
記住我
Hepatic hemangioma (HH) is the most common benign liver tumor in adults, with an incidence ranging from 0.4 to 20% [1]. Although the incidence of HH can be as high as 20%, they are considered benign lesions with minimal malignant potential [2]. Furthermore, most HH are asymptomatic and are typically discovered incidentally during routine medical examinations [3]. Therefore, the decision to treat HH depends on factors such as their size, growth rate, location, and the psychological impact on the patient [4,5]. In accordance with the consensus of domestic experts [4], our center classified HH into 3 grades according to the tumor length diameter: small hemangioma (<5 cm), large hemangioma (LHH) (5.0–9.9 cm) and giant hemangioma (GHH) (≥10.0 cm) [6]. In contrast, non-domestic scholars classify tumors with a diameter of >4 cm as GHH [2,7], and some foreign scholars have suggested that it is more reasonable to call HH with a diameter of ≥10 cm as GHH [8]. Currently, HH resection remains the reliable method for treating HH [9–11]. Consequently, most research on HH treatment has focused on comparing the efficacy of resection vs. thermal ablation [12,13] and resection vs. interventional embolization (IE) [14,15]. There is a lack of comparative studies between thermal ablation and IE. Thermal ablation techniques used in HH treatment include radiofrequency ablation (RFA) and microwave ablation (MWA). While RFA and MWA share similar principles, they differ in terms of ablation efficiency. RFA has a lower ablation efficiency and longer procedure times but offers precise control over the ablation zone, making it suitable for smaller hemangiomas located near important structures such as the hepatic portal vein. On the other hand, MWA provides rapid heating, a larger ablation zone, and shorter procedure times making it more suitable for GHH. Studies, such as those conducted by Wu et al. [16], suggest that RFA is not suitable for treating GHH due to a high rate of complications, even though no mortality cases were reported. Additionally, research by Kong et al. [17] identified thermal ablation method, HH diameter, and ablation time as independent risk factors associated with hemoglobinuria. Therefore, RFA is used in our center to treat patients with LHH who have a need for thermal ablation. For IE in HH treatment, drugs can be categorized into iodized oil (Lipiodol)-based strategies like L+Bleomycin (BLE), L+Pingyangmycin (PYG), or L+Ethanol, as well as non-iodized oil strategies like polyvinyl alcohol (PVA). Some studies [18,19] have shown that IE using L+BLE, L+PYG, or L+ethanol is safe and effective, while PVA-based transcatheter arterial embolization (TAE) has shown limited effectiveness in reducing hemangioma size. Long-term follow-up studies, such as those by Liu et al. [20], found that the long-term effective rates of TAE for LHH and GHH were 45.9% and 12.5%, respectively. At our center, that is, based on the L+BE strategy is referred to as transcatheter arterial chemoembolization (TACE) and is used to treat patients with LHH. This study aims to provide a comprehensive comparison of the treatment outcomes of RFA and TACE, exploring their respective advantages and disadvantages. The results of this research are expected to offer valuable insights and guidance for clinical practitioners in selecting appropriate treatment approaches based on individual patient conditions, thus holding significant clinical significance in the management of LHH.
Information and methods Study participantsThis is a single-center retrospective study. After obtaining approval from the medical ethics committee, medical records of patients who underwent RFA and TACE for LHH at Chaoyang Central Hospital between September 2018 and February 2023 were retrieved. Following inclusion and exclusion criteria screening and obtaining informed consent from patients and their families, a total of 82 patients with LHH were included in this study. Among them, 39 patients received RFA treatment, and 43 patients received TACE treatment.
