
記住我
Liver cancer is the leading cause of global cancer-related deaths and ranks fifth in the USA. Over 90% of liver cancer cases are attributed to hepatocellular carcinoma (HCC) [1]. Major causes of HCC include infection with hepatitis B virus (HBV) and hepatitis C virus, heavy alcohol consumption, intake of aflatoxin B1, smoking, and nonalcoholic fatty liver disease (NAFLD) resulting from obesity and insulin resistance [2]. Due to the implementation of HBV vaccines and direct-acting antivirals, NAFLD is projected to become the predominant cause of HCC in numerous countries by 2030 [3]. NAFLD can progress from simple steatosis to nonalcoholic steatohepatitis, liver fibrosis, and cirrhosis, and eventually, HCC [4]. Currently, the prognosis of HCC is unfavorable, making the exploration of factors influencing HCC prognosis a prominent research topic.
The Surveillance, Epidemiology, and End Results (SEER) database is a nationally representative, population-based cancer reporting system that includes all cancer cases within a specific geographic area of the USA. Analyzing longitudinal trends in cancer diagnosis, treatment, and survival through SEER contributes to a more intuitive understanding of cancer diagnosis and treatment [5]. Numerous studies have demonstrated the utility of the SEER database for survival and prognosis analysis of HCC. For example, Lin et al. investigated the impact of liver fibrosis on microvascular invasion and the prognosis of HCC with isolated nodules using the SEER database [6]. Zhu et al. identified clinicopathological factors influencing survival after hepatectomy in patients with early HCC and hepatitis B virus-associated cirrhosis using the SEER database [7]. The evidence above suggests that the SEER database is a commonly used and reliable tool for discussing HCC prognosis.
Numerous studies have demonstrated that sex is one of the key factors influencing cancer survival and prognosis, including colon [8], stomach [9], and esophageal cancers [10]. Research has shown that the majority of HCC patients are male, with a male-to-female ratio ranging between 1.5 and 4.0 [11,12], indicating that sex may also be a crucial factor influencing the prognosis of HCC patients. Additionally, the clinical features of tumors differ between men and women [11]. Therefore, we downloaded clinical data of HCC patients from the SEER database spanning from 2010 to 2015 and explored the impact of clinical features of HCC patients on survival and prognosis in both men and women.
Methods Data downloadA retrospective cohort analysis of patients with HCC was performed using the SEER (https://seer.cancer.gov/) database, covering 3486 cases from 2010 to 2015. Patients were excluded if their survival time and survival status were not available. Demographic and clinicopathologic information, including age at diagnosis, race, Purchased/Referred Care Delivery Areas, SEER historic stage, tumor size [determined by computed tomography (CT)], T stage (T1, T2, T3, T4), N stage (N0, N1, N2), M stage (M0, M1), presence of brain, bone, and lung metastases, whether the patient received chemotherapy or not, and survival follow-up (survival time and survival status) were downloaded using SEER*Stat software.
The cancer diagnosis, staging, and metastatic information in the SEER database mainly originate from medical records, pathology reports, cancer registries, and records of radiotherapy. HCC diagnosis in our study cohort primarily emanates from pathology reports obtained from medical institutions. Pathologists thoroughly examine tissue samples to ascertain the presence of HCC, identify its specific type, and document other pertinent pathological features. Subsequently, this information is recorded in the patients’ medical records and reported to cancer registries. Information on HCC staging is mainly derived from physicians’ diagnoses, surgical records, and relevant imaging studies. The TNM staging system, is used to assess the extent of tumor involvement, lymph node involvement, and metastasis. The identification of distant metastases relies on clinical examinations, imaging studies (such as MRI, CT, and PET scans), and observations made during surgical procedures. The SEER database collects, integrates, and standardizes clinical information from diverse medical records.
