
記住我





Participants assigned to the control group will receive the GP’s usual care of adults (≥ 18 years) presenting with symptoms of an acute LRTI where the GP suspects CAP. Usual care will be used as a pragmatic comparator to reflect the current standard examinations and care of these patients in general practices in Denmark. Usual care is recommended to follow applicable guidelines from the Danish Society of General Practitioners (DSAM) [22] and Lægehåndbogen [The Doctor’s Handbook] [23]. FLUS is currently not a standard or even a common examination in Danish general practice. Even for GPs already using POCUS on a weekly basis, FLUS is not part of usual care for adults presenting with symptoms of an acute LRTI.
Intervention descriptionParticipants assigned to the intervention group will receive a FLUS examination during the index consultation (day 0) in addition to usual care.
Ultrasonography equipmentThe participating GPs use POCUS on a weekly basis before trial commencement and use the ultrasonography device already available to them. The type of device (classified as hand-held, laptop, or stationary), brand, model, and transducer used will be reported.
FLUS training programA pilot test of a FLUS training programme for GPs was performed in a prospective cohort study (ClinicalTrials.gov NCT04711031), after which the programme was adjusted to fit this trial. GPs who have not already participated in a FLUS training program with a validated assessment will complete this FLUS training program before trial commencement.
The FLUS training program consists of theoretical self-studying, a 1-day hands-on FLUS training course, and, subsequently, specialist-supervised scans. The theoretical part of the training programme consists of an estimated four-hour self-study based on e-learning material from Basal Klinisk Ultralydsdiagnostik [Basic Clinical Ultrasound Diagnostics] published by Munksgaard [24]. The self-study concludes with a validated theoretical multiple-choice question test with a pass/fail assessment [25], which must be passed prior to the FLUS hands-on training course.
The 1-day FLUS training course consists of an introduction followed by five hours of hands-on training on (1) healthy persons and (2) a simulator. The simulator resembles an ultrasound device and combines a mannequin torso with dynamic images when scanned. At the end of the day, each GP completes a simulation-based test, and a Lung Ultrasound-Objective Structured Assessment of Ultrasound Skills (LUS-OSAUS) score will be obtained for FLUS skills [26].
As part of the training programme, each GP is encouraged to perform five to ten FLUS examinations in their clinic within 1 month following the training course. FLUS specialists from Danish university hospitals (Department of Respiratory Medicine at Odense and Aarhus University Hospitals and Department of Cardiology, Section for Lung Transplantation, Rigshospitalet, Copenhagen University Hospital) supervise the GPs on the ultrasound images obtained from the examinations and their interpretation of findings. The LUS-OSAUS scores and number of supervised FLUS examinations will be reported for participating GPs.
14-zone FLUS scanning protocolThe FLUS scanning protocol used has been previously validated in hospital settings [27, 28] and recently also in a general practice setting [29]. Moreover, before trial commencement, the FLUS scanning protocol was pilot tested in a similar patient population in a prospective cohort study in general practice (ClinicalTrials.gov NCT04711031). The hemithorax is divided into anterior, lateral, and posterior surfaces. The anterior and lateral surfaces on each hemithorax are divided into upper and lower quadrants. The posterior surfaces on each hemithorax are divided into upper, middle, and lower quadrants. Each quadrant represents a scanning zone. The scanning zones on the patients’ left side can be denoted from 1 to 7L, and those on the right side can be denoted from 1 to 7R. Each scanning zone is assessed using FLUS. The transducer is placed in the middle of the scanning zone to create a cross-sectional image of the intercostal space and the underlying pleura blades. The positioning of the patient during the examination is decided by the GP and can be in an upright or a supine position or both. The GPs are trained in the 14-zone scanning approach during the FLUS training program.
FLUS pathological findingsFLUS pathological findings are predefined, and the GPs are trained in recognizing and defining possible pathological findings during the FLUS training program. The definitions of FLUS findings are based on the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) coursebook [30] and findings described in a similar patient population through a prospective cohort study in general practice (ClinicalTrials.gov NCT04711031).
