or endovascular repair to preempt rupture is recommended when AAAs reach a diameter of 5.5 cm in men or 5 cm in women, or at smaller diameters if the growth rate exceeds 1 cm/y.7 Abdominal aortic aneurysms not meeting repair thresholds are imaged at 6-month to 3-year intervals, depending on diameter.7 Although practical, risk stratification of AAA based on maximum diameter and growth is both resource-intensive and imprecise. Approximately, 10% of AAAs rupture before reaching diameter thresholds for repair,8,9 and up to 40% of ruptures occur in AAA that are below repair thresholds at last surveillance.8–11
Recent studies have suggested that aortic wall biomechanical properties may be associated with AAA progression.12–15 Aortic wall strain and distensibility, the latter being derivable from wall strain and pulse pressure, are accessible measurements reflecting these properties, and may thus be useful for risk stratification.16,17 In vivo, AAA strain has been assessed via speckle tracking ultrasound18–20 and MR displacement encoding with stimulated echoes,21 whereas stiffness has been assessed by MR elastography.22–24 However, these methods require specialized MR system software and/or hardware and significant technical expertise, considerably limiting their clinical utility. Furthermore, to date, only MR elastography–derived AAA stiffness has been studied with regard to AAA progression.23
A variety of techniques have been developed to measure myocardial strain from standard cardiac-gated cine MR images without the need for special pulse sequences or imaging system hardware. Many of these techniques track imaging features of tissues (particularly endocardium) across cardiac phases to estimate tissue strain.25–32 One method with excellent reproducibility29–32 uses a deformable registration algorithm (DRA) to track the displacements of all image voxels,29 rendering it ideally suited for thin vascular walls that are difficult to delineate and track independent of their surrounding tissue. The goals of this study were to (1) establish the accuracy of AAA MR strain measurements using a DRA-based technique applied to simulated cine magnetic resonance imaging (MRI) of an AAA with a priori known ground truth strain and (2) to study the relationship between MR strain and AAA progression in a patient cohort with 6 months to 2 years of prior surveillance imaging.
METHODSThis single-center study was approved by the institutional review board of the facility and was compliant with the Health Insurance Portability and Accountability Act. Written informed consent was obtained for all patients except when the institutional review board waived the requirement for informed consent on the basis of a solely retrospective review of previously acquired clinical data.
In Silico Synthetic Cine MRI With Ground Truth AAA StrainA finite element model (FEM) was created from the end-diastolic cine MR image of the abdomen of a patient with a 4.7-cm AAA (Fig. 1A) to study the accuracy of AAA MR strain measurements. Briefly, the model included the aortic lumen, intraluminal thrombus (ILT) and aortic wall, periaortic fat, lumbar vertebral body, and bowel loops, with the remaining abdominal domain assigned to either intra/retroperitoneal fat or extraperitoneal tissue (Fig. 1B). Tissues and air were modeled as isotropic linear elastic materials with elastic moduli and densities derived from literature or chosen to match tissue deformations seen in the original in vivo cine MRI (Table 1). Poisson ratios in the range of 0.45–0.48 were used to account for the near incompressibility of biologic materials (Table 1).
 FIGURE 1:
FIGURE 1: In vivo cine MRI of AAA from which the FEM model was derived (A). Simplified model of the abdomen used in FEM simulations (B). L, aortic lumen; B, bowel; V, vertebral body; periaortic fat (asterisk); aortic wall (dagger); intraluminal thrombus (double dagger).
TABLE 1 - Tissue Material Properties Used for FEM Simulation Tissue Young Modulus, N/cm2 Density, kg/m3 Poisson Ratio Notes AAA wall 235 2000 0.48 Tangential modulus at 100 mm Hg ILT 50 1300 0.48 Chosen to match luminal distension in original in vivo cine MR, assuming 40 mm Hg pulse pressure Periaortic fat 0.4 920 0.42 Chosen in tandem with applied forces to approximate AAA anteroposterior motion and pulsatility of AAA in original cine Intra/retroperitoneal fat 0.5 920 0.45 Chosen in tandem with applied forces to approximate bulk breathing and AAA/bowel loop motions in original cine Extraperitoneal tissue 0.3 920 0.48 Chosen in tandem with applied forces to approximate breathing motion in original cineFEM, finite element model; AAA, abdominal aortic aneurysm; ILT, intraluminal thrombus; MR, magnetic resonance.
