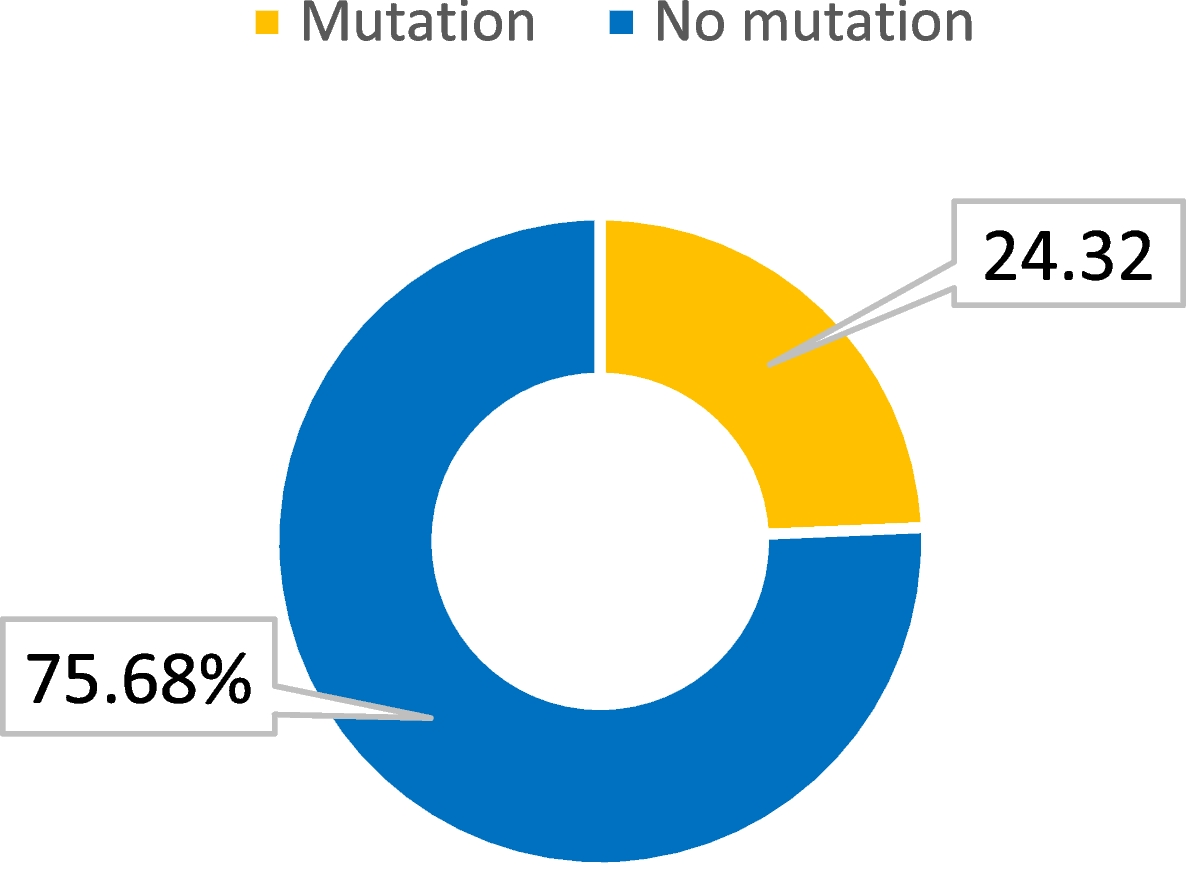
The current study represents a pioneering effort in utilizing an internationally accessible open-access database to investigate the radiological profile of de novo GBM. Due to the relatively low incidence of this disease compared to other metastatic cancers, comprehensive discussions on the subject pose challenges. The study population exhibited a slight male predominance, with a male-to-female ratio of 1.07:1, aligning with existing data from the United States [11]. The mean survival duration, regardless of the treatment protocol employed, was 347 (416.21) days, while the mean age of the subjects was 58.49 (11.39) years. The importance of evaluating the quality of life in these patients and establishing correlations with prognostic factors is underscored by the duration of survival [12, 13]. The majority (68.9%) of patients demonstrated wild-type IDH1 mutations, followed by cases categorized as NOS/NEC.
The mean survival days with SD for males and females were 553.8 (453.15) and 419.71 (368.13) days, respectively. Similarly, the mean survival days with SD for different GBM types were 475.1 (359.72) days for wild type, 427 (447.28) days for NOS/NEC, and 1265 (743.87) days for mutated. The raincloud plot in Fig. 1 provides a visual representation of these differences. It is worth noting that males tended to have a higher number of survival days compared to females, while patients with the mutated type had significantly higher survival days compared to those with wild type and NOS/NEC. However, it is important to consider that the mutated type comprised only two patients, with survival days of 1791 and 739 days, respectively. In a study conducted by Baid et al., a neural network was developed using MRI images, age, and tumor resection status to predict the survival days of GBM patients. The network achieved an accuracy of 70.2% in the training subset and 62.5% and 63.6% in the validation and testing subsets, respectively, with an overall accuracy of 73% for the entire dataset [14].