Statistical analysisWe used the age of 60 years as a threshold to define the younger and older age groups. In the survival status data, ‘alive’ was coded as 0, and ‘death’ was coded as 1. For the remaining data without clear classification, we uniformly labeled it as ‘Unknown’. We assessed the survival prognostic characteristics of male and female patients across various levels of clinical characteristics. Chi-square tests were utilized to analyze the relationship between sex classification and various clinical features. Features showing significant differences in the Chi-Square test were subsequently subjected to univariate Cox regression analysis to examine their prognostic characteristics. Overall survival (OS) was analyzed using Kaplan–Meier (KM) [13] and differences between survival curves were tested using the log-rank test. Multivariate Cox proportional hazard regression [14] was used to identify the hazard ratios of multiple clinical characteristics prognostic factors. Statistical analysis was performed using R version 4.3.2.
Results Demographic and clinical characteristics of patients with HCCFrom 2010 to 2015, a total of 3486 patients with HCC, including 2682 male patients and 804 female patients, were included in this analysis. The demographic and clinical characteristics of patients (males and females) with HCC are described in Table 1.
Table 1. - The demographic and clinical characteristics of patients (males and females) with hepatocellular carcinoma Female Male P-value Count Percent (%) Count Percent (%) Age 0.001164 60 years 215 6.17 882 25.30 60+ years 589 16.90 1800 51.64 Race 0.003593 Black 85 2.44 299 8.58 Other 222 6.37 588 16.87 White 497 14.26 1795 51.49 PRCDA 0.4905 Not PRCDA 403 11.56 1305 37.44 PRCDA 401 11.50 1377 39.50 Grade 0.1962 Grade I 215 6.17 734 21.06 Grade II 391 11.22 1381 39.62 Grade III 188 5.39 534 15.32 Grade IV 10 0.29 33 0.95 Stage 0.01229 Distant 76 2.18 342 9.81 Localized 524 15.03 1614 46.30 Regional 204 5.85 726 20.83 T 0.1335 T1 426 12.22 1289 36.98 T2 144 4.13 566 16.24 T3 169 4.85 612 17.56 T4 30 0.86 100 2.87 TX 35 1.00 115 3.30 N 0.1522 N0 734 21.06 2386 68.45 N1 39 1.12 174 4.99 NX 31 0.89 122 3.50 M 0.009829 M0 735 21.08 2362 67.76 M1 69 1.98 320 9.18 Bone 0.2627 No 784 22.49 2592 74.35 Yes 20 0.57 90 2.58 Brain 0.1195 No 804 23.06 2670 76.59 Yes 0 0.00 12 0.34 Lung 0.04139 No 780 22.38 2555 73.29 Yes 24 0.69 127 3.64 Size 0.6316 100–150 mm 79 2.27 251 7.20 150–200 mm 31 0.89 87 2.50 200+ mm 71 2.04 277 7.95 50-mm 416 11.93 1354 38.84 50–100 mm 207 5.94 713 20.45 Chemotherapy 0.01465 No/unknown 539 15.46 1669 47.88 Yes 265 7.60 1013 29.06M, distant metastasis; M0, cancer has not spread to other parts of the body; M1, cancer has spread to other parts of the body; N, regional lymph nodes; N0, there is no cancer in nearby lymph nodes; N1, N2, N3, Refers to the number and location of lymph nodes that contain cancer; NX, cancer in nearby lymph nodes cannot be measured; PRCDA, Purchased/Referred Care Delivery Area; T, primary tumor; T1, T2, T3, T4, Refers to the size and/or extent of the main tumor; TX, main tumor cannot be measured.
