
記住我
Inflammatory bowel disease (IBD), namely, Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic condition that continues to increase in incidence [1,2] worldwide. The management of the disease is complex, as it includes invasive diagnostics and imaging. Fortunately, several new treatments, including monoclonal antibodies against tumour necrosis factor-alpha, integrins, interleukins, and Janus kinase inhibitors [3], have become available in recent years. Nevertheless, the management of these patients typically involves multidisciplinary teams due to many aspects of the disease and treatments. Because of this, there is a tendency to centralise patients in a few specialised IBD centres with sufficient expertise and resources in many countries, with the argument that this will result in better care than if patients were treated locally in smaller nonacademic centres, where gastroenterologists are generally less subspecialized in specific conditions and thus could not provide equally good care as their IBD-subspecialized peers in academic centres who devote more time to IBD care.
The caveat here, however, is that academic centres are typically located only in larger cities, forcing patients to travel long distances and consuming a great deal of time [4]. Additionally, many patients, especially when suffering from a flare, perceive this as a tremendous burden. Furthermore, patients with disease or treatment complications will typically seek help in local environments. Additionally, the rapidly increasing prevalence of patients burdens academic medical centres in many countries; therefore, it is challenging to provide sufficient resources for all IBD patients only in academic centres.
Because of the above-described issues, several years ago, the decision to decentralise IBD patient care was made in Slovenia. The two academic medical centres located in Ljubljana (University Medical Centre Ljubljana) and Maribor (University Medical Centre Maribor) offer support to four other nonacademic medical centres (general hospitals Celje, Jesenice, Izola, and diagnostic centre Bled), especially when step-up to/loss of response to advanced treatments or when complications of disease that need interventional radiology or surgical management are encountered.
However, it is not clear whether patients receive comparable treatments in nonacademic compared to academic centres. To our knowledge, a comparison of IBD patients’ phenotypes and treatment approach with biologicals in academic vs. nonacademic settings has not yet been performed. Nevertheless, this knowledge would be important, as it could lead to the organisation of IBD units in different countries in light of the rapidly increasing number of patients.
The aim of this study was thus to explore and compare the phenotypes of IBD patients and their treatment approach with biologicals in academic vs. nonacademic IBD centres in Slovenia. To do this, we used prospectively collected data in the Slovenian national IBD registry based on the European Crohn’s and Colitis Organisation (ECCO)-powered platform UR-CARE.
Methods Data sourceWe used data collected in the UR-CARE Registry for six Slovenian IBD centres, two high-volume academic IBD university tertiary referral centres (University Medical Centre Ljubljana and Maribor), and four nonacademic IBD centres (three general hospitals (two high-volume centres: General Hospital Izola and Celje; one low-volume centre: General Hospital Jesenice) and one independent government-funded low-volume outpatient unit (Diagnostics Centre Bled)). These six centres covered the great majority of patients treated with biological treatments in Slovenia at the time of data extraction. In Slovenia, there are no limitations on the choice of specific biological drug since 2019, therefore the availability of biological drugs is similar in academic and nonacademic IBD centres. However, before initiation of biological treatment, every patient is presented to the multidisciplinary IBD team in one of the two academic IBD centres. After the approval of the indication for initiation of biological treatment, this can be started by the treating physician. Importantly, the multidisciplinary IBD teams do not advise on the specific biological to be used for a particular patient. The choice of specific drug to be used as first-line treatment is thus left to the treating physician. This is because we believe that shared decision-making between the treating physician and the patient results in optimal selection of specific drug for each patient. However, in case of first-line biological failure or when treatment complications occur, the academic IBD teams give more specific instructions on the choice of the next drug and on the dosing (e.g. dose optimisation, combination with immunomodulators) to assist nonacademic centres.
The UR-CARE Registry is a validated platform for the prospective collection of clinical data developed and supported by the ECCO [5]. The UR-CARE Registry collects patient data, such as disease demographics, disease activity, disease complications, and treatment. In Slovenia, data collection started in September 2020.
Data extraction and analysisTotal data were extracted from the Slovenian UR-CARE Registry on 1 October 2022. In this first Slovenian national analysis, we focussed on describing the disease phenotypes (demographics, disease extension, extraintestinal manifestations) and treatment approach (utilisation of conventional vs. advanced treatments, distribution of different classes of biologicals).