B-lines: Laser-like vertical echogenic artefacts arising from the pleural line, spreading without fading to the edge of the screen and moving synchronously with lung sliding
Interstitial syndrome: Multiple (≥ 3) B-lines in at least 2 zones on each side present
Consolidation: Loss of aeration, which allows visualization of the lung parenchyma with sonomorphologic characteristics that resemble a solid organ or tissue. Pathognomonic for a pneumonic consolidation is the presence of air-bronchograms and serrated or blurred margins
Subpleural consolidation: Small subpleural consolidation between 2 and 20 mm in size that moves together with lung sliding
Pleural effusion: Anechoic or hypoechoic space between the visceral and parietal pleura
Focal visceral pleural pathology: Hypoechogenic thickening of the pleura with a rough appearance and interruption of the normally smooth pleura
Pneumothorax: Area without lung sliding, lung pulse or B-lines, with the presence of a lung point in an adjacent area
Other FLUS pathology: Other incidental findings by FLUS are described according to the ability of the GPs
Criteria for discontinuing or modifying allocated interventionsDue to the short intervention period during index consultation, the allocated intervention may only be discontinued for a given trial participant by the GP due to an unexpected event, hindering the GP from conducting or completing the allocated intervention, e.g. acute worsening of the participant’s condition during index consultation, after consent has been given and allocation has been revealed. Moreover, the study may be discontinued for a given trial participant upon participant request or by withdrawal of informed consent. The data collected before the discontinuation or withdrawal of consent will be retained and used in the analyses; however, no further data will be obtained from the participant.
Strategies to improve adherence to interventionsDuring the trial, participating GPs will be contacted by the PI at least twice a month to improve adherence to the intervention protocols.
Relevant concomitant care permitted or prohibited during the trialParticipants assigned to the control group are prohibited from having a FLUS performed by the GP during the index consultation. No further concomitant care or interventions are prohibited during the index consultation or during the follow-up period.
Provisions for post-trial careThe participating patients are covered by the Danish Patient Compensation Association, as the consultations are performed by GPs (authorized health care professionals). Participating GPs are covered by the Occupational Injuries Insurance Act [31].
Outcomes Primary outcomeThe primary outcome is the proportion of participants with antibiotics prescribed at the index consultation (day 0) reported by the GP at the index consultation. We will assess the effect of adding FLUS to usual care on antibiotics prescribed at the index consultation by investigating whether there is a difference between groups in the proportion of participants with antibiotics prescribed.
Secondary outcome 1)Outcomes from the LRTI symptom diary
Participants will be asked to complete a validated LRTI symptom diary every day from day 0 to day 21 [32]. The recorded items include the following six symptoms of LRTI: cough, dyspnoea, sputum production, well-being, sleep disturbance, and activity disturbance. The participants are asked to consider how bad each symptom has been over the past 24 h by scoring each symptom on a 7-point Likert scale (0 = no problem, 1 = very little problem, 2 = slight problem, 3 = moderate problem, 4 = bad problem, 5 = very bad problem, and 6 = as bad as it could be). Moreover, the diary contains a social domain on cancellation of work-related or leisure activities [33]. Only on the day of the index consultation (day 0) will the diary also include a question on participants’ satisfaction with the consultation, assessed on a 5-point Likert scale (very dissatisfied (1) to very satisfied (5)) [34]
1.1)Daily total LRTI symptom score, calculated as the sum of the scores for six symptoms (minimum 0 - maximum 36) (mean/median)
1.2)The number of days with symptoms rated as ‘moderate problem’ or worse by the participant (at least one item with a score of 3 or above) (mean/median)
1.3)Number of days participants signed in sick/cancelled work-related activities or cancelled leisure activities(mean/median)
1.4)Proportion of participants who were satisfied or very satisfied (4 or 5) with the index consultation
Outcomes 1.1, 1.2, and 1.3 from the LRTI symptom diary will be calculated for each participant every day from day 0 until the participant has scored 0 for every item, whichever comes first, or up to a maximum of 21 days [32].