Inclusion criteria for patients undergoing RFA or TACE treatment for LHH Patients diagnosed with LHH. Patients who chose RFA or TACE as the surgical method. Patients who underwent regular follow-up examinations using color ultrasound, contrast-enhanced CT or contrast-enhanced MRI after RFA or TACE procedures. Exclusion criteria Patients who had received previous treatment for HH before the study. Patients with infectious diseases. Patients with concomitant other types of liver tumor diseases such as hepatocellular carcinoma. Preoperative preparationHH was diagnosed by enhanced CT or enhanced MRI in both the RFA and TACE groups before surgery and was used to assess the size, location and number of hemangiomas. All patients underwent routine preoperative laboratory tests such as routine blood test, routine urine test, renal function test, liver function, coagulation function, etc. A preoperative antibiotic skin test was completed. The risks of surgery and anesthesia were explained to the patients and their families, and the informed consent for surgery was signed by the patients and their families.
Methods of treatmentWhen patients visit, outpatient doctors provide them with objective information about these two treatment methods, including their advantages, disadvantages, risks, and expected outcomes. After fully understanding, patients decide on their own which method of treatment to adopt. Due to the distinct professional domains involved in RFA and TACE, surgeries are respectively performed by physicians with the title of chief physician in the departments of hepatobiliary surgery and interventional medicine. The operator for each group remains the same.
Radiofrequency ablation Anesthesia methodGeneral anesthesia was administered.
RFA approachThe choice of ablative equipment involves the use of a straight-needle design with a cold-circulation RFA electrode. In our center, the RFA electrodes selected are the Cool-tip cluster RF needles (15–2.5 cm) from COVIDIEN. The ablation process utilizes a single electrode. The patient is placed in a supine position under anesthesia with a laryngeal mask or endotracheal tube to control breathing. Negative electrode pads are attached to the mid-thigh on both sides. The puncture area is routinely disinfected, and draping is performed. The HH location and the skin entry point and angle for the RFA needle are determined through CT scanning. Under CT guidance and monitoring, the RFA needle is advanced through the abdominal wall and normal liver tissue to reach the edge of the HH. Ablation strategy considerations include [4,5] (1) the ablation electrode should traverse at least 1 cm of normal liver tissue into the HH, with the first ablation point selected at the tumor’s edge. Adequate ablation time at the initial point is extended to prevent bleeding at the puncture site and avoid complications such as tumor rupture and significant bleeding during ablation. (2) Adopt a multi-point ablation strategy of ‘first edge, then center’, with the second needle insertion point chosen at the edge of the first ablation focus. (3) Prioritize ablation of tumor tissue near feeding arteries to block the blood supply to the HH, enhancing ablation efficiency and reducing related complications. (4) Ensure the needle tip reaches the opposite edge of the tumor without protruding. (5) Monitor the ablation endpoint primarily through intraoperative CT imaging, power values on the RFA device, and ablation time. Complete ablation is indicated by tumor shrinkage and appearing as a low-density lesion on CT. Ablation time at each puncture point is restricted to approximately 12 min, with the total ablation time for all points kept within 1.5 h.
Transcatheter arterial chemoembolization Anesthesia methodLocal anesthesia was administered.
TACE approachThe patient lies supine on the digital subtraction angiography (DSA) procedure table. Intravenous infusion of 500 ml of 0.9% sodium chloride solution is administered at a drip rate of 40 drops per minute. Local infiltration anesthesia is performed in the right groin area using 5 ml of 2% lidocaine after the intravenous fluid is initiated and effective. Subsequently, a right femoral artery puncture is carried out, and a 5F catheter sheath, guide wire, and catheter are placed. Due to the early opacification and slow emptying of the contrast agent within the HH, the ‘staining’ duration of the HH is prolonged, exhibiting the characteristic of ‘early filling and late emptying’. In the arterial phase, multiple blood sinuses or larger supplying arteries are visible, presenting as varying-sized ‘small cotton balls’, ‘popcorn’ or ‘fruits hanging from a tree’ signs. After confirming the HH through iodophor contrast imaging, a microcatheter is introduced with the assistance of a Yashiro catheter, allowing for super-selective placement into the feeding artery of the HH. The embolic agent is a mixture of 10 ml of iodized oil and 30 000 to 45 000 units of bleomycin. The specific dosage is determined based on the intraoperative size of the tumor and the embolization endpoint, with bleomycin not exceeding 45 000 units [21]. If the tumor is too large and not completely filled, an additional 10 ml of iodized oil can be mixed. The embolic agent is slowly injected into the feeding artery of the HH through the microcatheter. The embolization endpoint is reached when the embolic agent remains visible within the HH feeding artery after three respiratory cycles, indicating sufficient filling of the HH. After completing all procedures, a follow-up contrast imaging is performed, demonstrating proper deposition of iodized oil within the HH, indicating the completion of the surgery. Local pressure is applied to the puncture site in the groin area for 15 min, followed by local compression bandaging and the application of a saline bag for pressure, aiming to prevent the formation of a subcutaneous hematoma. Postoperatively, the patient is advised to maintain a supine position, with immobilization of the right lower limb for 6 h.
