
記住我









WHO recommends that all pregnant women receive a standard dose of 30–60 mg iron and 400 μg folic acid as early as possible during pregnancy [6]. Ideally, women should receive IFA no later than the first trimester of pregnancy and take 180 tablets until delivery. In the current standard of care in Cambodia, pregnant women receive a total of 90 tablets of IFA supplements through ANC. This distribution is typically organized as follows: 60 tablets are provided during the first ANC visit, and an additional 30 tablets are given during the second ANC visit. Cambodia recommends four ANC visits during pregnancy, which also includes essential nutritional counseling and information about the importance of taking prenatal supplements.
The most recent Cambodia Demographic Health Survey (CDHS 2021–2022) does indicate that 86% of women had four or more ANC visits for their most recent live birth or stillbirth, and 98% of women took iron-containing supplements during their most recent pregnancy. Despite these figures, there is a data gap in knowing the actual adherence rates to the recommended 180 tablets of IFA, especially considering the government’s current distribution of only 90 IFA tablets. This underscores the importance of our study, as we seek to assess adherence and acceptability to 180 tablets of MMS as a potential alternative to IFA.
To date there are no published studies or documents from Cambodia on pregnant women’s acceptability of MMS or adherence to a 180-dosage regimen. A 2011 study in two provinces in Cambodia found access to ANC, the number of supplements provided, and ANC attendance were the strongest determinants for adherence to IFA supplementation [7]. Another assessement in Cambodia found the primary reasons for not adhering to 180 tablets of IFA during pregnancy were starting ANC after the first trimester and not attending all recommended four ANC visits [8]. In Nepal, Rai et al., found knowledge about preventable conditions and benefits, perceived barriers, social support, and perceived severity of not taking the supplement predicted IFA adherence [9] while Kulkarni et al. also found forgetting to take the supplements was a barrier [10]. In a study from Vietnam [11], determinants of adherence to either folic acid, IFA, or MMS were socioeconomic status, ethnicity, occupation, and parity, as well as increased contact with health workers. Acceptability studies which included MMS have identified organoleptic properties, perceived benefits, and fears or perceived negative effects as influential factors on acceptance and utilization [7, 12].
Assessment of the acceptability and feasibility of a new intervention should be done with end users prior to implementation, especially when the strategy requires possible changes in care processes. Determining the acceptability of MMS with pregnant women will enhance understanding of barriers to implementation and help to develop an MMS scale-up strategy that is feasible and cost-effective. Determining non-inferiority of adherence is also critical when introducing a new supplement.
In conclusion, the rationale for our study lies in the introduction of 180-tablets of MMS within ANC. To ensure successful implementation and scale-up of MMS, implementation research has been widely accepted as a necessary step [7]. This phase will involve testing product acceptability and adherence. Other planned studies include assessing enablers and barriers to MMS acceptability and adherence, product packaging and labeling, product marketing, health worker capacity building strategies, and strategic behavioral change communication strategies to promote daily use among Cambodian pregnant women. Furthermore, we need to address concerns expressed by host-country stakeholders regarding the potential impact on ANC attendance if MMS is provided in a larger quantity (i.e., 90 or 180 tablet bottles). Therefore, our study aims to bridge these knowledge gaps and inform the transition and scale-up of MMS in Cambodia’s ANC service delivery.
Intervention descriptionThe trial will include three intervention arms:
(1)IFA-90: Women in this arm will receive 60 tablets of IFA at the first ANC visit (ANC1) and 30 tablets of IFA at the second ANC visit (ANC2), as per current Cambodia's MoH guidelines
(2)MMS-90: Women in this arm will receive a total of 180 tablets of MMS, with 90 tablets distributed at ANC1 and 90 tablets distributed at ANC2
(3)MMS-180: Women in this arm will receive 180 tablets of MMS distributed at ANC1
The IFA tablet contains 60 mg elemental iron and 400 μg folic acid, while the MMS formulation was based on the UNIMMAP formulation [13] and contains 15 micronutrients: 30 mg elemental iron, 400 μg folic acid, 800 μg vitamin A, 200 IU vitamin D, 10 μg vitamin E, 70 mg vitamin C, 1.4 mg thiamin, 1.4 mg riboflavin, 18 mg niacin, 1.9 mg vitamin B6, 2.6 μg vitamin B12, 2 mg copper, 150 μg iodine, 65 μg selenium, and 15 mg zinc. The MMS tablets are available in either 90-tablet or 180-tablet bottles. Health centers (clusters) will be randomly assigned to one of the three arms.