Dynamic FEM simulations of 1 cardiac cycle of 0.81 seconds' duration were performed using Abaqus (Version 2021; Dassault Systemes, Simulia Corp, Vélizy-Villacoublay, France) using implicit time integration with maximum time step of 0.01 seconds. Boundary conditions were applied to simulate a range of physiologic conditions and included the following: (1) a general aortic pressure waveform with pulse pressures of 20–80 mm Hg, (2) traction forces applied in tandem with the pressure waveform to the periaortic fat to reproduce the bulk anteroposterior motion of the aorta seen in vivo, and (3) a 3 Fourier component pressure waveform applied within bowel loops to approximate physiologic bowel motion. Traction forces and bowel loop pressures were applied so as to achieve between −45% and +15% of the deformations seen in the in vivo cine MRI. The posterior edge of the lumbar vertebral body and the dependent edge of the extraperitoneal tissue (skin surface) were fixed in all directions. In total, the boundary condition combinations resulted in 13 distinct FEM simulations, each with a ground truth value of aortic wall strain (Supplemental Table S1, https://links.lww.com/RLI/A874).
For each simulated physiologic condition, a synthetic cine MRI series with 25 image frames over the simulated cardiac cycle was produced according to the evolution of the FEM mesh through the simulation. This was achieved by first sampling the original end-diastolic MR image at the locations of the nodes of the FEM mesh using interpolation. Then, for each simulation time step coinciding with a cine MRI image frame, the FEM mesh node locations evolved to that time step were used to resample the nodal signal intensities onto a rectilinear grid with the same pixel spacing as the original image. The synthetic cine images were then augmented with (a) 3 levels of aortic and bowel lumen signal intensity variation through the cardiac cycle ranging from no variation to 20% increase of the baseline intensity distribution, and (b) 4 levels of Gaussian image noise producing signal-to-noise ratios roughly equal to 25% to 100% that of the original cine MRI. Signal intensity variations in the aortic lumen were applied in tandem with the aortic pulse pressure waveform to reflect inflow of unsaturated blood during the cardiac cycle, whereas those in bowel loops were based on a 3-component Fourier waveform approximating the variation of signal intensities seen in vivo.
In total, 54 synthetic cine MRI series were produced from the 13 FEM simulations. Supplemental Video 1, https://links.lww.com/RLI/A875, demonstrates one example of these synthetic MRI series. The full matrix of FEM simulation and synthetic MRI parameters considered are provided in Supplemental Table S1, https://links.lww.com/RLI/A874.
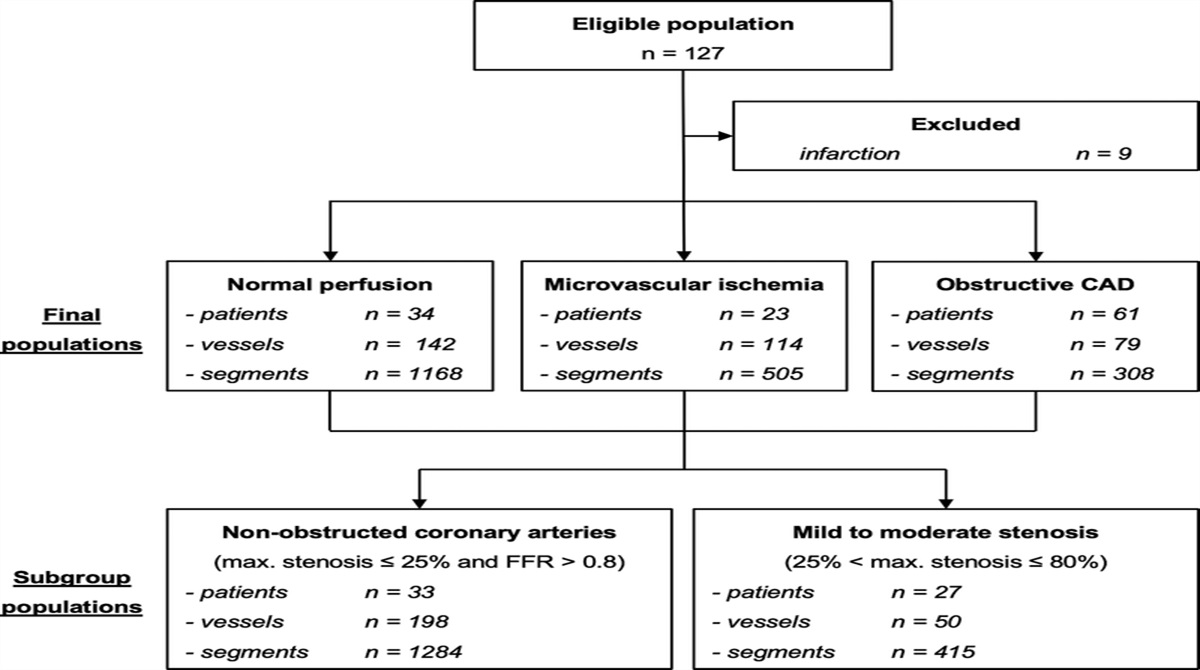