2)Outcomes from participants’ shared medication records (i.e. FMK) and on type of prescription
As a standard care and communication method, data on changes in medicine or new prescriptions are automatically uploaded to the participants’ electronic shared medication record (FMK). We will review the participants’ shared medication records (FMK) for outcomes on antibiotics prescribed during follow-up in both groups:
2.1)Proportion of participants with antibiotics prescribed within 7 days after the index consultation
2.2)Proportion of participants with antibiotics prescribed within 28 days after the index consultation
If antibiotics are prescribed at the index consultation (day 0), the GP is asked to report whether the prescription is an immediate or delayed prescription (ref.).
2.3)Proportion of antibiotics prescribed as delayed antibiotic prescriptions at index consultation (day 0) [35, 36]
As a standard care and communication, GPs receive notices of health-related events, e.g. discharge and out-of-hour notices. From participants’ electronic medical records, we will obtain outcomes on the clinical course during follow-up in both groups:
3)Outcomes from participants’ electronic medical records
3.1)Proportion of participants with reconsultations, defined as any primary care contact (general practice or out-of-hour services), within 28 days after the index consultation
3.2)Proportion of participants admitted to the hospital within 28 days after the index consultation
3.3)Proportion of participants with complications (pleural infection (defined as complicated parapneumonic effusion or empyema), lung abscess, or sepsis) during admission to the hospital within 28 days after the index consultation
3.4)Proportion of participants with imaging other than FLUS (any imaging performed in secondary health care services) performed within 28 days after the index consultation