We analysed utilisation of biologicals by comparing treatment episodes between academic and nonacademic centres. A treatment episode was defined as the use of one biological in a specific patient. However, one patient could have more than one treatment episode. For example, when a patient was exposed to two different biologicals during follow-up, we defined the first treatment episode as the time treated with the first biological and the second treatment episode as the time treated with the second biological.
Descriptive statistics are presented as the means ± standard deviations for parametric variables and percentages for categorical variables. To analyse potential differences between academic vs. nonacademic centres, we used the chi-square/Fisher’s exact test or t-test when the data were normally distributed or the Mann–Whitney U test as appropriate when variables had abnormal distributions. Statistical significance for all tests was set at P < 0.05.
Data collection and analyses were performed using Microsoft Excel software (version 2301, build 16.0.16026.20196) and SPSS 21.0 (IBM Inc., Chicago, Illinois, USA). This study was approved by the National Medical Ethics Committee of Slovenia (ID 0120-576/2019/7).
Results Patient characteristics and disease phenotypes Overall characteristics of the cohortAt the time of data extraction, the Slovenian UR CARE Registry included 2748 patients with IBD. Demographic data are presented in Table 1 (row 1) and include patients from 6 different IBD centres in Slovenia. The majority of patients were diagnosed with CD (51.1%), followed by UC (45.0%), and only a small number of patients had unclassified IBD (3.5%). A minority of data regarding the diagnosis (0.4%) were missing from the registry and were classified as missing. The proportion between the sexes was similar. Patients with CD were on average younger than patients with UC at diagnosis. Perianal disease in CD cases was detected in 264 (18.8%) out of 1405 patients (Table 1). Disease extension is shown in Supplementary Figure 1, supplemental digital content 1, https://links.lww.com/EJGH/B19 for CD, and Supplementary Figure 2, supplemental digital content 1, https://links.lww.com/EJGH/B19 for UC patients. Seventy percent of patients with CD had ileal involvement, and approximately half had colonic disease. Approximately half of UC patients had disease extension beyond the splenic flexure. Most, but not all, patients with UC had an affected rectum (93.8%).
Table 1. - Disease phenotype by academic vs. nonacademic inflammatory bowel disease centre in Slovenia Overall Academic centres Nonacademic centres P-value Total number of patients with IBD 2748 2319 (84.4%) 429 (15.6%) CD, N (%) 1405 (51.1%) 1191 (51.4%) 214 (49.9%) 0.656CD, Crohn’s disease; IBD, inflammatory bowel disease; IBD-U, unclassified IBD; UC, ulcerative colitis.
Demographic data classified by type of IBD centre (academic vs. nonacademic) are shown in Table 1 (rows 2 and 3). The overall characteristics of patients treated in academic IBD centres were similar to those of patients treated in nonacademic IBD centres. Data per respective IBD centre are shown in Supplementary Table 1, supplemental digital content 1, https://links.lww.com/EJGH/B19. The proportions of IBD patients with risk factors for disease complications (CD: ileal disease, perianal disease; UC: extensive colitis) were similar in academic compared to nonacademic centres. The only significant difference was age at diagnosis among patients with CD, with academic centres having patients that were approximately 5 years younger at diagnosis compared to nonacademic centres.
Biological treatment approach Overall treatment approach in the cohortIn total, 1687 patients included in the registry at the time of data extraction underwent 2781 treatment episodes with biologicals (adalimumab N = 703 (originator N = 500, biosimilars N = 203), golimumab N = 79, infliximab 886 (originator N = 339, biosimilars N = 547), ustekinumab N = 456, vedolizumab N = 653, other off-label biologicals N = 4). Of these, 703/1687 (42%) discontinued first-line biologicals, 280/1687 (17%) discontinued second-line biologicals and 87/1687 (5%) discontinued third-line biologicals. A detailed sequence of the prescription of biological drugs is shown in Supplementary Table 2, supplemental digital content 1, https://links.lww.com/EJGH/B19.
Comparison of academic vs. nonacademic inflammatory bowel disease centresThe total utilisation of biologicals by drug class was similar in academic vs. nonacademic centres. Comparison of total treatment episodes by drug class in academic and nonacademic patients did not show differences (P = 0.949) (Table 2). However, statistical significance was observed for ongoing biological therapy by drug class in academic centres compared to nonacademic centres (Table 3). In academic centres, slightly fewer patients were receiving TNF-alpha inhibitors than in nonacademic IBD centres (48% vs. 57%). A reciprocal difference was observed for anti-integrin vedolizumab and anti-IL-12/23 drug ustekinumab, with slightly higher utilisation in academic IBD centres compared to nonacademic IBD centres.