Regarding age at diagnosis, 822 (25.30%) male patients were younger than 60 years old, and 1800 (51.64%) were older than 60 years. For female patients, 6.17% were younger than 60 years old, and 16.90% were older than 60 years, significantly lower than their male counterparts. As for patients with different ethnicities, among the Black (males: 8.58%, females: 2.44%), White (males: 51.49%, females: 14.26%), and other populations (males: 16.87%, females: 6.37%), the proportion of male patients was higher than that of female patients. The proportions of male patients in different TNM staging systems and with varying tumor sizes were higher than those of female patients. Additionally, the proportion of male patients (39.50%) in Purchased/Referred Care Delivery Areas was greater than that of female patients (11.50%). As for tumor metastasis, the proportion of bone metastasis, brain metastasis, and lung metastasis in men was 2.58%, 0.34%, and 3.64%, respectively, which were higher than that in women (0.57% for bone metastasis, 0% for brain metastasis, and 0.69% for lung metastasis). Regarding the SEER historic stage, the proportion of men with distant (9.81%), localized (46.30%), and regional (20.83%) spread was higher than that of women (2.18%, 15.03%, and 5.85%, respectively). Regarding tumor grade, the proportion of early-grade (I, II, III, and IV) patients in men was 21.06%, 39.62%, 15.32%, and 0.95%, respectively, higher than the proportion of female patients (I: 6.17%, II: 11.22%, III: 5.39%, and IV: 0.29%). Moreover, the proportion of male patients who received chemotherapy was 29.06%, significantly higher than that of females at 7.60%.
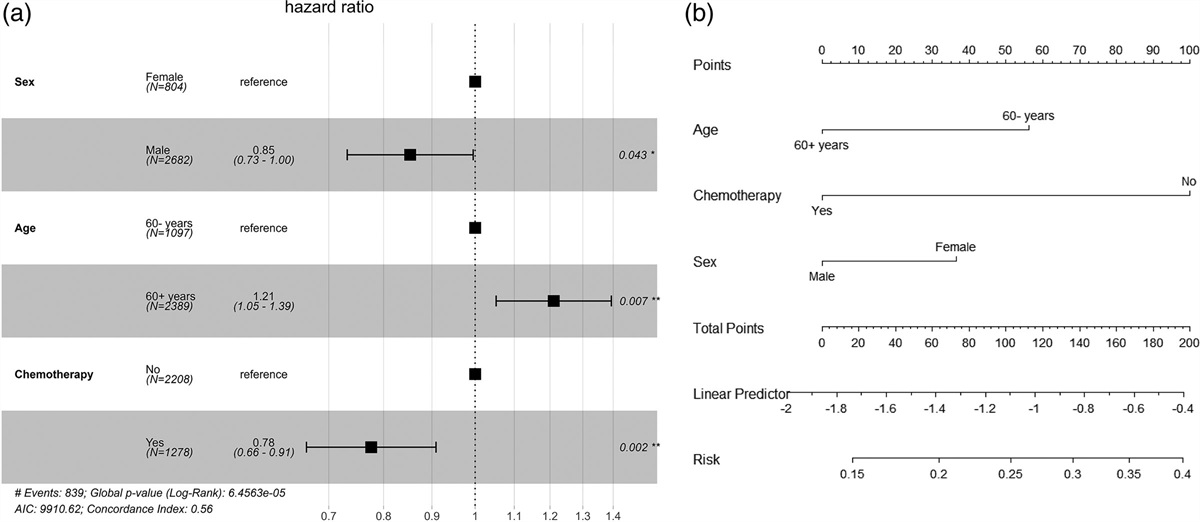
Survival prognosis analysisTo further investigate the influence of clinical features on survival between different genders, we conducted a univariate Cox hazard analysis to identify significant factors, followed by constructing a multivariate Cox regression model. Table 2 highlights that three clinical features, namely age, gender, and the administration of chemotherapy, significantly impact survival (P < 0.05). The results from the multivariate Cox regression analysis underscored the statistical significance of age, gender, and chemotherapy administration (P < 0.05; Fig. 1a), indicating that these factors were independent and significant predictors when forecasting the survival of HCC patients. Figure 1b illustrates that the administration of chemotherapy had the most pronounced effect on patient survival, while gender exhibited a comparatively smaller impact. Among these factors, females displayed a higher probability of survival compared to males, patients under the age of 60 had a greater likelihood of survival than those older than 60 years, and patients who did not receive chemotherapy exhibited a higher survival rate than those who did.