Data collectionWe collected the following information from both groups of patients: gender, age, how the HH was detected, location, size, and number of HH, preoperative and postoperative day 1 hemoglobin (HB), white blood cell (WBC) count, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine, total bilirubin (TBIL), surgical complications, application of postoperative pain medication, Operating-time, Postoperative-hospitalization, Hospitalization costs, and date of follow-up. The two groups of patients were followed up for a maximum of 41 months and a minimum of 6 months after surgery, and the corresponding examinations were done at 6–12 months after surgery to evaluate the treatment effect.
RFA group treatment efficacy analysisAt 6–12months postoperatively, treatment efficacy was assessed using contrast-enhanced CT or MRI scans, according to the following criteria: (The delayed phase for both contrast-enhanced CT and MRI is set to 5 min to ensure optimal contrast agent filling and imaging results. For contrast-enhanced CT, the NeuViz 128CT system from Neusoft Corporation is selected, and 80 ml of Ioversol contrast agent is administered. For contrast-enhanced MRI, the Signa Pioneer 3.0 system from GE Corporation is chosen, and 15 ml of gadoteric acid injection is used as the contrast agent.)
Complete response (CR): Complete disappearance of the lesion, meaning there was no enhancement observed in the target lesion on postoperative contrast-enhanced CT or MRI scans. Partial response (PR): Substantial reduction in the size of the lesion, with the product of the two largest dimensions of the enhancing portion being less than 30% of the product of the two largest dimensions of the lesion postoperatively. Minimum response: Partial reduction in the lesion, with the product of the two largest dimensions of the enhancing portion being between 30% and 50% of the product of the two largest dimensions of the lesion postoperatively. Stable disease: Minimal changes in the lesion, with the product of the two largest dimensions of the enhancing portion being more than 50% of the product of the two largest dimensions of the lesion postoperatively or with no significant changes observed in the lesion postoperatively. Progressive disease: Increase in the size of the lesion by more than 25%, along with a continuing growth trend, as observed on postoperative contrast-enhanced CT or MRI scans.(Note: If there are multiple enhanced regions, calculate the area of the enhanced portions by summing the product of the maximum diameters in each enhanced region.)
Effective rate = (CR + PR)/total number of patients in the RFA group × 100%
TACE group treatment efficacy analysisAt 6–12 months postoperatively, treatment efficacy was evaluated using contrast-enhanced CT or ultrasound (B-mode) scans, following the latest Response Evaluation Criteria in Solid Tumors [22] standards:
Complete response: Complete disappearance of the lesion, which is sustained for ≥4 weeks. Partial response: A reduction in the maximum diameter of the lesion by ≥30%, which is sustained for ≥4 weeks. Stable disease: A decrease in the maximum diameter of the lesion by <30% or an increase in diameter by ≤20%. Progressive disease: An increase in the maximum diameter of the lesion by >20%.Effective rate = (CR + PR)/total number of patients in the TACE group × 100%
Statistical methodsNormally distributed metric data was represented by the mean ± SD (X ± s) and analyzed using independent sample t-tests. Skewed metric data was represented by the median (P25, P75) and analyzed using non-parametric tests. Count data were expressed as frequencies (percentages) and analyzed using the chi-square test. All statistical analyses were performed using SPSS 25.0 statistical software. Statistical significance was defined as a P-value < 0.05.