Table 2. - Number of prescriptions (treatment episodes) of biologicals by drug class in academic vs. nonacademic inflammatory bowel disease centres Overall Academic Nonacademic P-value All 2782 2499 283 0.949 Ustekinumab 459 (16%) 414 (17%) 45 (16%) Vedolizumab 654 (24%) 588 (24%) 66 (23%) TNF-alpha inhibitors 1669 (60%) 1497 (60%) 172 (61%)When we classified data by disease phenotype (CD vs. UC), we observed that this difference was driven by CD patients, as these patients were less often receiving TNF-alpha inhibitors in academic centres than in nonacademic centres. Conversely, ustekinumab was more often used in academic centres than in nonacademic centres (Table 4).
Table 4. - Number of patients with ongoing biological treatment by drug class in academic vs. nonacademic inflammatory bowel disease centres (Crohn’s disease) Overall Academic Nonacademic P-value All 942 816 126 0.004 Ustekinumab 266 (28.2%) 243 (29.8%) 23 (18.3%) Vedolizumab 160 (17.0%) 143 (17.4%) 17 (13.5%) TNF-alpha inhibitors 516 (54.8%) 430 (52.7%) 86 (68.2%)These differences were not observed for UC (Table 5). Similarly, we did not observe a difference in the proportion of patients with UC with ongoing vedolizumab treatment in academic compared to nonacademic centres.
Table 5. - Number of patients with ongoing biological treatment by drug class in academic vs. nonacademic inflammatory bowel disease centres (ulcerative colitis) Overall Academic Nonacademic P-value All 531 455 76 0.759 Ustekinumab 83 (15.6%) 69 (15.2%) 14 (18.4%) Vedolizumab 234 (44.1%) 201 (44.2%) 33 (43.4%) TNF-alpha inhibitors 214 (45.4%) 185 (40.6%) 29 (38.2%)Additionally, the time to initiation of biologicals decreased during recent years to a similar extent in both academic and nonacademic IBD centres (Table 1, rows 11–12).
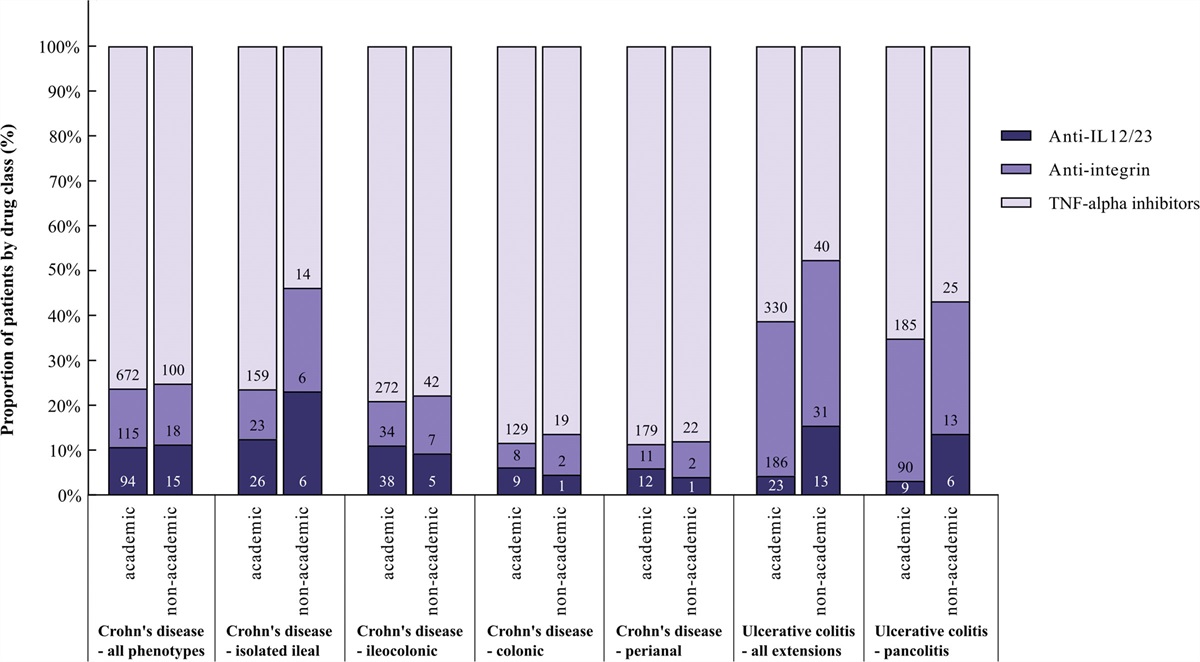
Similarly, TNF-alpha inhibitors were prescribed slightly less often as first-line biologicals in academic centres than in nonacademic centres (TNF-alpha inhibitors: 67.5% vs. 74.0%). Conversely, vedolizumab (20.3% vs. 17.9%) and ustekinumab (12.1% vs. 8.1%) were slightly more often first-line biologicals in academic than in nonacademic centres (P = 0.0096). The choice of first-line treatment in academic vs. nonacademic centres, classified by specific disease phenotype, is shown in Fig. 1.
