
記住我








In patients with prostate cancer with intermediate- or high-risk disease, lymph node (LN) metastases often first occur in the pelvis or lower abdomen. Nodal staging is crucial in determining prognosis and treatment options.1 Although extended pelvic LN dissection (ePLND) is the criterion standard for assessing nodal status, prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography PET/CT is increasingly used as a noninvasive imaging modality to identify and localize metastatic sites before ePLND.2 Recent data, however, show limited sensitivity of PSMA-PET/CT with histopathology as the reference standard. Especially LNs smaller than 5 mm are easily missed on PSMA-PET/CT.3–8
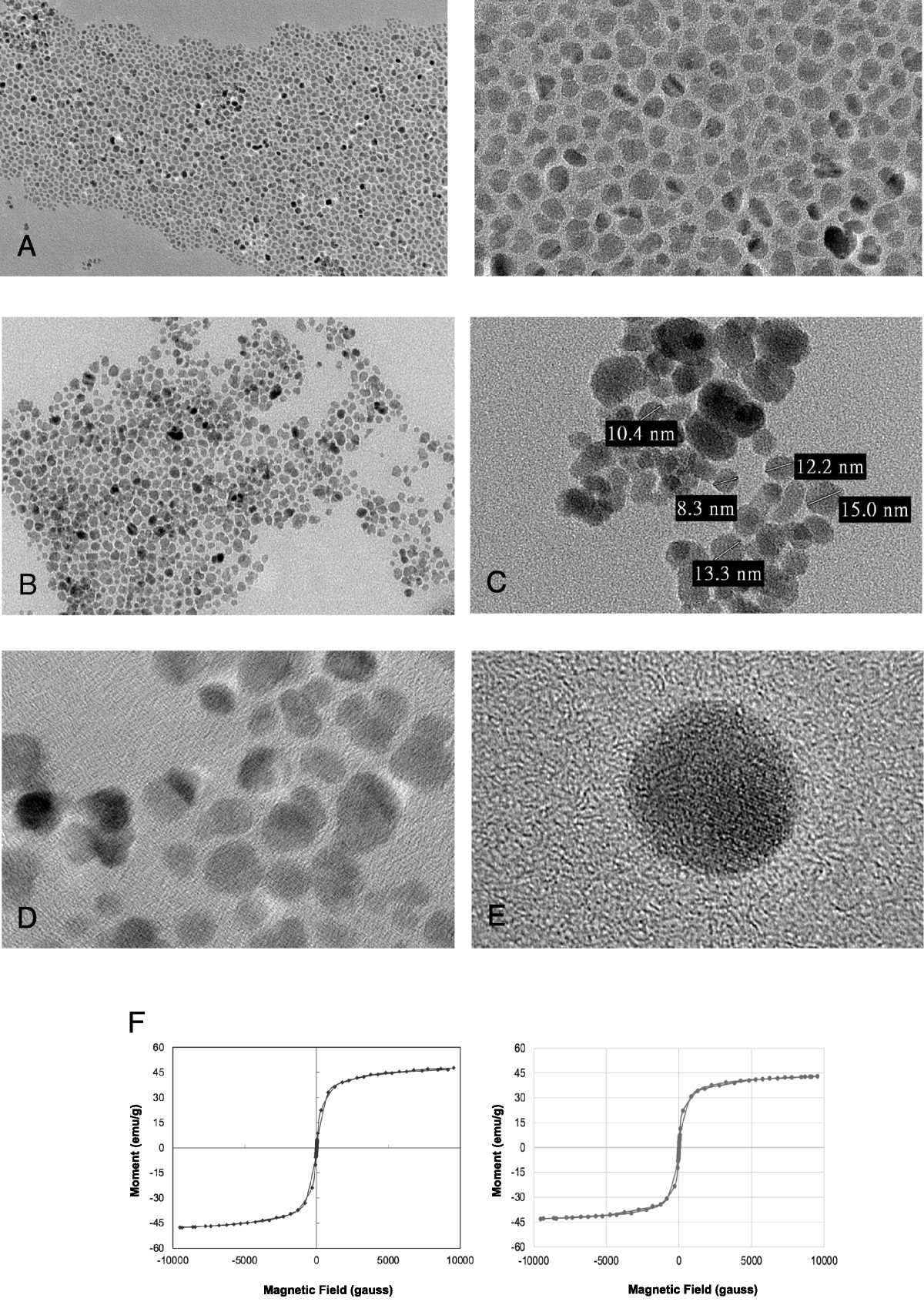
Another imaging modality to assess LN involvement is magnetic resonance imaging (MRI) enhanced with ultrasmall superparamagnetic iron oxide (USPIO) particles.9–11 This technique uses dextran-coated iron oxide nanoparticles (ferumoxtran-10), which are administered intravenously and accumulate only in healthy lymphatic tissue over 24–36 hours through phagocytosis by macrophages.12,13 Sensitive for the presence of these accumulated nanoparticles, USPIO-enhanced MRI can discriminate between healthy LNs and LNs that are (partially) infiltrated by metastatic tumor cells.14,15 Routine 3-dimensional (3D) T2*-weighted sequences with submillimeter isotropic resolution can visualize LNs as small as 2 mm.16
The targets on which imagings with PSMA-PET/CT and USPIO-MRI are based are very different; PSMA-PET targets PSMA expression on tumor tissue, whereas USPIO-MRI is a more anatomical imaging modality, depending on signal retention in tumor tissue as nanoparticles cause signal loss in healthy lymphatic tissue. Consequently, findings of the 2 imaging techniques may be complementary. A study comparing PSMA-PET/CT and USPIO-MRI in prostate cancer patients found that each modality identified potential LN metastases missed by the other. In particular, USPIO-MRI was superior at identifying suspicious LNs smaller than 5 mm.17 Unfortunately, an indisputable node-to-node comparison between in vivo imaging results and histopathology is hard to achieve, hampering the understanding of the identified differences. Because ePLND usually harvests more than 20 individual LNs, preparing the nodal material for histopathological examination by (1) finding all LNs within the resected adipose tissue specimens and (2) slicing all LNs into 3-mm-thick slices is very laborious and usually impossible to perform due to the high workload. As a result, small metastases are being missed.18 Using imaging as a guide to perform targeted sectioning of resection material could increase the detection rate and sensitivity of histopathology.