3.5)Other imaging methods performed within 28 days after the index consultation
3.6)Proportion of participants referred with suspicion of cancer within 60 days after the index consultation
3.7)Proportion of participants diagnosed with cancer within 60 days after the index consultation
3.8)Number of spontaneously reported unintended events up to 60 days after the index consultation
3.9)All-cause mortality up until day 28 and day 60
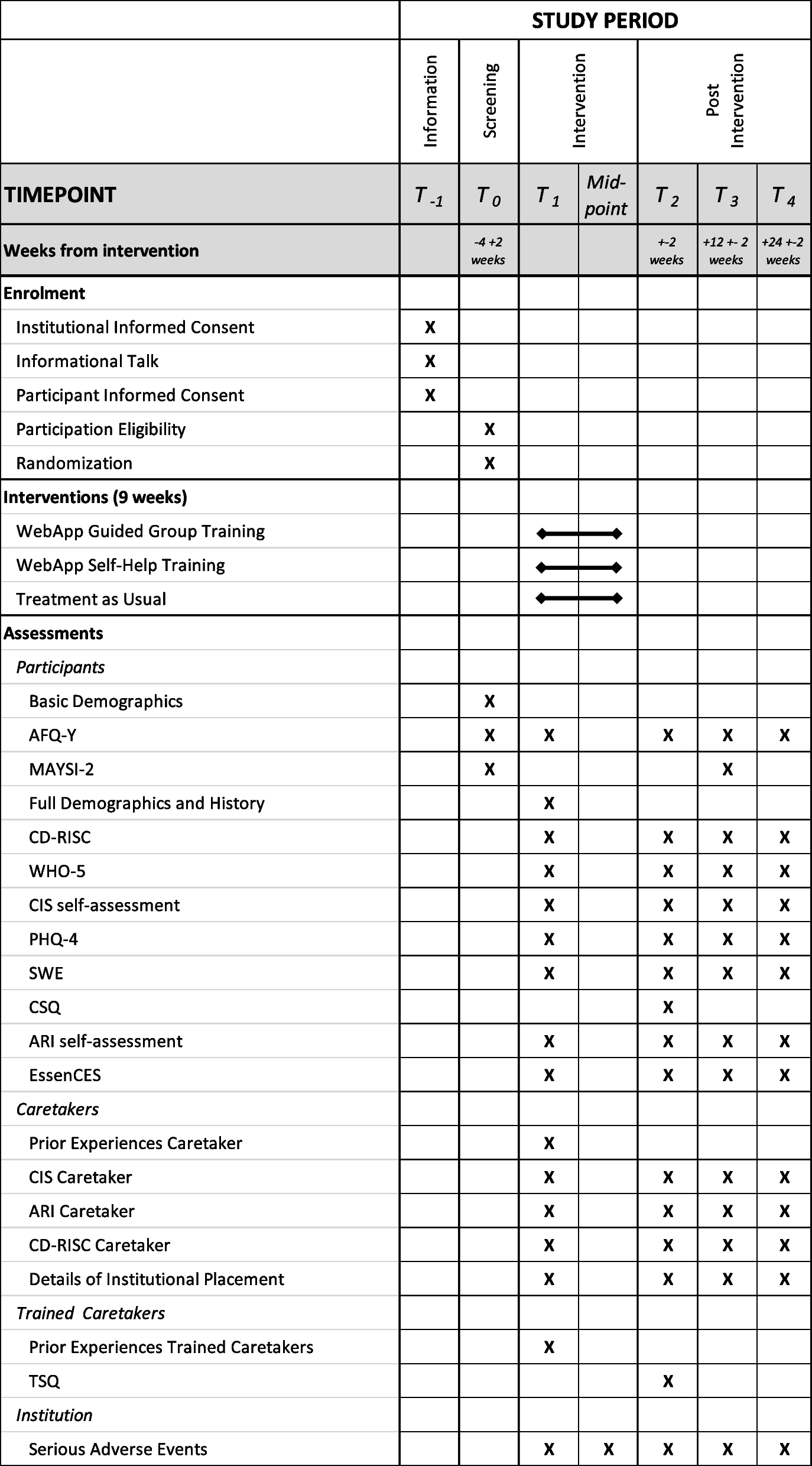
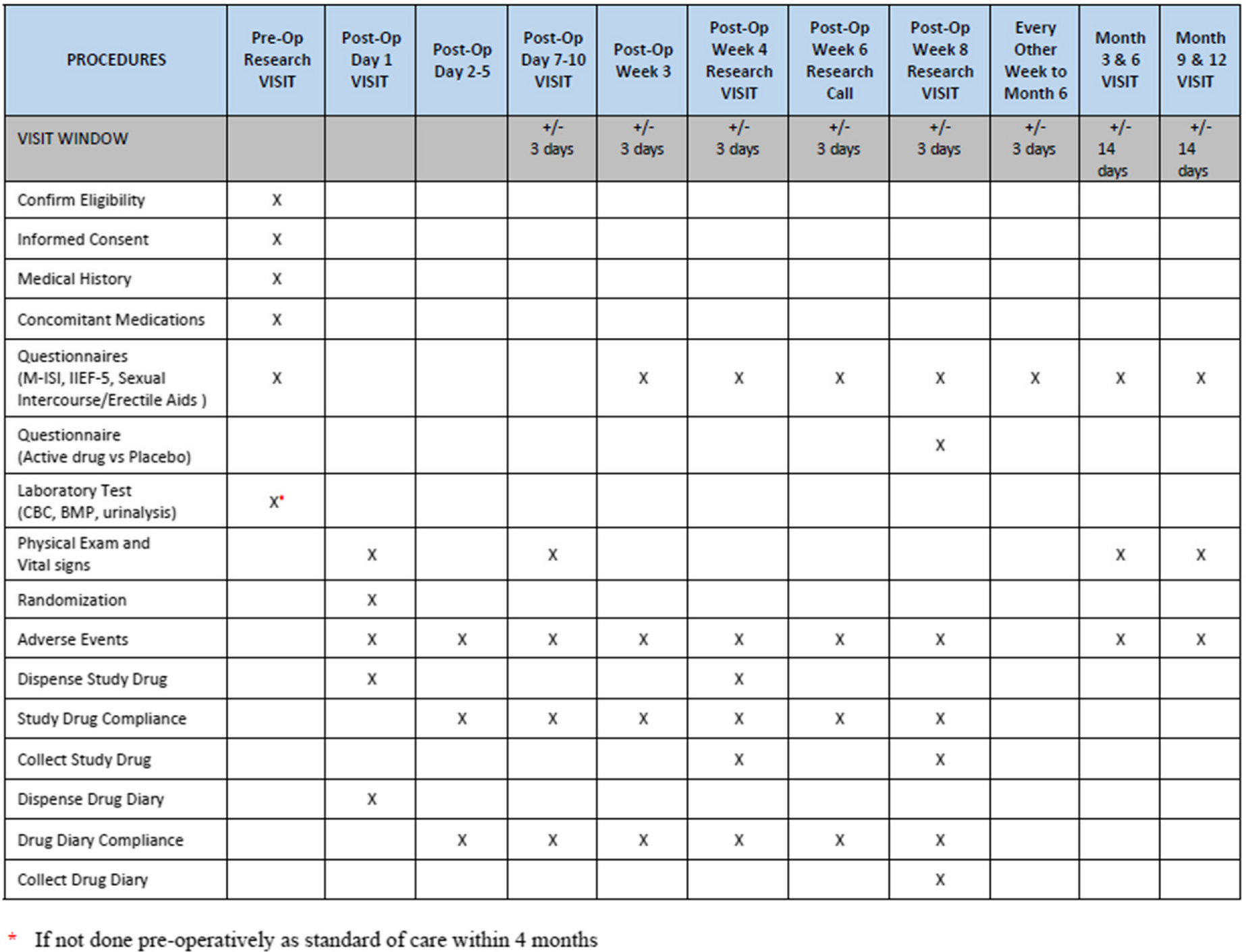
Participant timelineA diagram of the enrollment, allocation, intervention, and follow-up of the participants is shown in Fig. 1. Eligible participants are identified as they present to general practice. Once the GP identifies the patient as eligible for the study, information is provided, and informed consent will be signed as described earlier. Following consent, the GP will decide what diagnostics are necessary following the GP’s usual care of patients suggestible of having a bacterial CAP. The GP will complete an electronic case report form (e-CRF) for each participant recording information about symptoms and clinical findings and, if performed, point-of-care test (POCT) results, e.g. CRP. Randomization occurs once usual care has been performed and before possible treatment is prescribed. The GP will proceed directly to the phase of the consultation containing explanation and planning, with participants randomized to the control group before ending the index consultation. Participants randomized to the intervention group will receive a FLUS performed and interpreted by the GP before proceeding to explanation, planning, and ending the consultation. After the index consultation, during follow-up, it is of the discretion of the GP to reassess participants at any time if needed.