In Vivo Patient Study Study ParticipantsThis study enrolled consecutive patients referred for AAA surveillance between July 2021 and March 2023 with at least 1 prior MRI or computed tomography (CT) study of the abdomen at least 6 months and no more than 2 years prior. Magnetic resonance imaging and CT are used at nearly equal rates for most regular AAA surveillance studies at our institution. Prespecified exclusion criteria were history of vasculitis (n = 0), connective tissue disorder (n = 0), or dissection (n = 1).
Magnetic Resonance ImagingAll imaging was performed on a 3 T MRI system (Skyra; Siemens Healthcare, Erlangen, Germany). For the purposes of this study, pulse-gated cine balanced steady-state free precession (bSSFP) acquisitions were performed for strain measurement at 2 abdominal aortic locations orthogonal to the vessel course. One was acquired at the level of maximum AAA diameter, and the other in the normal caliber abdominal aorta proximal to the aneurysm neck. Cine imaging parameters were the following: 12 segments per effective TR, TE/eff, TR = 1.43/39.24 milliseconds, parallel acceleration factor = 3, field of view = 340 × 284 mm2, acquisition matrix = 256 × 200, reconstructed voxel size = 1.33 × 1.33 mm, slice thickness = 6 mm, flip angle = 44–46 degrees, bandwidth = 960 Hz/pixel, and 25 frames/cardiac cycle. A postcontrast 3-dimensional fast gradient-echo stack-of-stars volumetric interpolated breath-hold examination (Star-VIBE) sequence included in our standard surveillance protocol was used for AAA diameter measurements (see below). The parameters for this sequence were the following: coronal acquisition plane, 96 slices, 320 mm field of view with 8 radial spokes reconstructed at 1.25 mm isotropic resolution, TR/TE = 24.67/1.99 milliseconds, and flip angle = 9 degrees. Finally, participants were instrumented with an MR-compatible sphygmomanometer, which was used to measure blood pressure just before the acquisition of the AAA cine series.
Maximum AAA Diameter and Growth Rate Calculation of Study ParticipantsTwo imaging scientists (H.D. with 8 years of experience, and A.Z. with 5 years of experience in cardiovascular image analysis) under the supervision of a board-certified abdominal radiologist (J.L. with 10 years of experience) measured the maximum AAA diameter in all CT and MRI studies of each study participant over the preceding 2 years. Measurements were performed using commercial 3-dimensional postprocessing software (Vitrea Version 7.14; Vital Images, Minnetonka, MN) orthogonal to the vessel centerline using multiplanar reformation.33 To maximize precision of the outcome variable studied in this work (maximum AAA diameter growth rate), the maximum AAA diameter measurements of the 2 readers for each imaging study were averaged. Growth rate was then calculated by linear regression of the average maximum AAA diameters over time.