Furthermore, to comprehensively interpret the differences and agreements between the images from both modalities, a subnodal comparison is needed. With this aim, we conducted an explorative study comparing ex vivo 111In-PSMA μSPECT images with high-resolution 7 T USPIO μMR images and histopathology of a selection of resected LN specimens from prostate cancer patients, allowing to assess the degree of correspondence.
MATERIALS AND METHODS Patient PopulationThe study population comprises patients from the Dutch DETECT trial (NCT4300673). Twenty men with histologically proven prostate cancer were included between September 2020 and April 2022. The study was approved by the local medical ethical review board (CMO Arnhem-Nijmegen), and written informed consent was obtained from all patients before enrolment. All patients had newly diagnosed prostate cancer and ≥1 PSMA-PET suspicious LN on preoperative PSMA-PET/CT.
Administration of Contrast AgentsTwo days before surgery, patients received 2.6 mg/kg ferumoxtran-10 (Ferrotran; SPL Medical BV, Nijmegen, the Netherlands), through a slow intravenous drip infusion. The USPIO contrast agent ferumoxtran-10 (Ferrotran; SPL Medical BV, Nijmegen, the Netherlands) was used. This agent is available for clinical studies and in Named Patient Use Programs in the Netherlands and Switzerland. A large phase III international multicenter pivotal trial for European Medicines Agency approval is ongoing (EudraCT 2018-004310-18). The intravenous administration was performed over a period of 30–40 minutes and under medical supervision. One day before ePLND, patients received a mean single dose of 157 MBq (range, 151.8–164.2) 111In-PSMA-I&T injected as an intravenous bolus and were observed for 1 hour postadministration.
Surgical Procedure and Tissue PreparationExtended pelvic LN dissection was performed with radioguidance using a laparoscopic γ-probe (SOE-311-AL; Eurorad SA, Eckbolsheim, France) detecting radiation from 111In-PSMA-I&T. Both in vivo and ex vivo (back table) probe measurements were taken to identify LNs with increased activity. Lymph nodes with a maximum ex vivo count of ≥10 counts per second (cps) were considered probe suspicious. Those LNs were considered LNs of interest (LNOIs). In addition, large palpable LNs without increased activity were also considered LNOIs. All LNOIs were marked with sutures and subject to elaborate additional imaging. Resected tissue was collected separately according to the anatomical resection site and fixated in formalin. After surgery, the specimens containing LNOIs were prepared for ex vivo μSPECT and μMR imaging. Specimens were removed from formalin, and digital photographs were taken in the intended orientation of ex vivo imaging. Specimens were carefully packed in cellophane and fixated on an MR-compatible Perspex sheet with a 200-μL Eppendorf tube filled with a solution of 111In-PSMA-I&T as reference sample to match both MRI and SPECT images. Immediately after μSPECT and MRI acquisition, specimens were placed back in formalin to continue the fixation process.