Criteria for discontinuing or modifying allocated interventionsPregnant women enrolled in the trial who experience any reported adverse reactions in any of the trial arms will be referred to their midwife or doctor for guidance on whether to continue in the study or to withdraw. Participants are free to withdraw at anytime for any reason without consequence.
Strategies to improve adherence to interventionsANC and research staff will provide standard of care strategies to improve adherence to prenatal vitamins, such as counseling on the benefits of prenatal vitamins and how best to manage side-effects. The study aims to assess adherence of the interventions without influencing outcomes.
Relevant concomitant care permitted or prohibited during the trialIn the IFA-90 arm, pregnant women identified with anemia (Hb < 11 g/dL) during pregnancy will receive the Cambodia MoH’s standard of care, which includes provision of two IFA tablets per day and monitoring to assess if hemoglobin concentrations increase. Anemia is routinely tested for using the Hemocue at ANC1.
For the MMS-90 and MMS-180 trial arms, pregnant women with mild or moderate anemia (Hb 7.9– < 11.0 g/dL) will be referred to their midwife or doctor for guidance on the care and/or treatment of anemia during pregnancy.
Provision for post-trial carePost-trial care will follow the Cambodia MoH’s standard of care protocols for all enrolled participants.
Outcomes Primary OutcomeThe primary outcome is the non-inferiority of adherence rates (based on pill counts) of MMS-180 (180 days) compared to IFA-90 (90 days), using a non-inferiority margin of 15%. Adherence will be calculated based on the number of tablets consumed, divided by the total number of tablets the woman was eligible to take at the time of the final study visit.
Secondary Adherence OutcomesThe non-inferiority of adherence rates, (based on pill counts) of MMS-180 (180 days) compared to MMS-90 (180 days), using a non-inferiority margin of 15%.
The non-inferiority of adherence rates, (based on pill counts) of MMS-90 (90 days) compared to IFA-90 (90 days), using a non-inferiority margin of 15%.
Other Acceptability OutcomesThe overall acceptability of MMS as compared to IFA, assessed at the end-point of the trial (90 days for IFA-90 and MMS-90 and 180 days for MMS-180).
Adherence (%):The non-inferiority of adherence rates, (based on tablet counts) of MMS-180 (180 days) compared to MMS-90 (180 days), using a non-inferiority margin of 15%. MMS-1890 compared to IFA-90 at the trial's end-point will be measured. in terms of adherence rates. The non-inferiority of adherence rates, (based on pill counts) of MMS-90 (1890 days) compared to IFA-90 (90 days)MMS-180 to MMS-90 in terms of adherence rates. Other Acceptability Outcomes: The overall.
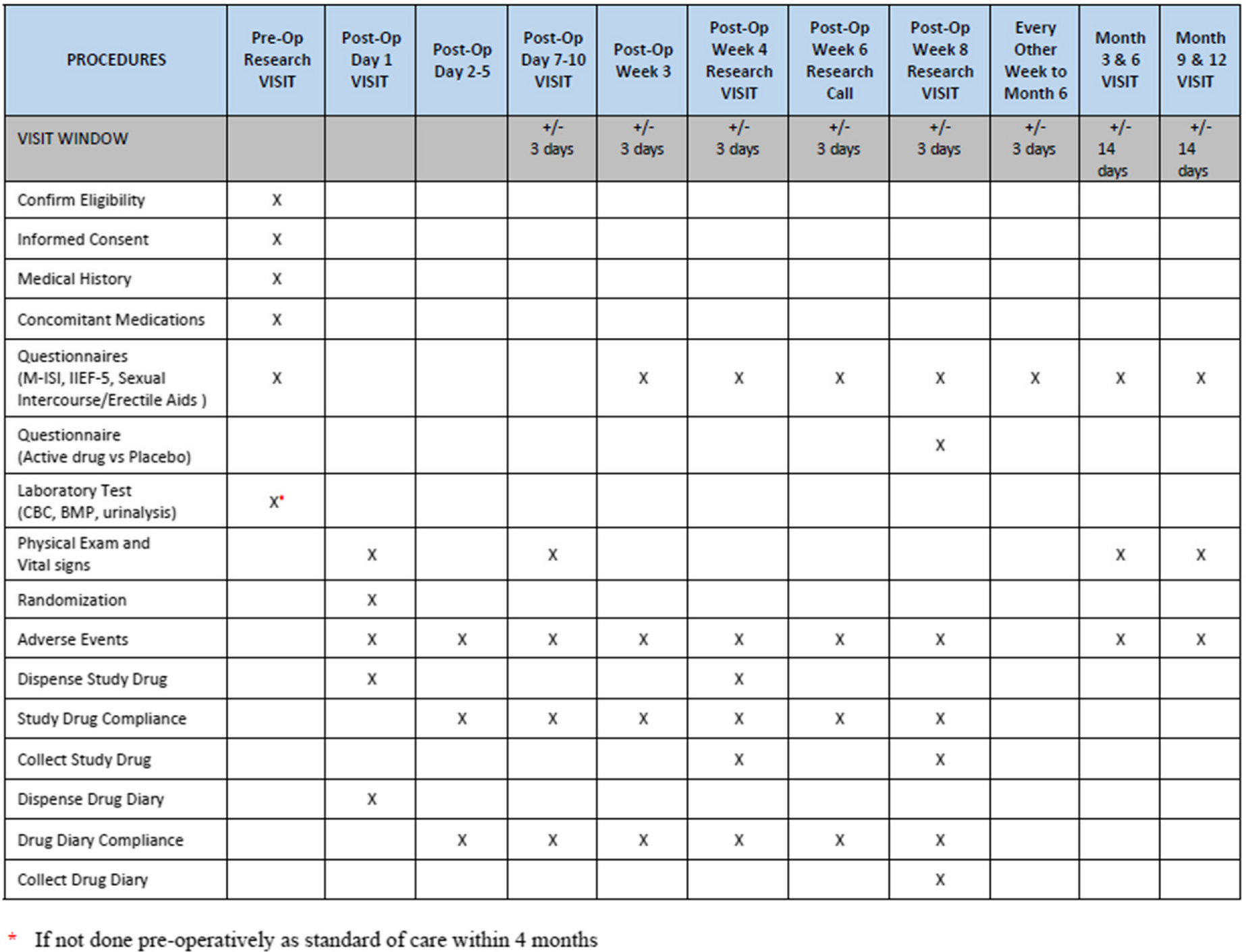
Participant timelineFigure 1 outlines the schedule of enrollment, interventions, and assessments.
Fig. 1
Schedule of enrolment, interventions, and assessments
t 1-ANC 1: Distribution of prenatal supplements for all three trial arms.
t 2− 30-day house visit: Acceptability survey questionnaire and adherence tablet count for IFA-90, MMS-90, and MMS-180.