Aortic Circumferential MR Strain MeasurementStrain quantification of both synthetic in silico and in vivo cine MRIs was performed using a work-in-progress software package (TrufiStrain,* Version 3.0; Siemens Healthineers, Erlangen, Germany) based on a DRA. This technique computes a symmetric and inverse-consistent dense deformation of the image between cardiac phases, minimizing a local cross-correlation similarity metric and using a spatial smoothing regularization.34 It then uses the computed deformations to derive the radial and circumferential strains of any set of operator-selected voxels. We used this method to extract the circumferential strain of the voxels underlying a cubic spline-interpolated, manually drawn curve placed just inside the visible outer edge of the aorta by the operator. This approach is informed by the typical AAA wall thickness of 1.2–2.5 mm,35 ensuring that the selected voxels contain primarily AAA wall tissue with minimal partial volume effects (given the 1.3 mm voxel size). The curve was drawn by the operator in a single cine image frame of their choice and was then automatically propagated to the remaining frames based on the DRA solution. For the purposes of this study, the operator visually confirmed that the propagated curve indeed remained on the edge of the aorta in all remaining frames. For analysis, we calculated the peak strain over the cardiac cycle as the difference between systolic and diastolic strains. For the synthetic cine MRIs, the aortic wall curve was delineated at the end diastolic frame by the abdominal radiologist, and the same curve was used for all synthetic MRIs as the FEM boundary conditions ensured this frame was identical across all simulations. For in vivo cine MRIs, 1 cardiovascular imaging scientist delineated the aortic wall in an image frame of their choice for each subject. A second imaging scientist also delineated the wall independently, so that interoperator reliability could be assessed.
Statistical AnalysisStatistical analyses were performed in Stata (Version 12.1; StataCorp, College Station, TX). A 2-tailed P value of less than 0.05 was considered significant.
Characterization of MR Strain AccuracyEach of the 13 FEM simulations possessed a ground truth value for the peak wall strain. However, for each simulation, multiple MR strains were measured, one from each synthetic cine MRI series corresponding to the different noise and signal intensity variations simulated. For each of the 13 ground truth settings, we assessed the mean pairwise difference (ie, bias) between the measured MR strains and the corresponding ground truth strain setting and 95% confidence interval (95% CI). We also assessed dependency of the mean pairwise differences on the ground truth strain magnitude via Pearson correlation.
Association of In Vivo MR Strain and AAA Growth RateWe studied the association between the observed AAA growth rate and a number of explanatory variables using univariate linear regression. The following explanatory variables were considered: peak MR strain of the AAA as well as the normal caliber aorta and their ratio; maximum AAA diameter; mean aortic pressure and pulse pressure at the time of the MRI since pressure load is the primary driver of strain; presence of ILT (yes/no) and amount of periaortic abdominal fat (categorized as moderate or high, based on qualitative visual assessment) as these may also affect aortic wall strain; and finally, factors with established relationships to AAA progression, namely, diabetes mellitus, hypertension, and smoking (yes/no for both ever smoker and current smoker). We then performed a multivariable regression including all variables found to have a statistically significant association to growth rate in the univariate models, additionally controlling for maximum AAA diameter.
Interoperator Agreement of In Vivo MR Strain MeasurementsWe determined the mean of the pairwise differences (bias) with 95% CI of MR strain measurements performed by the 2 imaging scientists. We also calculated the intraclass correlation coefficient and the coefficient of variation (CoV; calculated as the within-subject standard deviation divided by the mean measurement).
RESULTS Association of DRA-Based Strain to In Silico Ground Truth StrainThe peak circumferential aortic wall strain in the 13 FEM simulations ranged from 0.66% to 2.41%, whereas the DRA-measured strains measured from the 54 synthetic cine MRI series generated from these simulations ranged from 0.75% to 3.03%. Figure 2A shows the correlation between the ground truth FEM strain and the average MR strain measured from all synthetic MRIs corresponding to each FEM simulation. The slope of the regression was 0.963 (95% CI, 0.873–1.052; P < 0.001). The mean pairwise difference between ground truth and MR strain across the 54 simulated MRIs was −0.48%, with 95% CI of −0.90% to −0.06%, shown in Figure 2B. That is, 95% of MR strain measurements are expected to be within −0.48% ± 0.42% of the ground truth strain. Furthermore, the difference between ground truth and MR strains was independent of strain magnitude (P = 0.887, Fig. 2B), indicating that difference is systematic and does not change over the range of physiologic AAA strains investigated.
 FIGURE 2:
FIGURE 2: Association of MR strain measured from 54 synthetic cine MRIs generated from 13 in silico FEM simulations of an AAA, as described in the text (A). Error bars indicate the standard deviation of the MR strain across multiple synthetic MRI series with different levels of noise and aortic and bowel intraluminal signal intensity variations generated from each FEM simulation, as described in the text. Pairwise differences of ground truth and MR strains with bias, 95% confidence intervals, and linear regression of the differences with respect to strain magnitude (B).