Postoperative Ex Vivo μSPECT and MRI AcquisitionμSPECT acquisition was performed on a preclinical SPECT/CT system (U-SPECT II, MILabs) using a 1.0-mm diameter pinhole collimator tube. Acquisition time was 2 hours. MILabs reconstruction software was used to reconstruct the μSPECT scans via an ordered-subset expectation maximization algorithm (energy windows 145–188 keV and 220–270 keV, 1 iteration, 16 subsets, and voxel size of 0.75 mm). μMRI acquisition was performed on a preclinical 7 T MRI system interfaced with a clinical Siemens user interface (ClinScan; Bruker BioSpin, Ettlingen, Germany). An 86-mm body coil was used for signal excitation, whereas receiving the signal was done with a 20-mm diameter surface coil, covering the LNOIs. The ex vivo μMRI examinations consisted of a frequency-selective lipid excitation T1-weighted 3D gradient echo (GRE) sequence (TR = 15 milliseconds, TE = 2.8 milliseconds resolution = 110 × 110 × 110 μm, flip angle = 10 degrees) and a water-excited T1-weighted 3D multi-GRE pulse sequence with 5 acquired echoes (TR = 30 milliseconds, TE = 2.8, 7.1, 11.4, 15.7, and 20.0 milliseconds, resolution = 110 × 110 × 110 μm, flip angle = 14 degrees).
Histopathological EvaluationHistopathological evaluation was performed according to standard of care protocols with the addition of immunohistochemical PSMA staining. Lymph nodes of interest were separately numbered, sectioned, or sliced on different levels (5 mm), enclosed in tissue cassettes, and stained with hematoxylin-eosin and PSMA.
MR Image Evaluation and Coregistration With μSPECTTo provide iron-sensitive contrast for the interpretation of signal retention or attenuation within the lesions, T2*-fits of individual pixels of the multi-GRE images were used to calculate computed echo time (cTE) images19,20 of 15 milliseconds. Ex vivo images were evaluated by the coordinating physician. Lymph nodes of interest (marked with suture) were matched to LNs on ex vivo MRI based on comparison with macroscopic photographs. They were recognized on the basis of both 3D MR image sets as a spheroid bordered structure on water-selective images without signal intensity on lipid selective GRE images.
The retainment of high MR signal within an LN on the 15 milliseconds image, either partially or completely, was classified as suspicious for containing metastases.21,22 Overlay of μSPECT reconstructed images on MR images was performed manually using the software assistant SAFIR technology (Fraunhofer MEVIS, Bremen, Germany). The Eppendorf tube functioned as a 3-dimensional structure of reference for image coregistration.
Image Analysis and Comparison With HistopathologyTo substantiate the degree of correspondence between μSPECT and MR findings, a 4-level classification scheme was composed. This Likert scale is depicted in Figure 1 and describes the level of correspondence (LoC) with regard to the location and dimension of suspicious and nonsuspicious tumor tissue. The 4 categories range from poor correspondence (0%–25%; LoC 1), to moderate (25%–50%; LoC 2), to good (50%–75%; LoC 3), and excellent (75%–100%; LoC 4), with subcategories for appearance (a, b, c) (Fig. 1). Sizes of LNs were determined by measuring the longest axis in either 1 of 3 dimensions on lipid selective GRE images. The size of the suspicious part within an LN (high MR signal) was determined by measuring the longest axis in either 1 of 3 dimensions on the cTE 15 milliseconds water-excited GRE images. The assessment was performed by a trained researcher (M.S.) and an experienced radiologist (P.Z.). Any disagreement was resolved by discussion.
 FIGURE 1:
FIGURE 1: Four-point Likert scale for the level of correspondence between prostate-specific membrane antigen (PSMA) expression and ultrasmall superparamagnetic iron oxide (USPIO) particles in lymph nodes of interest (LNOIs). For PSMA μSPECT, the red color indicates the presence of PSMA-expressing tumor tissue. For USPIO μMRI, the black parts indicate loss of MR signal due to accumulation of USPIO contrast in the LNOI. The white parts indicate retaining of MR signal in tumor tissue.
Histopathological data from all LNOIs were collected. Node-to-node matching was achieved by manually matching macroscopically marked LNOI to nodes seen on ex vivo imaging and corresponding tissue cassette(s). Subnodal matching of histopathology and ex vivo imaging was difficult, so only histopathological presence or absence of metastatic tissue and PSMA expression was compared with imaging. All results are descriptive and depicted as numbers and percentages.