 Fig. 1.:
Fig. 1.: Choice of first-line biological treatment in academic vs. nonacademic centres for specific phenotypes of inflammatory bowel disease.
Intravenous TNF-alpha inhibitors were slightly less often started as first-line treatment than subcutaneous TNF-alpha inhibitors in academic compared to nonacademic centres (534/1025 (52.1%) vs. 91/143 (63.6%), P = 0.01). This difference was driven mainly by CD as intravenous TNF-alpha inhibitors were chosen in 311/672 (46.3%) patients in academic centres compared to 60/100 (60.0%) patients in nonacademic centres (P = 0.01). In UC this difference was not observed as intravenous TNF-alpha inhibitors were chosen in 213/330 (64.5%) patients in academic compared to 29/40 (72.5%) patients in nonacademic centres (P = 0.318).
DiscussionThe burden of IBD has increased during the last decade to the extent that precludes the management of these patients only in highly specialised IBD academic centres. Many patients therefore have to be treated outside specialised academic settings. However, it is reassuring that our analysis of the nationwide Slovenian IBD registry confirmed that IBD patients received similar biological treatments in academic and nonacademic medical centres. We observed only slight differences in the choice of first-line biologicals with less use of TNF-alpha inhibitors for CD in academic settings but not for UC. In the last 2 years, we have witnessed a decrease in time from diagnosis to the introduction of biologics both in academic and nonacademic IBD centres. Our data thus suggest that IBD can also be effectively managed outside academic settings, provided that continuous support is offered by academic teams. This is an important clinical message that could guide national strategies for many countries with a rapidly increasing burden of IBD.
The disease phenotype of IBD was similar in academic and nonacademic centres, with roughly equal proportions of CD and UC patients. Similar results were also observed for disease location, as the proportions of ileocolonic CD, isolated ileum CD and perianal CD were similar in both academic and nonacademic centres and comparable with those reported by others [6,7–10]. Additionally, the proportion of UC patients with pancolitis in our study was in line with other reports [6,9,10]. The same was observed for the proportion of patients with perianal fistulizing disease (18.8%) in our study, as this was similar to that reported by others [11–14]. The added value of our study is that we observed that the proportion of perianal fistulizing disease patients was similar in academic and nonacademic centres, suggesting that these patients are also successfully managed outside highly specialised teams. However, we did not have data on combined immunosuppression or the rate of dose optimisation for these patients. Nevertheless, we believe that continuous support offered by the two types of academic centres allows efficient treatment of these patients by community gastroenterologists outside academic medical centres in Slovenia.
The demographics of patients treated at academic and nonacademic medical centres were similar. The only difference was that patients were 5 years younger at diagnosis of CD in academic centres. Our explanation for this is that perhaps younger patients move more easily to larger cities than older patients, perhaps due to enrolment in schools and employment opportunities. However, we did not specifically investigate this, and there are no published data on similar comparisons in the literature.