In Vivo Study Participant Characteristics, MR Strain, and AAA ProgressionTwenty-five AAA patients (all male) were included in this study. Patient characteristics are provided in Table 2. On average, participants had 3±1 (range, 2–5) imaging examinations in the 2 years preceding the cine MRI, resulting in a mean follow-up interval of 1.5 ± 0.4 years (range, 200–757 days). During this follow-up, AAAs grew at an average rate of 2.1 ± 1.2 mm/y, from a diameter of 42.0 ± 9.1 mm at the baseline study to 45.0 ± 10.3 mm at the time of the cine MRI acquisition. At the baseline study, 1 AAA had a diameter >5.5 cm, measuring 5.6 cm, whereas at the time of the cine MRI acquisition, 6 AAAs had a diameter >5.5 cm.
TABLE 2 - Patient Characteristics (n = 25) Age, y 75.6 ± 5.7 Male sex, n 25 (100%) Maximum AAA diameter at baseline, mm 42.0 ± 9.1 Maximum AAA diameter, mm 45.0 ± 10.3 Growth rate, mm/y 2.1 ± 1.2 Follow-up interval, d 537 ± 162 AAA circumferential MRI strain, % 1.2 ± 0.6 Remote normal aorta circumferential MRI strain, % 2.4 ± 1.7 Remote normal aorta/AAA MRI strain 2.3 ± 1.6 Mean aortic pressure at scan, mm Hg* 91.8 ± 13.5 Pulse pressure at scan, mm Hg* 48.8 ± 13.8 Hypertension, n† 15/24 (62.5%) Diabetes mellitus, n† 4/24 (16.7%) Ever smoker, n† 15/24 (62.5%) Current smoker, n† 4/24 (16.7%)*Data not available for 3 patients.
†Data not available for 1 patient.
AAA, abdominal aortic aneurysm; MRI, magnetic resonance imaging.
The mean peak circumferential strain of the aortic wall measured by the DRA technique was 1.2% ± 0.6% (range, 0.4%–2.4%) at the site of AAA maximum diameter versus 2.4% ± 1.7% (range, 0.7%–7.2%) at the level of the proximal nonaneurysmal aorta. The mean pairwise difference in peak MR strain between the 2 sites was 1.2% ± 1.3% (range, −0.6% to 5.0%) and was statistically significant (Wilcoxon sign rank test, P < 0.001). Figure 3 demonstrates the aortic wall circumferential MR strain over the cardiac cycle of the aneurysm and the normal-caliber proximal aorta of a representative AAA patient.
 FIGURE 3:
FIGURE 3: Sample frame of the cine MRI obtained at the level of the proximal, nonaneurysmal aorta (A), and the AAA (B) in 1 patient with a AAA 2-year growth rate of 1.1 mm/yr. Strain through the cardiac cycle of the tissue in voxels underlying the wall boundary demarcated in the cine images (yellow curves in panels A and B) was measured from the cine MRI using a deformable registration algorithm (C).
A lower MR strain was observed with increasing AAA diameter, ranging from 1.4% ± 0.6% for AAA < 45 mm, to 1.0% ± 0.4% for AAA ≥ 45 mm and <55 mm, and 0.7% ± 0.2% for AAA > 55 mm in maximum diameter (Fig. 4). The difference between MR strain of AAA < 45 mm versus those >55 mm in maximum diameter was statistically significant (1-way analysis of variance, P = 0.010). Univariate analysis revealed that maximum AAA diameter and peak MR strain were significantly associated with growth rate (Table 3, Fig. 5). In the multivariate model controlling for maximum AAA diameter, peak AAA strain remained statistically significantly associated with growth rate (Table 3). According to the fitted model, a reduction of 1.1% in peak AAA MR strain and an increase of 17.9 mm in maximum AAA diameter were each independently associated with a 1 mm/y increase in growth rate (P = 0.014 and P = 0.006, respectively, Table 3).
 FIGURE 4:
FIGURE 4: Peak circumferential AAA strain measured by cine MRI DRA analysis, grouped by maximum AAA diameter.