Table 2. - Univariate Cox hazard analysis among male and female patients with hepatocellular carcinoma Characteristic HR 95% CI P-value Age 0.004699 60 years — — 60+ years 1.22 1.06, 1.41 Race 0.7669 Black — — Other 1.01 0.79, 1.29 White 0.96 0.76, 1.20 Stage 0.7217 Distant — — Localized 0.88 0.51, 1.53 Regional 0.82 0.46, 1.47 M 0.2956 M0 — — M1 1.43 0.76, 2.69 lung 0.3358 No — — Yes 1.53 0.68, 3.42 Chemotherapy 0.001508 No — — Yes 0.78 0.66, 0.91 Sex 0.03704 Female — — Male 0.85 0.73, 0.99CI, confidence intervals; HR, hazard ratio; M, distant metastasis; M0, cancer has not spread to other parts of the body; M1, cancer has spread to other parts of the body.
 Fig. 1.:
Fig. 1.: Multivariate Cox proportional hazard regression analysis of overall survival in the retrospective cohort. (a) Multivariable cox regression forest plot. (b) Multivariable cox regression column chart.
KM survival curves constructionBased on the above analysis, we have identified two features that were both associated with gender and HCC prognosis (chemotherapy and age). To further elucidate the impact of these two features on the survival prognosis of HCC patients, we constructed individual feature KM curves within different genders (Fig. 2a and b). No significant difference was observed in survival curves among female patients across different age groups (Fig. 2a). However, among male patients, the survival rate of those under the age of 60 was significantly higher than that of patients aged 60+ years (P = 0.016; Fig. 2a). Figure 2b illustrates that among female patients, the survival rate of those who received chemotherapy was significantly higher than that of those who did not receive chemotherapy (P = 0.00019). In contrast, among male patients, no significant difference was observed (Fig. 2b).
 Fig. 2.:
Fig. 2.: Kaplan–Meier survival curves for overall survival analysis of female (left) and male (right) patients stratified by age at diagnosis (a) and (b) the administration of chemotherapy.
DiscussionMost cancers exhibit sex differences in incidence, mortality, and prognosis [15–18]. Therefore, sex differences are critical issues that cannot be overlooked in oncology research. A previous systematic review noted that women have a survival advantage over men in many cancers. Among the various sex differences observed in cancer manifestations, researchers have noted that some may be associated with occupational and environmental exposures in men [19]. However, in numerous cases, the sex differences observed in many cancers remain unexplained, even when controlling for environmental and genetic factors [20,21]. Therefore, our research focuses on analyzing the effects of clinical indicators on the survival and prognosis of HCC patients of different sexes. Our results suggest that age, gender, and the administration of chemotherapy are factors affecting the prognosis of HCC in different sexes.
We found that the proportion of men with HCC younger than 60 years was higher than the proportion of women (25.30% vs. 6.17%); the proportion of men > 60 years of age with HCC was higher than that of women (51.64% vs. 16.90%) as well. Differences in the age of HCC patients may be related to the body’s hormone levels. The estrogen receptor of hepatocytes has been reported to inhibit the replication and transcription of the hepatitis virus and the release of interleukin-6, a protein associated with chronic hepatitis [22]. Conversely, the androgen receptor plays an opposing role: its activation can enhance the replication of the hepatitis virus and promote the expression of genes related to liver cancer development [23]. Numerous epidemiological studies have linked a lower risk and higher survival rate to increased estrogen exposure in adult females [24,25]. Selecting age 60 as the cutoff point ensures that patients older than 60 years are postmenopausal [8], further highlighting the significance of hormone levels in both sexes. Additionally, various other factors, including epigenetic and genetic factors, sex hormones, and psychosocial aspects, contribute to the observed differences. These factors result in females having a stronger innate and adaptive immune response, thereby reducing the risk of cancer-related mortality [26]. Furthermore, survival analysis revealed that among male patients, those under the age of 60 exhibited a significantly higher survival rate than their counterparts older than 60 years. Moreover, multivariate regression analysis demonstrated that the hazard ratios for age and gender in HCC patients were 1.21 (reference value 1.05–1.39) and 0.85 (reference value 0.73–1.00), respectively, further confirming the pivotal role of age and gender in influencing HCC prognosis.