Treatment approaches with biological drugs were generally in line with those reported elsewhere [15]. Approximately half of the patients were treated with TNF-alpha inhibitors, and the others were treated with ustekinumab or vedolizumab. Similarly, as reported by others, ustekinumab was more often used in CD and vedolizumab in UC [16,17]. Our main observation here was that in academic centres, TNF-alpha inhibitors were slightly less often a first-line biological for CD than in nonacademic centres. Consequently, the proportion of patients with ongoing ustekinumab treatment was slightly higher (approximately 10%) in academic centres than in nonacademic centres. Interestingly, in line with this is a recent report in which adoption of ustekinumab was higher in high-volume urban facilities than in rural facilities and in facilities with greater teamwork [18]. Despite this difference being small, it could still be relevant due to the more favourable safety profiles of ustekinumab compared to TNF-alpha inhibitors with comparable efficacy demonstrated recently [19]. However, time to initiation of biologicals from diagnosis of IBD was similar in both academic and nonacademic medical centres, further indicating that patients are approached similarly in both settings. An interesting observation was also that first-line TNF-inhibitor was more often subcutaneous in academic centres, but intravenous in nonacademic centres in CD. This might be due to higher local availability for infusions in lower volume nonacademic centres.
In general, the proportion of vedolizumab-treated patients with CD was low in both academic and nonacademic centres, despite the documented efficacy for healing different bowel segments, including the ileum [20]. Tools such as a clinical decision support tool (CDST) could perhaps assist in decision-making in such cases in the future [21]. Such scoring systems perhaps would be of more value for nonacademic centres where the proportion of CD patients treated with vedolizumab is particularly low. The proportion of UC patients treated with vedolizumab was similar and high in both academic and nonacademic settings. Nevertheless, the use of TNF inhibitors was high among patients with UC. This can be at least partly explained by the fact that before 2019 in Slovenia, vedolizumab and ustekinumab were reserved for second-line treatment after TNF-alpha inhibitors had failed.
We acknowledge some important limitations of our report. Not all patients with IBD in Slovenia were entered into the UR-CARE Registry at the time of data extraction. Additionally, most centres contributed to the registry by first entering patients treated with biologicals at this early stage; thus, we were not able to compare the proportion of patients treated with biologicals vs. conventional drugs in different centres. However, since the disease phenotypes of biologically treated patients were similar in academic and nonacademic centres, we believe that patient selection for biologicals was similar in both settings. In line with this is also the similar time from diagnosis to initiation of first biologicals in both settings. We also failed to analyse treatment outcomes in academic vs. nonacademic centres, but for IBD, this difference might only be evident after prolonged periods [22]. Because of this, we will be able to assess potential differences in outcomes only a few years after launch of the registry in Slovenia. We also did not have data on the dose optimisation of biologicals and thus were unable to compare this aspect of treatment in both settings. Although the incidence of extraintestinal manifestations in our cohort was in line with those reported by others [23,24], we cannot exclude that at this early stage for the UR-CARE Registry in Slovenia, data capture was insufficient for extraintestinal manifestations; thus, we might have underestimated its true incidence. Additionally, due to the low number of specific extraintestinal manifestations, we were unable to perform more focussed analyses. It should also be acknowledged that in our country two multidisciplinary IBD teams in both academic centres support local hospitals. Thus, our findings cannot be generalised if such support is not provided.
In conclusion, this analysis of nationwide data indicated that IBD patients receive similar biological treatments early in the course of the disease in academic and nonacademic IBD centres. This is a reassuring message for patients and physicians, as it indicates that IBD can be successfully managed outside highly specialised high-volume academic settings. This finding has important implications for stakeholders, as it suggests that decentralisation of IBD care is a valid approach to cope with the increasing prevalence of IBD.
AcknowledgementsWe thank our IBD nurses Carmen Bobnar Sekulić, Tadeja Polanc, and Andreja Planinc for data acquisition from the UR-CARE Registry.
This work was partially financially supported by the Slovenian Research Agency (ARRS Grant J3-4499).
KT, DŠ, and DD conceptualised the study, collected the data, performed the analysis and wrote the manuscript. All authors contributed to data collection. All authors critically reviewed and revised the manuscript, and all authors approved the final manuscript as submitted. Guarantor of the article: David Drobne.