Results Patient characteristicsA total of 82 patients meeting the inclusion criteria were included in the study. Among them, 39 were in the RFA group, and 43 were in the TACE group. Table 1 summarizes the characteristics of the patients. There were no significant differences between the two treatment groups in terms of patient gender, age, tumor number, tumor size, tumor location, reason for tumor discovery, blood routine, and liver and kidney function indicators. Therefore, the data for the two groups can be considered balanced and comparable (Table 1).
Table 1. - Baseline characteristics and tumor characteristics of patients RFA (n = 39) TACE (n = 43) P-value Age (years) 51.7 ± 9.4 51.2 ± 7.9 0.79 Gender Man 16 (41.0%) 10 (23.3%) 0.08 Woman 23 (59.0%) 33 (76.7%) Preoperative Hb (g/L) 139.9 ± 22.6 135.2 ± 12.9 0.30 WBC (×109/L) 5.8 (5.3, 7.0) 5.6 (5.1, 6.7) 0.32 ALT (U/L) 19.0 (13.0, 22.0) 18.0 (16.0, 21.0) 0.79 AST (U/L) 18.0 (15.0,21.0) 18.0 (16.0, 21.0) 0.69 Creatinine (mmol/L) 56.0 (50.2, 74.9) 59.0 (54.1, 69.5) 0.40 TBil (mmol/L) 10.8 (8.2, 14.3) 11.4 (9.3, 15.4) 0.34 Alb (g/L) 40.1 ± 3.2 40.5 ± 3.1 0.61 Preoperative diameter (cm) 6.6 ± 1.4 7.1 ± 1.3 0.08 Number of lesions One 25 (64.1%) 34 (79.1%) 0.13 Several (≥2) 14 (35.9%) 9 (20.9%) Lesion location Left lobe 13 (33.3%) 19 (44.2%) 0.06 Right lobe 18 (48.2%) 22 (51.2%) Left and right lobe 8 (20.5%) 1 (2.3%) liver caudate lobe 0 (0%) 1 (2.3%) Reasons for discovery Medical checkup 32 (82.1%) 34 (79.1%) 0.73 Symptomatic 7 (17.9%) 9 (20.9%)Primary lesions with a diameter of ≥5 cm will be included in the statistical analysis, while those with a diameter of <5 cm will undergo treatment during the procedure but will not be included in the statistical analysis.
The RFA group exhibited a significantly longer total operation time compared to the TACE group (100.8 ± 35.5 min vs. 41.2 ± 14.9 min, P < 0.001) (Table 2). Additionally, the RFA group incurred higher hospitalization costs than the TACE group (30952.1 ± 4327.6 CNY vs. 17 052.7 ± 1364.8 CNY, P < 0.001) (Table 2). On the first day postoperatively, the RFA group showed higher levels of WBC (P < 0.001), ALT (P < 0.001), AST (P < 0.001), and TBIL (P < 0.001) compared to the TACE group (Table 2). When compared to preoperative levels, WBC, ALT, AST, and TBIL in both groups increased on the first postoperative day, with the elevation range being greater in the RFA group than in the TACE group (Table 3). No statistically significant differences were observed in the remaining indicators (Tables 2 and 3).