RESULTSTwenty newly diagnosed prostate cancer patients were included. Baseline characteristics of these patients are summarized in Table 1. The median interval between USPIO administration and ePLND was 46 hours (interquartile range [IQR], 46–51). The median time between 111In-PSMA-I&T administration and ex vivo μSPECT imaging was 28 hours (IQR, 26–31). No adverse events occurred during the administration of ferumoxtran-10 or 111In-PSMA-I&T.
TABLE 1 - Patient Characteristics and Imaging Characteristics Age at time of surgery (mean, range), y 69 (57–79) iPSA (mean, range), ng/L 22.2 (2.9–117) EAU risk classification (n, %) Intermediate risk 7 (35%) High risk 13 (65%) Time between USPIO particles administration and resection (median, IQR), h 46 (46–51) Time between 111In-PSMA-I&T administration and SPECT imaging (median, IQR), h 28 (26–31) LNOIs 41 γ-Probe suspicious 31 (74%) Maximum cps (median, IQR) 58 (18–116) Large lymph node, γ-probe nonsuspicious 10 (24%) Maximum cps (median, IQR) 4 (3–8)EAU, European Association of Urology; iPSA, initial prostate-specific antigen level; IQR, interquartile range; PSMA, prostate-specific membrane antigen; USPIO, ultrasmall superparamagnetic iron oxide; LNOI, lymph node of interest.
A total of 40 LNOI-containing tissue samples were scanned ex vivo. Three tissue samples were excluded from analysis due to insufficient imaging quality (n = 2) or inability to reliably coregister MR with μSPECT images (n = 1). The remaining 37 tissue samples contained 41 LNOIs. Of the 41 LNOIs, 31 lesions were suspicious based on increased maximum cps (median, 58; IQR, 18–116). The remaining LNOIs (n = 10) were found by palpation but not suspicious based on γ-probe measurements (median, 4 maximum cps; IQR, 3–8).
Evaluation of Ex Vivo μSPECT and USPIO-MRIBased on suture localization, all 41 selected LNOIs could be successfully matched to an LN on ex vivo μMRI. The median size of these LNs was 18 mm (range, 5–55 mm). Of the 31 probe-suspicious LNOI, 27 (87%) showed increased activity at the site of the suture on μSPECT image analysis (Fig. 2). In the same 27 LNOIs, the evaluation of water-selective images (cTE = 15 milliseconds) showed a high MR signal intensity in (parts of) the LNs compared with lipid tissue, making them suspicious of metastatic deposits. The median size of these deposits was 7 mm (range, 2–20). Histopathological evaluation confirmed the presence of PSMA-positive metastases in all 27 LNOIs (100%). Four LNOIs that were detected with the γ-probe did not indicate the presence of PSMA-avid metastases on μSPECT and on μMRI. Histopathological analysis of those lesions revealed no metastases.
 FIGURE 2:
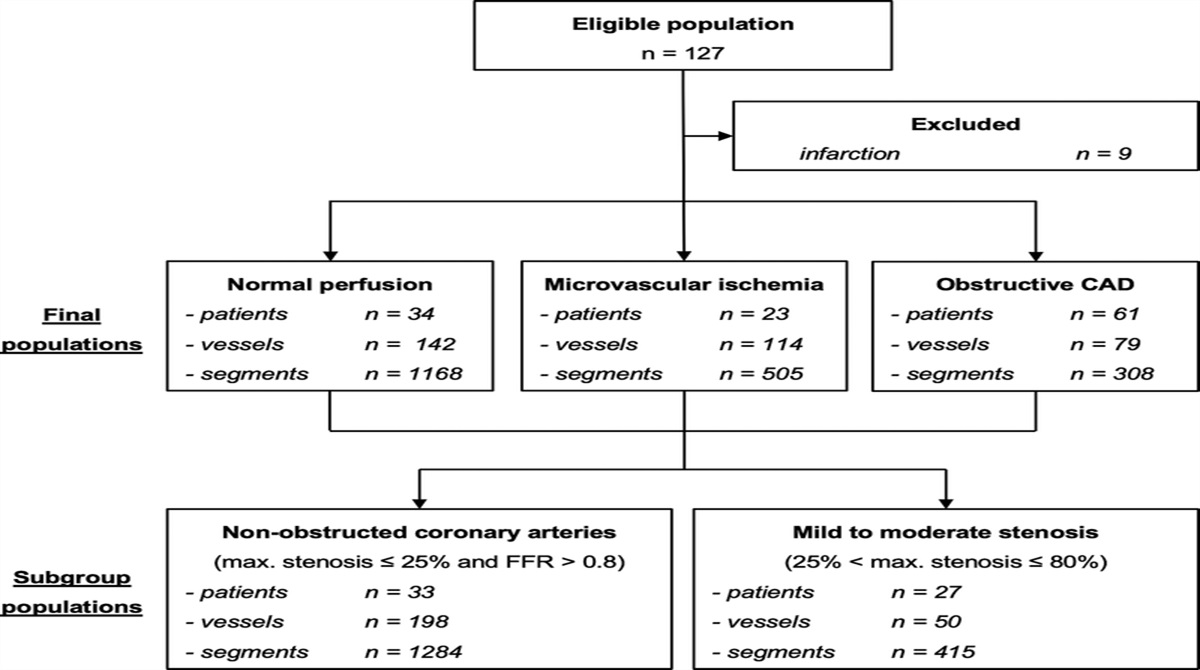
FIGURE 2: Overview of all LNOIs. The flowchart demonstrates the numbers and percentages of LNOIs with respect to imaging results and histopathology on a single-node level.