Fig. 1
Schedule of enrolment, interventions and assessment. Abbreviations: GP, general practitioner; FLUS, focused lung ultrasonography; e-CRF, electronic case report form; LRTI, lower respiratory tract infection; FMK, shared medication record
Sample sizeBased on previous quality improvement projects in general practice in Denmark [37], a Danish study by Holm et al. [8] and a Dutch study on reducing antibiotic prescribing in patients with LRTI [34], we assume to detect a 15% decrease in antibiotic prescribing in patients with LRTI from 50% (usual care) to 35% (+ FLUS). According to sample size calculations comparing these two proportions, a total of 340 patients with 170 trial participants in each arm were needed, using a 5% significance level and a power of 80%. We assume withdrawal or discontinuation by a maximum of 10% [38], furthermore, we increased the sample size by 5% to account for covariates in the analyses. Consequently, we plan to include a total of 390 trial participants (195 in each arm). Each GP is encouraged to include a minimum of 10 participants to account for the individual effect of FLUS on antibiotic prescribing at a GP level.
RecruitmentA total of 390 eligible patients will be enrolled by 30–40 GPs. A previous Danish study indicated that the incidence of patients suspected of having CAP when presenting to the GP is three to four patients on average per GP per month during the winter season [39]. Consequently, a study period of five months is expected to include 390 participants. The first participant was enrolled on November 3, 2023, and the enrolment period is envisaged to last until March 31, 2024. Enrollment is monitored by the PI, who contacts participating GPs at least twice a month to maintain recruitment and enrolment.
留言 (0)