Table 2. - Postoperative results of patients RFA TACE t/Z P-value Operating time (minutes) 100.8 ± 35.5 41.2 ± 14.9 8.7 <0.001 Postoperative-hospitalization (days) 2.0 (2.0–3.0) 2.0 (2.0–3.0) 1.3 0.19 Hospitalization costs (CNY) 30952.1 ± 4327.6 17 052.7 ± 1364.8 17.2 <0.001 First postoperative day Hb (g/L) 128.7 ± 22.1 126.1 ± 16.4 0.6 0.58 WBC (×109/L) 10.9 (9.3–14.8) 6.8 (5.8–8.2) 6.1 <0.001 ALT (U/L) 221.0 (142.0–505.0) 25.0 (20.0–80.0) 6.1 <0.001 AST (U/L) 291.0 (180.0–425.0) 29.0 (18.0–65.0) 6.5 <0.001 Creatinine (mmol/L) 60.0 (46.2–67.4) 61.0 (55.0–75.5) 1.6 0.12 TBil (mmol/L) 27.84 (23.6–35.62) 16.3 (12.8–21.8) 5.9 <0.001 Alb (g/L) 39.1 ± 3.7 39.4 ± 3.3 0.32 0.75As shown in Table 4, a total of 34 patients experienced 38 cases of general complications, including 17 out of 39 patients (43.6%) in the RFA group and 17 out of 43 patients (39.5%) in the TACE group, with no statistically significant difference (P = 0.7). Among the 39 patients in the RFA group, 15 (38.5%) experienced postoperative abdominal pain, while in the TACE group of 43 patients, 7 (16.3%) had postoperative abdominal pain. This difference in the occurrence of postoperative abdominal pain was statistically significant (P = 0.02), with a higher incidence in the RFA group. In the RFA group of 39 patients, 3 (7.7%) experienced postoperative belch, while in the TACE group of 43 patients, 11 (25.6%) had postoperative belch. This difference in the occurrence of postoperative belch was also statistically significant (P = 0.03), with a higher incidence in the TACE group. There were no statistically significant differences in other general complications (P > 0.05) (Table 4).
Table 4. - Comparison of general complications Dindo-Clavien RFA (39) TACE (43) P-value General complications 17 (43.6%) 17 (39.5%) 0.7 Abdominal paina I 15 (38.5%) 7 (16.3) 0.02 Belch I 3 (7.7%) 11 (25.6%) 0.03 Feverishb I 0 (0%) 1 (2.3%) >0.99 Cough I 1 (2.6%) 0 (0%) 0.96aWhether or not pain medication was applied.
bTemperature >38 °C.
As shown in Table 5, a total of 42 procedure-related complications occurred in 36 patients, including 23 cases (59.0%) in the RFA group and 13 cases (30.2%) in the TACE group (P = 0.009). Temporary liver injury was observed in 23 patients (59.0%) in the RFA group and 12 patients (27.9%) in the TACE group (P = 0.005). There were no statistically significant differences in other procedure-related complications (P > 0.05). According to the Dindo-Clavien classification [23], only 2 patients in the TACE group, who had ischemic cholecystitis, required the use of antibiotics and were classified as grade II complications. All other complications in these patients were either treated with grade I medication or resolved spontaneously (Table 5)
Table 5. - Comparison of procedure-related complications Dindo-Clavien RFA (39) TACE (43) P-value Procedure-related complications 23 (59.0%) 13 (30.2%) 0.009 Temporary liver injurya I 23 (59.0%) 12 (27.9%) 0.005 Hemolytic jaundiceb I 4 (10.3%) 0 (0%) 0.10d SIRSc I 3 (7.7%) 0 (0%) 0.20d Ischemic cholecystitis II 0 (0%) 2 (4.7%) 0.52daAlanine aminotransferase and/or aspartate aminotransferase >80 U/L.
bTotal bilirubin >34.2 µmol/L.
cDiagnostic criteria for Systemic Inflammatory Response Syndrome (SIRS) were defined as the presence of any two or more of the following indices: (1) temperature >38 °C; (2) heart rate >90 beats/min; (3) respiratory rate >20 breaths/min or partial pressure of carbon dioxide in the blood gas analysis <32 mmHg (1 mmHg = 0.133 kPa); 4), blood routine white blood cell count >12 × 109/L.
dFisher probabilities.