None of the 10 large palpable, probe-negative LNOIs showed increased activity on μSPECT image analysis or suspicion on USPIO-μMRI. However, in 1 of the 10 large palpable LNOIs that were not suspicious on γ-probe measurements, histopathology revealed a PSMA-avid metastasis of 3 mm in a 42-mm LNs, which was neither identified with μSPECT imaging nor on μMRI, also not in retrospect.
Correspondence Between μSPECT and USPIO-MRICoregistration of μSPECT images with USPIO-enhanced water-selective multi-GRE images was successful for 41 LNOIs. Classification of LoC and characteristics of all LNOIs are shown in Table 2. The majority of lesions had an LoC 4 (37/41, 90%). Figure 3 shows an example of a partially affected metastatic LNOI (as based on ex vivo μMRI) with high correspondence of the SPECT signal in 3 dimensions (LoC 4b). In 5 of 41 LNOIs, coregistered images of USPIO-enhanced MRI and μSPECT showed suspicion of completely affected metastatic LNs, with no remaining healthy nodal tissue (LoC 4c) and median 90 maximum cps max (range, 59–599). An example of an LNOI with LoC 4c is displayed in Figure 4A. All LNOIs with LoC 4b and 4c were suspicious based on peroperative γ-probe measurements, and all contained PSMA-expressing metastases on final histopathology. A total of 14 LNOIs (35%) showed no suspicion of metastases on either μSPECT or ex vivo μMR imaging and were thus classified LoC 4a with a median maximum cps of 6 (range, 0–15 cps). The majority (10/14) of those LNs were marked based on palpable size. The remaining marked LNs (4/14) measured a maximum cps of 13, 13, 14, and 15 cps, respectively, and contained no metastases on histopathology.
 TABLE 2:
TABLE 2: Characteristics of Lymph Nodes of Interest According to Level of Correspondence*
 FIGURE 3:
FIGURE 3: Multiplanar reconstruction of an LNOI with excellent correspondence between PSMA expression and absence of USPIO particles. An LNOI depicted in 3 orthogonal orientations (pink [A, B, C], blue [D, E, F], and yellow [G, H, I]); one orientation per row in correspondence to the color-axes depicted in A, D, and G. The first column (A, D, and G) shows the lipid selective gradient echo (GRE) MR images (anatomic) where the border of the LNOI is indicated with the green dotted line. The second column (B, E, and H) shows the water-excited GRE MR images at a computed echo time of 15 milliseconds (iron sensitive). The third column (C, F, and I) shows the 15 milliseconds water-excited GRE images coregistered with PSMA μSPECT images. The round structure visible on the right corner of the last row is the Eppendorf tube for reference.
 FIGURE 4: Typical examples of 3 individual LNOIs with different levels of correspondence, according to the 4-point Likert scale as described in Figure 1. Three examples of LNOIs with excellent (A), good (B), and moderate (C) correspondence between USPIO particle enhanced μMR and PSMA μSPECT. Left column shows the lipid selective GRE MR images (anatomic) where the border of the LNOI is indicated with the green dotted lines. The second column shows the water-excited GRE MR images at a computed echo time of 15 milliseconds (iron-sensitive). The third column shows the 15 milliseconds water-excited GRE images coregistered with PSMA μSPECT images. The fourth column shows 2 exemplary microscopic PSMA-stained slides of the LNOI. The LNOI in example A was classified as level of correspondence (LoC) 4c, example B as LoC 3a, and example C as LoC 2b in accordance to the description in Figure 1. Of note, without proper alignment during workup, the orientation of histopathological slides was only visually matched to the imaging modalities.