Chemotherapy is one of the most important treatment modalities for advanced HCC [27]. Our research findings revealed that the proportion of male patients receiving chemotherapy was 29.06%, significantly higher than that of females at 7.60%. This finding aligns with previous results [28]. Furthermore, multivariate Cox regression analysis indicated that the hazard ratio for HCC patients receiving chemotherapy was 0.78 (reference value 0.66–0.91). Kaplan–Meier survival curves demonstrate a significantly higher survival rate for female patients who received chemotherapy compared to those who did not, whereas no significant difference was observed among male patients. In a study by Kaif et al. based on the SEER database, HCC patients who received chemotherapy also exhibited a significantly longer median OS compared to those who did not receive chemotherapy [29]. These findings aligned with our research results, and collectively, they supported the notion that the decision to receive chemotherapy was one of the crucial factors influencing the prognosis of HCC.
In this study, we explored the impact of clinical features on HCC survival and prognosis in different sexes, but some shortcomings remain. First, this study was primarily based on observational clinical data and lacks experimental validation. Further experimental research was needed to confirm whether the observed associations have causal relationships. Additionally, due to the limitations of the data, certain important biological or molecular factors were not included in the analysis, which could potentially have an impact on the results.
In conclusion, our study revealed that age, gender, and the administration of chemotherapy were important factors affecting the prognosis of male and female HCC patients. Our research provides a theoretical basis for clinical management and has the potential for clinical applications.
AcknowledgementsNone.
Conflicts of interestThere are no conflicts of interest.
References 1. Anwanwan D, Singh SK, Singh S, Saikam V, Singh R. Challenges in liver cancer and possible treatment approaches. Biochim Biophys Acta Rev Cancer. 2020; 1873:188314. 2. Chidambaranathan-Reghupaty S, Fisher PB, Sarkar D. Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification. Adv Cancer Res. 2021; 149:1–61. 3. Ioannou GN. Epidemiology and risk-stratification of NAFLD-associated HCC. J Hepatol. 2021; 75:1476–1484. 4. Anstee QM, Reeves HL, Kotsiliti E, Govaere O, Heikenwalder M. From NASH to HCC: current concepts and future challenges. Nat Rev Gastroenterol Hepatol. 2019; 16:411–428. 5. Doll KM, Rademaker A, Sosa JA. Practical guide to surgical data sets: surveillance, epidemiology, and end results (SEER) database. JAMA Surg. 2018; 153:588–589. 6. Lin E, Zou B, Zeng G, Cai C, Li P, Chen J, et al. The impact of liver fibrosis on microvascular invasion and prognosis of hepatocellular carcinoma with a solitary nodule: a surveillance, epidemiology, and end results (SEER) database analysis. Ann Transl Med. 2021; 9:1310. 7. Zhu Q, Yuan B, Qiao GL, Yan JJ, Li Y, Duan R, et al. Prognostic factors for survival after hepatic resection of early hepatocellular carcinoma in HBV-related cirrhotic patients. Clin Res Hepatol Gastroenterol. 2016; 40:418–427. 8. Ma B, Li Y, Meng Q. The predictive and prognostic value of sex in localized colorectal cancer: a SEER-based analysis. Transl Cancer Res. 2021; 10:2108–2119. 