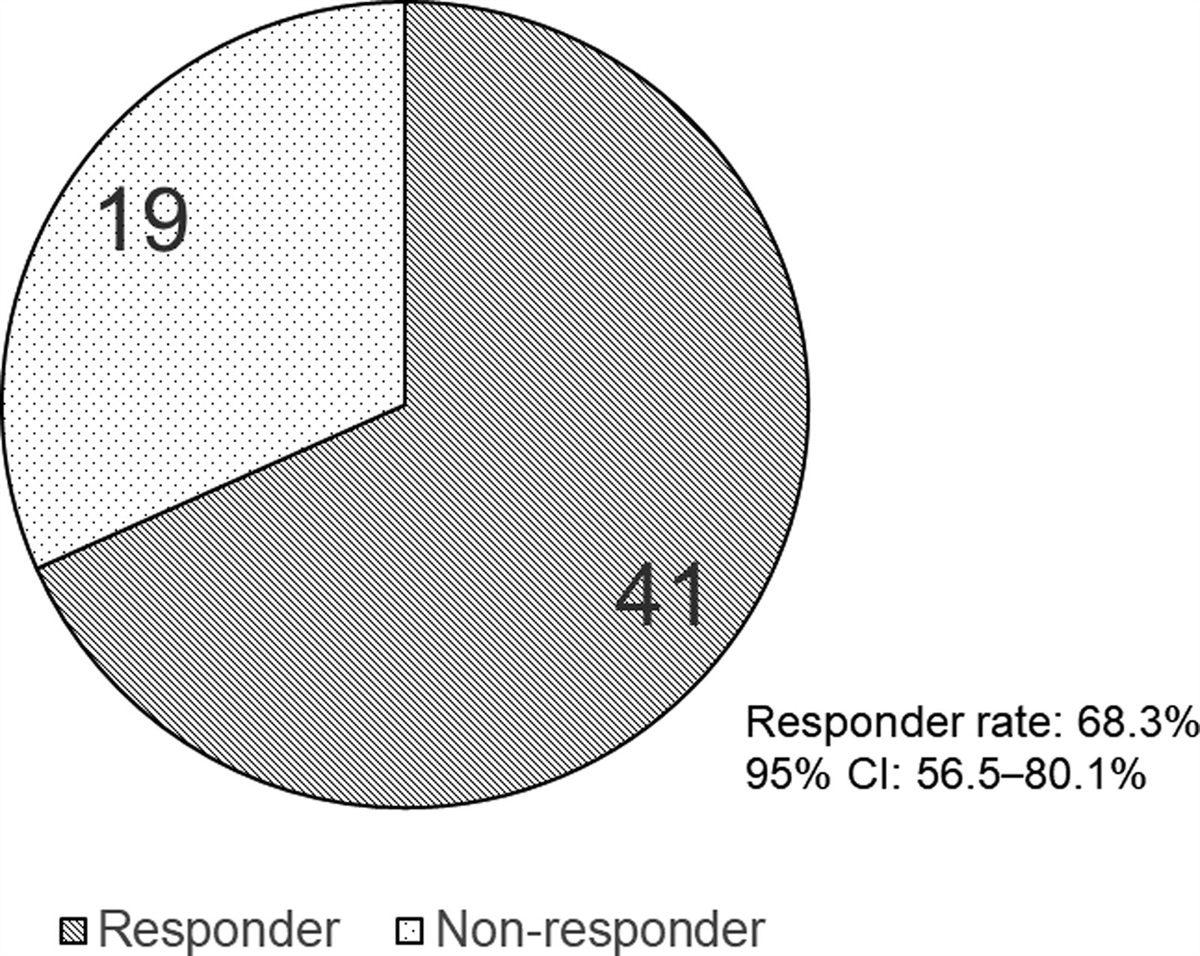
The postoperative 6–12-month radiological evaluation showed that in the RFA group, 32 out of 39 patients (82.1%) were considered effective, while in the TACE group, 24 out of 43 patients (55.8%) were considered effective. The difference between the two groups was statistically significant (P = 0.01), indicating a significant overall difference between the groups (Table 6).
Table 6. - Analysis of efficacy from 6 to 12 months after surgery RFA (39) TACE (43) P-value Validity 32 (82.1%) 24 (55.8%) 0.01 Not validity 7 (17.9%) 19 (44.2%)MRI of RFA before (a) and 1 month after (b) shows a significant reduction in the size of the hemangioma (Fig. 1).