FIGURE 4: Typical examples of 3 individual LNOIs with different levels of correspondence, according to the 4-point Likert scale as described in Figure 1. Three examples of LNOIs with excellent (A), good (B), and moderate (C) correspondence between USPIO particle enhanced μMR and PSMA μSPECT. Left column shows the lipid selective GRE MR images (anatomic) where the border of the LNOI is indicated with the green dotted lines. The second column shows the water-excited GRE MR images at a computed echo time of 15 milliseconds (iron-sensitive). The third column shows the 15 milliseconds water-excited GRE images coregistered with PSMA μSPECT images. The fourth column shows 2 exemplary microscopic PSMA-stained slides of the LNOI. The LNOI in example A was classified as level of correspondence (LoC) 4c, example B as LoC 3a, and example C as LoC 2b in accordance to the description in Figure 1. Of note, without proper alignment during workup, the orientation of histopathological slides was only visually matched to the imaging modalities.A total of 3 LNOIs were classified as LoC 3 (7%) and 1 LNOI as LoC 2 (2%). Examples of both LoC 3 and LoC 2 are depicted in Figures 4B and 4C, respectively. All LoC 2 and LoC 3 lesions contained PSMA-expressing metastases on final histopathology.
DISCUSSIONCurrently, there are 2 advanced noninvasive imaging techniques for LN staging of patients with prostate cancer: PSMA radionuclide imaging and USPIO-MRI, which outperform conventional imaging, that is, CT scanning or nonenhanced MRI.23,24 In this work, we evaluated the correspondence between these 2 modalities ex vivo on a subnodal level. It seemed to be technically feasible to perform high-quality, high-resolution imaging of resected LNs by both techniques. This allows to identify and relate LN anatomy and metastases on imaging with histopathology.
First, an important finding of this study is that both PSMA μSPECT and USPIO μMRI findings on a single-node level strongly correspond regarding the presence or absence of metastatic tissue on final histopathology. Only a 3-mm small partial metastasis was missed by both PSMA-μSPECT and μMRI.
Second, on subnodal level, meticulous coregistration of the μSPECT and μMR images demonstrated excellent correspondence regarding the presence of metastatic tissue and affected subnodal site in 90% (37/41) of the LNOI. Furthermore, both modalities strongly agreed in identifying both partially (LoC 4b) and completely (LoC 4c) affected LNs. We identified only 1 lesion with moderate (LoC 2) and no lesions with poor (LoC 1) correspondence. These findings not only verify concordance but also give insight in the subnodal appearance of both imaging technologies. As considerable uncertainties remain regarding the exact (patho)physiological mechanism of both USPIO contrast and PSMA tracers, exact explanations for the identified differences in LoC 2 and 3 lesions remain unknown.25 Although it is widely accepted that the lack of (or little) USPIO presence in metastatic LNs is due to the absence of USPIO-accumulating macrophages, the actual evidence regarding this hypothesis is limited.12,13 It still remains unclear which macrophage types accumulate USPIO. Meanwhile, the presence of partly non–PSMA-expressing tumor tissue (or other tissue, eg, fibrosis) might explain discrepancies.14
Nonetheless, our findings support the findings of Schilham et al, who found that the majority (73%) of PSMA-PET/CT suspicious LNs were also suspicious on USPIO-MRI.14 Interestingly, in their study, only 33% of the USPIO-MRI suspicious LNs were PSMA-PET positive. The small size of these LNs and the limitation of the spatial resolution of PET/CT are likely to contribute to this discrepancy, as LN metastases smaller than 5 mm are difficult to detect on PET/CT.26 This is also why true PET-positive nodal metastases (median, 4.0–13.6 mm) are on average larger than false PET-negative metastases (median, 2.5–5.0 mm).27 The detection limit of USPIO-MRI is determined by the spatial resolution of the 3-dimensional MRI, which is 0.8-mm isotropic, resulting in the detection of many small suspicious nodes with short-axis diameter <3 mm LNs. For these small LNs, histopathological evaluation is difficult and time-consuming.28 In this work, we focused on a selection of LNs based on peroperative γ-probe measurements of excised tissue (31/41) and morphologically large LNs (10/41). Therefore, there was high a priori likelihood of an LN being positive on PSMA μSPECT and thus a selection bias in favor of SPECT-suspicious lesions. Second, although based on the same concept of PSMA expression, ex vivo γ-probe measurements are potentially more sensitive compared with in vivo PSMA-PET/CT, considering the smaller distance between the PSMA-expressing tissue and the γ-detector and the lack of background activity.