TABLE 3 - Association of AAA Growth Rate With Clinical and MRI Variables Variable Univariate Models Multivariable Model β 95% CI P β 95% CI P Age −0.046 −0.135, 0.043 0.293 — — — DM* 1.155 −0.025, 2.334 0.055 — — — HTN* −0.800 −1.723, 0.124 0.086 — — — Smoking* Ever 0.256 −0.772, 1.284 0.609 — — — Current 1.242 −0.025, 2.508 0.054 — — — Maximum AAA diameter 0.087 0.054, 0.120 <0.001 0.056 0.018, 0.094 0.006 Presence of ILT 0.664 −0.79, 1.706 0.123 — — — Abdominal fat −0.373 −1.484, 0.739 0.495 — — — AAA MRI strain −1.563 −2.194, −0.932 <0.001 −0.904 −1.609, −0.200 0.014 Normal aorta MRI strain −0.144 −0.448, 0.159 0.336 — — — Normal/AAA strain ratio 0.206 −0.507, 0.462 0.111 — — — Mean aortic pressure† 0.004 −0.036, 0.044 0.827 — — — Aortic pulse pressure† −0.033 −0.069, 0.003 0.071 — — —*Data not available for 1 patient.
†Data not available for 3 patients.
AAA, abdominal aortic aneurysm; MRI, magnetic resonance imaging; CI, confidence interval; DM, diabetes mellitus; HTN, hypertension; ILT, intraluminal thrombus.
 FIGURE 5:
FIGURE 5: Association of AAA growth rate and peak circumferential strain measured by cine MRI DRA analysis after adjusting for maximum AAA diameter.
MRI Strain Interoperator AgreementThe mean pairwise difference (bias) in MR strain measurements by the 2 readers was 0.03% with 95% CI of ±0.31%. The CoV was 7.14%, and the intraclass correlation coefficient was 97.8% with 95% CI of 95.1% to 99.0%.
DISCUSSIONThis study measured the global circumferential AAA wall strain using a DRA analysis of standard, readily available cine MRI and assessed its accuracy and relationship to AAA progression. In silico simulations showed an excellent correlation between the cine MR-measured strain and the ground truth. In vivo, AAA peak circumferential MR strain had high interobserver reproducibility. Abdominal aortic aneurysm wall tissue seemed to be stiffer than the nonaneurysmal proximal abdominal aorta, which on average had a 2.3-fold higher MR strain. Finally, a lower MR strain was observed in AAA that had exhibited a higher growth rate over an average follow-up of 1.5 years, independent of maximum AAA diameter. Together, these results suggest that MR strain may be sufficiently sensitive to detect differences in aneurysm wall mechanical properties and that this information may be useful toward patient-specific assessment of progression risk.
To the best of our knowledge, this is the first study to validate AAA wall strain measured by MRI and the first study to use a “digital patient twin” to perform such a validation. The digital twin was based on an FEM simulation of a patient's abdomen with precisely known aortic wall strains, controlled via operator-prescribed boundary conditions of the aortic pulse pressure and forces related to the physiologic motion of the abdominal aorta and other structures. By analyzing synthetic MR images generated from this digital twin, we found that the peak circumferential strain of the aortic wall measured using the DRA approach had excellent correlation with its true value, although it was systematically overestimated by 0.48% and varying by ±0.42% around this biased estimate when image characteristics unrelated to tissue strain, such as noise and inflow enhancement in the aortic lumen, were altered.
In vivo, we observed a peak circumferential AAA MR strain of 1.2% ± 0.6%. This is in good agreement with a previous report of 1.5% ± 0.6% using speckle-tracking (ST) ultrasound (US).36 That study also reported a 3.1-fold higher strain in aortas of normal controls. In comparison, we observed a 2.3-fold higher MR strain in the nonaneurysmal proximal abdominal aorta of AAA patients. A larger ST US study reported a median peak circumferential strain of 1.0% (interquartile range, 1.0%–1.75%) and a 2-fold higher median strain in normal aortas.37 In comparison, the median AAA strain in our study was 1.0% (interquartile range, 0.7%–1.6%), whereas the proximal nonaneurysmal aorta median strain was 2.2-fold higher. A third ST US study previously reported that AAA peak circumferential strain trended lower with increasing diameters up to 6.5 cm, namely, from 3.89% for AAA <4.5 cm to 2.75% for AAA between 4.5 cm and <5.5 cm, and 1.8% for AAA between 5.5 cm and 6.5 cm.18 The in vivo AAA strains measured in our study exhibited the same trend with diameter, although with 2.7-fold lower magnitudes than that US study. The consistently larger strain magnitudes of this latter ST US study compared with other ST US studies as well as the present study may be due to the use of a higher frame rate. Importantly, however, our results suggest that relative differences in strain across AAA disease progression can still be detected despite the lower frame rate of cine MRI.