9. Yang D, Hendifar A, Lenz C, Togawa K, Lenz F, Lurje G, et al. Survival of metastatic gastric cancer: Significance of age, sex and race/ethnicity. J Gastrointest Oncol. 2011; 2:77–84. 10. Bohanes P, Yang D, Chhibar RS, Labonte MJ, Winder T, Ning Y, et al. Influence of sex on the survival of patients with esophageal cancer. J Clin Oncol. 2012; 30:2265–2272. 11. Ding J, Wen Z. Survival improvement and prognosis for hepatocellular carcinoma: analysis of the SEER database. BMC Cancer. 2021; 21:1157. 12. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424. 13. Hess AS, Hess JR. Kaplan-Meier survival curves. Transfusion. 2020; 60:670–672. 14. Fisher LD, Lin DY. Time-dependent covariates in the Cox proportional-hazards regression model. Annu Rev Public Health. 1999; 20:145–157. 15. Kauppila JH, Wahlin K, Lagergren P, Lagergren J. Sex differences in the prognosis after surgery for esophageal squamous cell carcinoma and adenocarcinoma. Int J Cancer. 2019; 144:1284–1291. 16. Lim JH, Ryu JS, Kim JH, Kim HJ, Lee D. Gender as an independent prognostic factor in small-cell lung cancer: Inha Lung Cancer Cohort study using propensity score matching. PLoS One. 2018; 13:e0208492. 17. Matteoni S, Abbruzzese C, Villani V, Malorni W, Pace A, Matarrese P, et al. The influence of patient sex on clinical approaches to malignant glioma. Cancer Lett. 2020; 468:41–47. 18. Tian M, Ma W, Chen Y, Yu Y, Zhu D, Shi J, et al. Impact of gender on the survival of patients with glioblastoma. Biosci Rep. 2018; 38:BSR20180752. 19. Ferguson MK, Skosey C, Hoffman PC, Golomb HM. Sex-associated differences in presentation and survival in patients with lung cancer. J Clin Oncol. 1990; 8:1402–1407. 20. Edgren G, Liang L, Adami HO, Chang ET. Enigmatic sex disparities in cancer incidence. Eur J Epidemiol. 2012; 27:187–196. 21. Dorak MT, Karpuzoglu E. Gender differences in cancer susceptibility: an inadequately addressed issue. Front Genet. 2012; 3:268. 22. Liu WC, Liu QY. Molecular mechanisms of gender disparity in hepatitis B virus-associated hepatocellular carcinoma. World J Gastroenterol. 2014; 20:6252–6261. 23. Humphries C. Sex differences: luck of the chromosomes. Nature. 2014; 516:S10–S11. 24. McGlynn KA, Hagberg K, Chen J, Braunlin M, Graubard BI, Suneja N, et al. Menopausal hormone therapy use and risk of primary liver cancer in the clinical practice research datalink. Int J Cancer. 2016; 138:2146–2153. 25. Hassan MM, Botrus G, Abdel-Wahab R, Wolff RA, Li D, Tweardy D, et al. Estrogen replacement reduces risk and increases survival times of women with hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2017; 15:1791–1799. 26. Irelli A, Sirufo MM, D’Ugo C, Ginaldi L, De Martinis M. Sex and gender influences on cancer immunotherapy response. Biomedicines. 2020; 8:232. 27. Ikeda M, Morizane C, Ueno M, Okusaka T, Ishii H, Furuse J. Chemotherapy for hepatocellular carcinoma: current status and future perspectives. Jpn J Clin Oncol. 2018; 48:103–114. 28. Liu M, Xu M, Tang T. Association between chemotherapy and prognostic factors of survival in hepatocellular carcinoma: a SEER population-based cohort study. Sci Rep. 2021; 11:23754. 29. Qayum K, Kar I, Rashid U, Nawaz G, Krishnakumar P, Sudarshan V, et al. Effects of surgery, chemotherapy, and radiation on hepatocellular carcinoma patients: a SEER-based study. Ann Med Surg (Lond). 2021; 69:102782.
留言 (0)