The concept of ex vivo imaging can support pathological evaluation of removed LNs, as determining the presence or absence of metastases in LN dissection specimens is a labor-intensive task. Extensive sectioning of the sample leads to far too much evaluation of the resected material, leading to the possible missing of small metastases and high costs. Ex vivo imaging results can provide quick and accurate information about the possible presence, amount, and location of suspicious lesions.29 The use of these images when cutting specimens can prevent small LNs and (micro)metastases within LNs.18
This explorative study is not without limitations. Most importantly, due to its PSMA-PET–driven design, it comprises a selected subset of only PSMA γ-probe positive or large palpable LNs. This impedes a conclusion regarding the particularly interesting subgroup of small LNs that are missed in PSMA scanning and positive in USPIO-MRI. Second, although all lesions could be matched to histopathology on a node-to-node level, an exact subnodal anatomical comparison with histopathology was not possible. To better understand how both imaging modalities relate to pathophysiological processes in LNs, a systematic and meticulous correlation between imaging and pathology in larger series of LNs is needed.22 In such research, small LNs that are suspicious on in vivo USPIO-MRI and undetectable on PSMA-PET/CT are of particular interest. Third, our LoC classification is only semiquantitative, as SPECT imaging does not allow exact quantification of area of enhancement to compare to signal-enhanced area or volume on MRI. However, our 4-point Likert scale did allow a subnodal comparison between the imaging modalities.
In conclusion, this explorative, proof-of-concept study examined the correspondence between 2 advanced imaging modalities for nodal staging of prostate cancer on a subnodal level. Coregistration of both imaging modalities seems to be technically feasible, and both modalities showed excellent subnodal correspondence in the majority of lesions, in line with clinical histopathological readouts.
REFERENCES 1. Marra G, Valerio M, Heidegger I, et al. Management of patients with node-positive prostate cancer at radical prostatectomy and pelvic lymph node dissection: a systematic review. Eur Urol Oncol. 2020;3:565–581. 2. Bukavina L, Luckenbaugh AN, Hofman MS, et al. Incorporating prostate-specific membrane antigen positron emission tomography in management decisions for men with newly diagnosed or biochemically recurrent prostate cancer. Eur Urol. 2022;83:521–533. 3. Baas DJH, Schilham M, Hermsen R, et al. Preoperative PSMA-PET/CT as a predictor of biochemical persistence and early recurrence following radical prostatectomy with lymph node dissection. Prostate Cancer Prostatic Dis. 2022;25:65–70. 4. Stabile A, Pellegrino A, Mazzone E, et al. Can negative prostate-specific membrane antigen positron emission tomography/computed tomography avoid the need for pelvic lymph node dissection in newly diagnosed prostate cancer patients? A systematic review and meta-analysis with backup histology as reference standard. Eur Urol Oncol. 2022;5:1–17. 5. Hermsen R, Wedick EBC, Vinken MJM, et al. Lymph node staging with fluorine-18 prostate specific membrane antigen 1007-positron emission tomography/computed tomography in newly diagnosed intermediate- to high-risk prostate cancer using histopathological evaluation of extended pelvic node dissection as reference. Eur J Nucl Med Mol Imaging. 2022;49:3929–3937. 6. van Kalmthout LWM, van Melick HHE, Lavalaye J, et al. Prospective validation of gallium-68 prostate specific membrane antigen-positron emission tomography/computerized tomography for primary staging of prostate cancer. J Urol. 2020;203:537–545. 7. Jansen BHE, Bodar YJL, Zwezerijnen GJC, et al. Pelvic lymph-node staging with (18)F-DCFPyL PET/CT prior to extended pelvic lymph-node dissection in primary prostate cancer—the SALT trial. Eur J Nucl Med Mol Imaging. 2021;48:509–520. 8. Klingenberg S, Jochumsen MR, Ulhøi BP, et al. 68Ga-PSMA PET/CT for primary lymph node and distant metastasis NM staging of high-risk prostate cancer. J Nucl Med. 2021;62:214. 