Importantly, the 1.2% difference in MR strain that we observed between the aneurysmal abdominal aorta and the normal-caliber proximal abdominal aorta was larger than the variability expected either due to image variations unrelated to wall mechanics (±0.42% from in silico experiments) or due to the interobserver reproducibility of in vivo strain measurements (±0.31% in vivo interoperator variability). This supports that DRA-based MR strain is able to detect, and hence study, differences in strain associated with the fundamentally altered mechanical properties of the aneurysmal vessel wall. The mechanical properties of the aortic wall are known to be associated with its extracellular matrix remodeling. In a normal aorta, elastin determines the wall elasticity and provides reversible extensibility, whereas less-distensible collagen fibers serve as scaffolds and prevent wall failure under high stress.38 During AAA expansion, the degenerative remodeling of elastin fibers can compromise its loading-bearing capacity, shifting the mechanical load to the much stiffer collagen and leading to a decrease in distensibility.39 An increase in distensibility in the final prerupture phase of AAA evolution has been suggested to be indicative of the final degeneration of the collagen network before rupture.40 The DRA-based MR strain may also be useful to detect such an ominous change in AAA distensibility, although further studies are needed to confirm this.
The relationship of AAA wall strain and aneurysm progression has not been previously studied with any modality. We directly associated the peak circumferential strain, maximum AAA diameter, and several clinical variables with AAA progression over an average follow-up of 1.5 years before the cine MRI study. After controlling for maximum AAA diameter, we found that a 1.1% reduction in peak circumferential strain was associated with a 1 mm/y faster AAA growth. Large studies have previously associated a 1 mm/y increase in growth rate to a 1-cm increase in maximum AAA diameter.41 In turn, a 1-cm increase in AAA diameter carries a nearly 4-fold higher risk of rupture.42 Thus, if our findings are confirmed, MR strain could potentially provide important information relevant to AAA patient risk stratification used to select follow-up intervals and the timing of prophylactic repair. Moreover, the MR strain technique only requires standard cine bSSFP imaging, which is already used routinely for cardiovascular imaging and is sufficiently fast to be well-tolerated by most patients, rendering it suitable for clinical translation.
Limitations of this study include the small sample size and male-only cohort, the latter reflecting the patient population within the Veterans Affairs health care system and natural 4:1 male-to-female prevalence of AAA.43 The reproducibility and measurement accuracy may be lower in standard clinical practice conditions. However, we do not expect significant site-specific variability given that cine bSSFP imaging is a well-established MR technique used routinely in the clinic. The MR strain accuracy may also be adversely impacted by irregular heart rhythm during the MRI acquisition, although its potential impact on the utility of the technique was not assessed in the present work. A limitation of our in silico results is that we assessed MR strain accuracy using a single simulated anatomy, due to the labor involved in performing FEM simulations and analyzing the results. However, we observed that most cine imaging features unrelated to AAA pulsation, such as bulk motion or simulated peristalsis of bowel loops, had negligible effects on accuracy. Based on our results, the sole imaging feature difference that can have a potentially relevant effect on the measured MR strain is the signal intensity variation within the lumen, which is attenuated by the proximity of the AAA wall to the lumen, given the presence and extent of ILT. The majority of clinically relevant AAA possess ILT44 so that our results from this single anatomy should still be representative of the majority of AAA patients. A limitation of our in vivo findings is that we could only assess growth over the period leading up to the cine MRI study, and accordingly, our results only support that circumferential MR strain measured using a DRA technique is associated with a recent period of AAA growth. Prospective studies are needed to establish whether AAA circumferential MR strain is similarly associated with future AAA progression. It is also of interest to establish the relationship of strain with clinical outcomes, and particularly with the occurrence of rupture at diameters below the recommended repair thresholds. Nonetheless, as described above, our results support that MR strain is sensitive to aortic wall composition, whereas progression is indeed characterized by changes in wall composition. Finally, this work only studied the mean global circumferential strain of the AAA wall. Previous studies have demonstrated local variations in AAA strain that may also be useful in evaluating AAA biomechanical properties18,19 and will also be studied using MR strain in our future analyses.