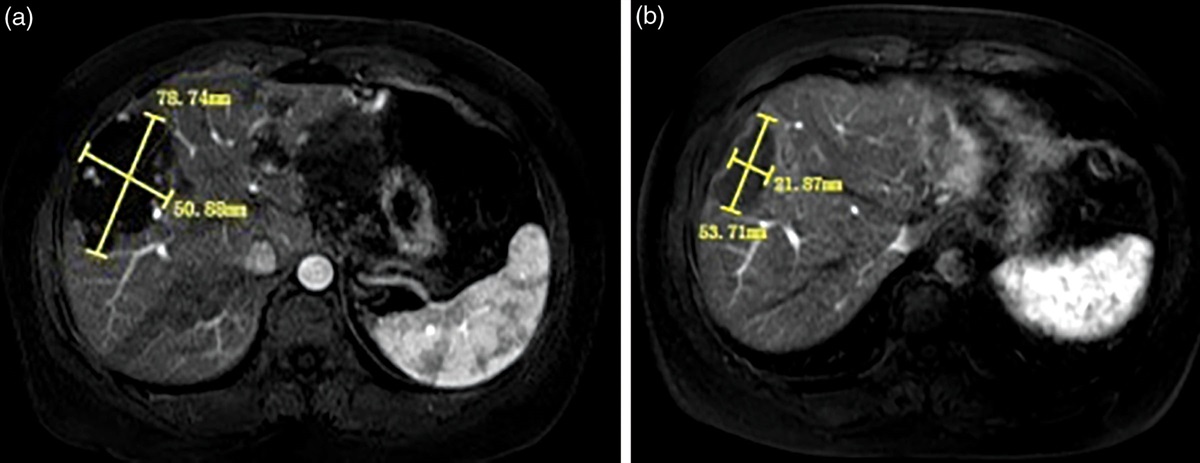
 Fig. 1.:
Fig. 1.: MRI of RFA before (a) and 1 month after (b) shows a significant reduction in the size of the hemangioma.
Enhanced CT of TACE before (c) and 22-month postoperative MRI (d) showed a significant reduction in the size of the hemangioma (Fig. 2).
 Fig. 2.:
Fig. 2.: Enhanced CT of TACE before (c) and 22-month postoperative MRI (d) showed a significant reduction in the size of the hemangioma.
DiscussionMany centers still consider surgical resection as the primary treatment option for HH [24,25]. However, for patients with early-detected LHH, the high risks associated with surgical resection may make them reluctant to undergo surgery. High-risk events related to surgical resection include a mortality rate of 0.5–2% [26], significant blood loss, prolonged postoperative hospitalization, and perioperative complications of Grade II [23] or higher such as liver dysfunction, bile leakage, and incision infections, among others [26,27]. Apart from surgical treatment, there is no standardized approach in the medical community for selecting minimally invasive treatments. Prior research by individuals like Gu and Yu (2015) [15], Zhang et al. (2016) [12] and Shi et al. (2020) [28] has suggested that both thermal ablation and IE are safe and effective in the short term for the treatment of HHs. Compared to traditional surgical resection, thermal ablation and IE are associated with less intraoperative bleeding, shorter postoperative hospitalization, and lower complication rates, among other advantages [12,15]. This study specifically focuses on comparing the safety and efficacy of RFA and TACE in the treatment of HH.