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Conflicts of interestKT has served as a speaker, consultant, and/or advisory board member for Pfizer, Abbvie, and Krka. JH has served as a consultant for Abbvie, Alimentiv Inc., Janssen, and Takeda. UK has served as a speaker, consultant, and/or advisory board member for MSD, Takeda, Medtronic, Zaloker & Zaloker, Abbot, and Abbvie. GN has served as a speaker, consultant, and/or advisory board member for Takeda in Ethicon. RŠ has served as a speaker, consultant, and/or advisory board member for Takeda, Abbvie, Lek, Pfizer, and Janssen. MŽ has served as a speaker, consultant, and/or advisory board member for Abbvie. JB has served as a speaker, consultant, and/or advisory board member for Abbvie, Takeda, Pfizer, Janssen, Viatris, Lek, and Krka. AO has served as a speaker, consultant, and/or advisory board member for MSD, Abbvie, Takeda, Pfizer, Janssen, Krka, Oktal Pharma, Novartis, Amgen, Biogen, Lek, Abbott, Mediasi, Sobi, dr Falk Pharma, and Carso Pharm. CPD has served as a speaker, consultant, and/or advisory board member for MSD, Abbvie, Takeda, Pfizer, and Janssen. TM has served as a speaker, consultant, and/or advisory board member for MSD, Abbvie, Takeda, Krka, Janssen, Amgen, and Pfizer. NK has served as a speaker, consultant, and/or advisory board member for Lek, Krka, Abbvie, Sobi, dr Falk Pharma, Janssen, and Ferring. AZ has served as a speaker, consultant, and/or advisory board member for Abbvie, Takeda, Pfizer, Ferring, Janssen, Krka, Amgen, Biogen, Lek, Sobi, and dr Falk Pharma. NJB has served as a speaker, consultant, and/or advisory board member for Amgen, Pfizer, Janssen, Abbvie, and Lek. NS has served as a speaker, consultant, and/or advisory board member for AbbVie, Takeda, Janssen, Pfizer, Oktal Pharma, Novartis, Sobi, Amgen, Biogen, and MSD. GN has served as a speaker, consultant, and/or advisory board member for Abbvie, Takeda, Pfizer, Janssen, Oktal Pharma, Sobi, Krka, Sandoz, and Biogen. TK has served as a speaker, consultant, and/or advisory board member for Takeda, MSD, Abbvie, Janssen, Ferring, and Abbvie. BŠ has served as a speaker, consultant, and/or advisory board member for MSD, Abbvie, Takeda, Pfizer, and Janssen. DD has served as a speaker, consultant, and/or advisory board member for MSD, Abbvie, Takeda, Pfizer, Janssen, Krka, Eli Lilly, Oktal Pharma, Roche, Novartis, Amgen, and Lek. For the remaining authors, there are no conflicts of interest.
References 1. Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2017; 390:2769–2778. 2. Mak WY, Zhao M, Ng SC, Burisch J. The epidemiology of inflammatory bowel disease: east meets west. J Gastroenterol Hepatol 2020; 35:380–389. 3. Moreno LO, Fernández-Tomé S, Abalo R. Biological treatments in inflammatory bowel disease: a complex mix of mechanisms and actions. Biologics 2021Aug 10; 1:189–210. 4. Borren NZ, Conway G, Tan W, Andrews E, Garber JJ, Yajnik V, et al. Distance to specialist care and disease outcomes in inflammatory bowel disease. Inflamm Bowel Dis 2017; 23:1234–1239. 5. Burisch J, Gisbert JP, Siegmund B, Bettenworth D, Thomsen SB, Cleynen I, et al. Validation of the ‘United Registries for Clinical Assessment and Research’ [UR-CARE], a European Online Registry for Clinical Care and Research in Inflammatory Bowel Disease. J Crohns Colitis 2018; 12:532–537. 6. Nuij VJAA, Zelinkova Z, Rijk MCM, Beukers R, Ouwendijk RJT, Quispel R, et al.; Dutch Delta IBD Group. Phenotype of inflammatory bowel disease at diagnosis in the Netherlands: a population-based inception cohort study (the Delta Cohort). Inflamm Bowel Dis 2013; 19:2215–2222. 7. Ng SC, Tang W, Ching JY, Wong M, Chow CM, Hui AJ, et al.; Asia–Pacific Crohn's and Colitis Epidemiologic Study (ACCESS) Study Group. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-Pacific Crohn’s and colitis epidemiology study. Gastroenterology 2013; 145:158–165.e2. 