CONCLUSIONSStrain reflects the dynamic behavior of the AAA wall and its mechanical properties, information that is not currently routinely accessible in a clinical setting. The present study suggests that the circumferential strain of the AAA wall can be reliably measured using readily available MRI using a deformable image registration analysis. The MR strain may offer patient-specific insight regarding regional biomechanical properties of the AAA wall, and importantly, the risk of aneurysm progression.
REFERENCES 1. Li X, Zhao G, Zhang J, et al. Prevalence and trends of the abdominal aortic aneurysms epidemic in general population—a meta-analysis. PLoS One. 2013;8:e81260. 2. Owens DK, Davidson KW, Krist AH, et al. Screening for abdominal aortic aneurysm. JAMA. 2019;322:2211. 3. Leach JR, Shen H, Huo E, et al. Impact of implicit abdominal aortic aneurysm screening in the Veterans Affairs Health Care System over 10 Years. J Am Heart Assoc. 2022;11:e024571. 4. Brewster DC, Cronenwett JL, Hallett JW, et al. Guidelines for the treatment of abdominal aortic aneurysms: report of a subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. J Vasc Surg. 2003;37:1106–1117. 5. Scott R. The multicentre aneurysm screening study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial. Lancet. 2002;360:1531–1539. 6. Bengtsson H, Bergqvist D. Ruptured abdominal aortic aneurysm: a population-based study. J Vasc Surg. 1993;18:74–80. 7. Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018;67:2–77.e2. 8. Darling RC, Messina CR, Brewster DC, et al. Autopsy study of unoperated abdominal aortic aneurysms. The case for early resection. Circulation. 1977;56(3 Suppl):II161–II164. 9. Hall AJ, Busse EFG, McCarville DJ, et al. Aortic wall tension as a predictive factor for abdominal aortic aneurysm rupture: improving the selection of patients for abdominal aortic aneurysm repair. Ann Vasc Surg. 2000;14:152–157. 10. Ahmad M, Mistry R, Hodson J, et al. How quickly do asymptomatic infrarenal abdominal aortic aneurysms grow and what factors affect aneurysm growth rates? Analysis of a single centre surveillance cohort database. Eur J Vasc Endovasc Surg. 2017;54:597–603. 11. Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ultrasound surveillance. Ann Surg. 1999;230:289. 12. Vorp DA, Vande Geest JP. Biomechanical determinants of abdominal aortic aneurysm rupture. Arterioscler Thromb Vasc Biol. 2005;25:1558–1566. 13. Indrakusuma R, Jalalzadeh H, Planken RN, et al. Biomechanical imaging markers as predictors of abdominal aortic aneurysm growth or rupture: a systematic review. Eur J Vasc Endovasc Surg. 2016;52:475–486. 14. Bappoo N, Syed MBJ, Khinsoe G, et al. Low shear stress at baseline predicts expansion and aneurysm-related events in patients with abdominal aortic aneurysm. Circ Cardiovasc Imaging. 2021;14:1112–1121. 15. Mitsouras D, Leach JR. Expanding the radiologist's arsenal against abdominal aortic aneurysms, a versatile adversary. Radiology. 2020;295:730–732. 16. Koullias G, Modak R, Tranquilli M, et al. Mechanical deterioration underlies malignant behavior of aneurysmal human ascending aorta. J Thorac Cardiovasc Surg. 2005;130:677–683. 17. Raaz U, Zöllner AM, Schellinger IN, et al. Segmental aortic stiffening contributes to experimental abdominal aortic aneurysm development. Circulation. 2015;131:1783–1795. 18. Li T, Liu X, Sun H, et al. Assessment of the global and regional circumferential strain of abdominal aortic aneurysm with different size by speckle-tracking echocardiography. J Ultrasound Med. 2021;40:2619–2627. 19. Ning H, Liu X, Ma C, et al. The evaluation of longitudinal strain of large and small abdominal aortic aneurysm by two-dimensional speckle-tracking ultrasound. J Ultrasound Med. 2022;41:1085–1093. 20. Derwich W, Keller T, Filmann N, et al. Changes in aortic diameter and wall strain i
留言 (0)