The determination of the time of efficacy assessment of RFA and TACE in this study was based on previous studies. On the one hand, research suggests that the period of tumor shrinkage following TACE for treating HH occurs primarily within the first 12 months postoperatively, with minimal changes observed beyond 12 months [19,29]. On the other hand, although there hasn’t been explicit research on the contraction period of HH treated with RFA, relevant study [30] data suggests that the most significant volume changes occur within the first 12 months following thermal ablation. In summary, our center conducted a statistical analysis of follow-up data for RFA and TACE within 6–12 months postoperatively. The data from our center indicates that the efficacy rate in the RFA group (82.1%) during the 6–12-month postoperative period is significantly higher than that in the TACE group (55.8%, P = 0.01). This suggests that within the 6–12-month postoperative timeframe, the treatment outcomes of the RFA group are significantly superior to those of the TACE group. In 2021, Wu et al. [16] conducted a long-term follow-up study of patients who underwent RFA treatment for LHH, with an average follow-up time of 35 ± 29 months (range 6–120 months). Their study concluded that RFA is a safe and effective minimally invasive method for treating LHH. However, more data are needed to prove the safety of RFA for treating GHH. The study did not find any deaths or recurrences related to RFA, nor were there delayed complications (such as local tumor progression, bile duct injury, or liver abscess formation). However, in our study, 7 patients in the RFA group had a follow-up enhanced CT examination at 6–12 months and found recurrence of HH. As for whether TACE remains effective in the long term for treating HH, there is currently no consensus. In 2017, Liu et al. [20] found that the long-term effects of TACE for treating HH were not ideal and carried a risk of serious complications. The study included 55 patients, with 53 patients completing a 5-year long-term follow-up. Only 19 patients (19/53, 35.8%) had their HH either decrease in size or remain stable, while the HH continued to grow in the other 34 patients (34/53, 64.2%). Among them, 14 patients initially experienced a reduction in the size of HH followed by growth. The authors analyzed that this result may be due to the presence of nourishing blood vessels outside the hepatic artery supplying the HH. Four patients (4/55, 7.3%) experienced severe complications, with 2 patients requiring liver resection for postoperative bile cysts, and 2 patients recovered after drainage for liver abscesses. In 2021, Torkian P [18] presented a contrasting conclusion. They conducted a meta-analysis and found that using BLE, PYG, or ethanol in combination with L for TAE was safe and effective. In their study, all participants successfully underwent TAE, with a clinical response rate of 63.3–100% postoperatively. There were no reported deaths, and no severe complications occurred. In 2022, Yuan B [19] also considered TAE combined with BLE as a safe and effective method to improve abdominal symptoms caused by HH. It demonstrated reliable medium-term (≥3 years) and long-term (≥5 years) clinical and radiological success rates.
On the first day after surgery, the levels of WBC, ALT, AST, and TBIL in both the RFA group and the TACE group were significantly higher than the preoperative levels. Furthermore, this study found that the difference in blood biochemical parameters before and after surgery in the RFA group was greater than that in the TACE group. The changes in ALT and AST levels may be attributed to damage to normal liver tissue. The mechanism of RFA treatment for liver vascular tumors involves the vibration and friction of ions in the liver tissue surrounding the radiofrequency needle, converting radiofrequency current into heat energy, leading to tissue coagulation [31], with temperatures reaching up to 100 °C. Therefore, it is inevitable to accidentally damage normal liver tissue during RFA surgery. The damage to normal liver tissue by TACE is due to the cytotoxic effect of drugs such as Bleomycin not only on the endothelial cells of blood vessels but also on the liver tissue itself. Despite the super-selective nature of embolization, there may still be a small amount of BLE retained in normal liver tissue. Research suggests that the elevation of ALT and AST after RFA and TACE is temporary and returns to normal within 1–2 weeks [12,17,19]. In the RFA group, hemolytic jaundice may occur after surgery, which is attributed to the destruction of red blood cells during the RFA process. Studies have shown that the change in TBIL is proportional to the tumor volume [17]. Regarding changes in WBC after RFA, in 2022, Sun WB and others proposed the concept of Systemic Inflammatory Response Syndrome (SIRS) [32] after RFA. The important reasons for the occurrence and development of SIRS after RFA are the release of heat generated during the RFA process into the bloodstream, damage to endothelial cells inside the tumor, and the destruction of red blood cells, leading to a series of systemic reactions. The duration of ablation and tumor volume are also factors related to SIRS [
留言 (0)