8. Lakatos L, Kiss LS, David G, Pandur T, Erdelyi Z, Mester G, et al. Incidence, disease phenotype at diagnosis, and early disease course in inflammatory bowel diseases in Western Hungary, 2002-2006. Inflamm Bowel Dis 2011; 17:2558–2565. 9. Sjöberg D, Holmström T, Larsson M, Nielsen AL, Holmquist L, Ekbom A, et al. Incidence and natural history of ulcerative colitis in the Uppsala Region of Sweden 2005-2009 - results from the IBD cohort of the Uppsala Region (ICURE). J Crohns Colitis 2013; 7:e351–e357. 10. Sjöberg D, Holmström T, Larsson M, Nielsen AL, Holmquist L, Ekbom A, et al. Incidence and clinical course of Crohn’s disease during the first year - results from the IBD Cohort of the Uppsala Region (ICURE) of Sweden 2005-2009. J Crohns Colitis 2014; 8:215–222. 11. Zhao M, Lo BZS, Vester-Andersen MK, Vind I, Bendtsen F, Burisch J. A 10-year follow-up study of the natural history of perianal Crohn’s disease in a Danish population-based inception cohort. Inflamm Bowel Dis 2019; 25:1227–1236. 12. Lightner AL. Perianal Crohn’s disease. Dis Colon Rectum 2020; 63:1023–1026. 13. Schwartz DA, Loftus EV, Tremaine WJ, Panaccione R, Harmsen WS, Zinsmeister AR, et al. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology 2002; 122:875–880. 14. Panés J, Rimola J. Perianal fistulizing Crohn’s disease: pathogenesis, diagnosis and therapy. Nat Rev Gastroenterol Hepatol 2017; 14:652–664. 15. Huynh L, Hass S, Peyrin-Biroulet L, Duh MS, Sipsma H, Cheng M, et al. Real-World Treatment Patterns and Physician Preferences for Biologics in Moderate-to-Severe Inflammatory Bowel Disease: Retrospective Chart Review in Europe. Crohns Colitis 360. 2022; 4:otac001. 16. Biemans VBC, van der Woude CJ, Dijkstra G, van der Meulen-de Jong AE, Löwenberg M, de Boer NK, et al.; Dutch Initiative on Crohn and Colitis (ICC). Ustekinumab is associated with superior effectiveness outcomes compared to vedolizumab in Crohn’s disease patients with prior failure to anti-TNF treatment. Aliment Pharmacol Ther 2020; 52:123–134. 17. Helwig U, Mross M, Schubert S, Hartmann H, Brandes A, Stein D, et al. Real-world clinical effectiveness and safety of vedolizumab and anti-tumor necrosis factor alpha treatment in ulcerative colitis and Crohn’s disease patients: a German retrospective chart review. BMC Gastroenterol 2020; 20:211. 18. Cohen-Mekelburg S, Van T, Berinstein JA, Yu X, Costa DK, Wallace BI, et al. Characteristics of facilities with early and rapid ustekinumab adoption for patients with inflammatory bowel disease. Am J Gastroenterol 2023; 118:1688–1692. 19. Sands BE, Irving PM, Hoops T, Izanec JL, Gao LL, Gasink C, et al.; SEAVUE Study Group. Ustekinumab versus adalimumab for induction and maintenance therapy in biologic-naive patients with moderately to severely active Crohn’s disease: a multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet 2022; 399:2200–2211. 20. Danese S, Sandborn WJ, Colombel JF, Vermeire S, Glover SC, Rimola J, et al. Endoscopic, radiologic, and histologic healing with vedolizumab in patients with active Crohn’s disease. Gastroenterology 2019; 157:1007–1018.e7. 21. Dulai PS, Boland BS, Singh S, Chaudrey K, Koliani-Pace JL, Kochhar G, et al. Development and validation of a scoring system to predict outcomes of vedolizumab treatment in patients with Crohn’s disease. Gastroenterology 2018; 155:687–695.e10. 22. Khanna R, Bressler B, Levesque BG, Zou G, Stitt LW, Greenberg GR, et al.; REACT Study Investigators. Early combined immunosuppression for the management of Crohn’s disease (REACT): a cluster randomised controlled trial. Lancet 2015; 386:1825–1834. 23. Bernstein CN, Blanchard JF, Rawsthorne P, Yu N. The prevalence of extraintestinal diseases in inflammatory bowel disease: a population-based study. Am J Gastroenterol 2001; 96:1116–1122. 24. Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal manifestations of inflammatory bowel disease: current concepts, treatment, and implications for disease management. Gastroenterology 2021; 161:1118–1132.
留言 (0)