t 3-ANC 2: Distribution of prenatal supplements for IFA-90 and MMS-90 groups.
t 4–90-day house visit: Acceptability survey questionnaire and tablet count for IFA-90, MMS-90, and MMS-180.
t 5–180-day house visit: Acceptability survey questionnaire, tablet count for MMS-90 and MMS-180 groups.
Sample sizeA sample of 1545 pregnant women is required for the statistical power determination for the adherence non-inferiority tests. Sample size estimations were calculated using adherence as both a binary and a continuous outcome. The more conservative sample size calculation for adherence as a binary outcome was chosen to ensure we were powered for both outcomes. The sample size was determined using a design effect of 2, twice as large as would be expected with simple random sampling. This accounts for the clustering within health centers (across 48 clusters) and the testing of three different arms. As the study arms are all within the same province and within three similar operational districts, large differences within clusters are not expected. Therefore, a design effect of 2 was deemede appropriate.
In addition, the sample size was calculated considering a 2-sided test, 90% power, an alpha of .025 for a one-sided confidence interval (CI), and a non-inferiority parameter of 15%. This sample size will allow for the detection of a significant difference in intake between the arms equal to 2% prevalence difference between arms (76% vs 74%) and a non-inferiority limit was determined ‘a priori’ as 15%. To compensate for a potential 10% loss to follow-up, a total of 515 women per arm will be recruited. Thus, the total sample size of pregnant women enrolled in the non-inferiority trial is 1545.
RecruitmentThe trial will randomly assign 48 government run health centers (clusters) from three Operational Districts to one of the three arms. Each arm will distribute a different supplement: IFA-90, MMS-90, or MMS-180. The MMS will only be given to enrolled trial participants.Pregnant women will be enrolled on a rolling basis in each health center. The enrollment process is anticipated to be completed within 3 months. Pregnant women will be enrolled on a rolling basis in each health center. The enrollment process is anticipated to be completed within 3 months.
Incentives for participant enrollment are not provided, but several strategies will be employed for ensuring sufficient cluster and participant enrollment. An orientation session for ANC providers (maternal and child health chiefs, midwives, and nurses) will be conducted to ensure a clear understanding of the study interventions and enrollment criteria. This session aims to equip health facility staff with the necessary knowledge and skills for effective enrollment of eligible participants.
Training sessions conducted by the research team to all health facility staff will emphasize the importance of prenatal vitamins in promoting a healthy pregnancy. Staff we will be encouraged to communicate this vital information to all participants across all study arms. This aims to raise awareness among pregnant women about the benefits of the study interventions, regardless of their assigned arm, and to underscore the significance of their participation.
留言 (0)