9. Dadfar SM, Roemhild K, Drude NI, et al. Iron oxide nanoparticles: diagnostic, therapeutic and theranostic applications. Adv Drug Deliv Rev. 2019;138:302–325. 10. Turkbey B, Czarniecki M, Shih JH, et al. Ferumoxytol-enhanced MR lymphography for detection of metastatic lymph nodes in genitourinary malignancies: a prospective study. AJR Am J Roentgenol. 2020;214:105–113. 11. Czarniecki M, Pesapane F, Wood BJ, et al. Ultra-small superparamagnetic iron oxide contrast agents for lymph node staging of high-risk prostate cancer. Transl Androl Urol. 2018;7(Suppl 4):S453–s61. 12. Koh DM, Brown G, Temple L, et al. Rectal cancer: mesorectal lymph nodes at MR imaging with USPIO versus histopathologic findings—initial observations. Radiology. 2004;231:91–99. 13. Xue HD, Lei J, Li Z, et al. Lymph node image with ultrasmall superparamagnetic iron oxide and comparison with pathological result [in Chinese]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2009;31:139–145. 14. Froehlich JM, Triantafyllou M, Fleischmann A, et al. Does quantification of USPIO uptake-related signal loss allow differentiation of benign and malignant normal-sized pelvic lymph nodes? Contrast Media Mol Imaging. 2012;7:346–355. 15. Birkhauser FD, Studer UE, Froehlich JM, et al. Combined ultrasmall superparamagnetic particles of iron oxide-enhanced and diffusion-weighted magnetic resonance imaging facilitates detection of metastases in normal-sized pelvic lymph nodes of patients with bladder and prostate cancer. Eur Urol. 2013;64:953–960. 16. Heesakkers RA, Fütterer JJ, Hövels AM, et al. Prostate cancer evaluated with ferumoxtran-10-enhanced T2*-weighted MR imaging at 1.5 and 3.0 T: early experience. Radiology. 2006;239:481–487. 17. Schilham MGM, Zamecnik P, Privé BM, et al. Head-to-head comparison of (68)Ga-prostate-specific membrane antigen PET/CT and ferumoxtran-10-enhanced MRI for the diagnosis of lymph node metastases in prostate cancer patients. J Nucl Med. 2021;62:1258–1263. 18. Schilham MGM, Küsters-Vandevelde H, Somford DM, et al. How image-guided pathology can improve the detection of lymph node metastases in prostate cancer. Clin Nucl Med. 2022;47:559–561. 19. Philips BWJ, Stijns RCH, Rietsch SHG, et al. USPIO-enhanced MRI of pelvic lymph nodes at 7-T: preliminary experience. Eur Radiol. 2019;29:6529–6538. 20. Philips BWJ, Fortuin AS, Orzada S, et al. High resolution MR imaging of pelvic lymph nodes at 7 tesla. Magn Reson Med. 2017;78:1020–1028. 21. Harisinghani MG, Barentsz J, Hahn PF, et al. Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med. 2003;348:2491–2499. 22. Driessen DAJJ, Zámecnik P, Dijkema T, et al. High-accuracy nodal staging of head and neck cancer with USPIO-enhanced MRI: a new reading algorithm based on node-to-node matched histopathology. Invest Radiol. 2022;57:810–818. 23. Hofman MS, Lawrentschuk N, Francis RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet. 2020;395:1208–1216. 24. Heesakkers RA, Hovels AM, Jager GJ, et al. MRI with a lymph-node-specific contrast agent as an alternative to CT scan and lymph-node dissection in patients with prostate cancer: a prospective multicohort study. Lancet Oncol. 2008;9:850–856. 25. Shetty D, Patel D, Le K, et al. Pitfalls in gallium-68 PSMA PET/CT interpretation—a pictorial review. Tomography. 2018;4:182–193. 26. Wang K. Feasibility of high spatial resolution working modes for clinical PET scanner. Int J Med Phys Clin Eng Radiat Oncol. 2018;7:539–552. 27. Hernes E, Revheim ME, Hole KH, et al. Prostate-specific membrane antigen PET for assessment of primary and recurrent prostate cancer with histopathology as reference standard: a systematic review and meta-analysis. PET Clin. 2021;16:147–165. 28. Fortuin A, van Asten J, Veltien A, et al. Small suspicious lymph nodes detected on ultrahigh-field magnetic resonance imaging (MRI) in patients with prostate cancer with high risk of nodal metastases: the first in-patient study on ultrasmall superparamagnetic iron oxide–enhanced 7T MRI. Eur Urol. 2023;83:375–377. 29. Stijns R, Philips B, Wauters C, et al. Can ex vivo magnetic resonance imaging of rectal cancer specimens improve the mesorectal lymph node yield for pathological examination? Invest Radiol. 2019;54:645–652.
留言 (0)