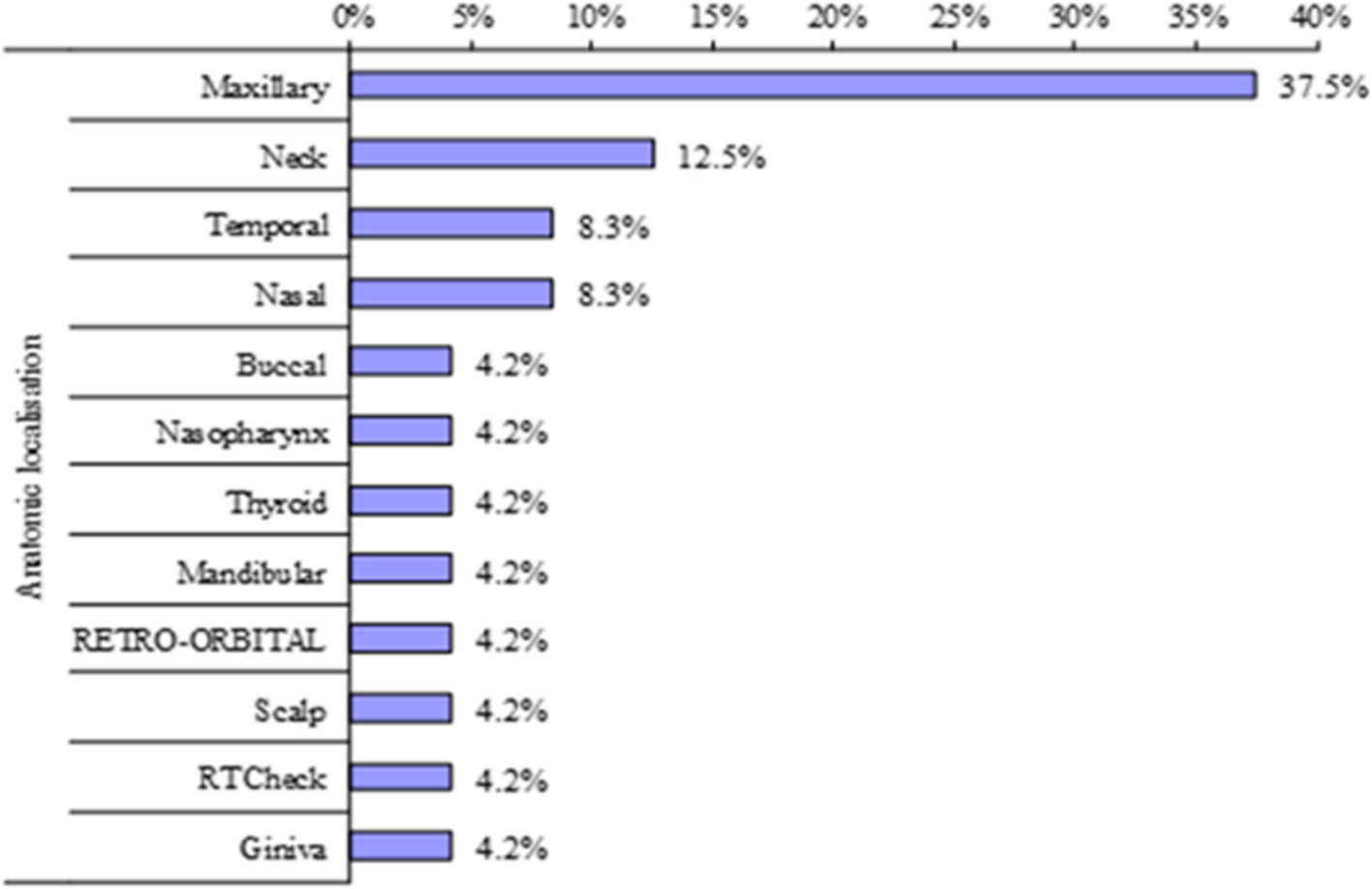
GBMs are typically found in the supratentorial region of the brain, which includes the frontal, temporal, parietal, and occipital lobes. Among these regions, the frontal lobe has the highest incidence of GBMs, followed by the temporal and parietal lobes, with tumors often overlapping multiple lobes. In the current study, the parietal lobe was the most commonly affected region, observed in 21 (36.2%) patients [15]. The dimensions of the tumor, including the anteroposterior (AP), transverse (TR), and craniocaudal (CC) measurements, were analyzed using z-scores to assess their significance. The z-score for AP was − 2.53 (p = 0.01), indicating a statistically significant difference from the mean. Similarly, the z-score for TR was − 3.89 (p < 0.001), indicating a highly significant difference. However, the CC dimension had a z-score of 1.53 (p = 0.12), indicating that the difference was not statistically significant at the specified significance level of 0.05.
Radiomics analysis of multi-parametric MRIs provides valuable information for radiologists in distinguishing between tumor progression and pseudoprogression. Ismail et al. achieved an impressive accuracy of 90.2% in this differentiation by combining T1 and T2/FLAIR images to create a 3D image for surface radiomics extraction [16]. They identified key factors such as the total curvature of the enhancing lesion and the curvature of the peritumoral hyperintense regions from T2/FLAIR images that aided in this distinction. The use of radiomics can significantly reduce the need for invasive biopsies as they contribute to the diagnosis and evaluation of treatment efficacy in patients. It is important to note that approximately 40% of glioblastomas do not respond to chemoradiotherapy and exhibit progression over 6–9 months [17]. Hypoxia, a critical pathway in neovascularization within GBM tumors, contributes to tumor resistance and leads to a poorer prognosis [18]. Beig et al. demonstrated that radiomics analysis can assess the extent of neovascularization and hypoxia before treatment, providing insights into survival prediction [19]. Figure 4 illustrates the impact of volumetric pixels and volumetric volume, two radiomic parameters, on survivability between males and females. These findings underscore the significance of considering different imaging protocols, including T1, T2, and FLAIR, when evaluating and analyzing radiomics in GBM patients.
Prasanna et al. conducted a study to assess the correlation between survivability and mass effect-induced deformation heterogeneity (MEDH) in glioma patients [20]. They found that the expression of MEDH in highly expressed multi-sequence MRIs had a significant impact on survivability, particularly when observed in areas associated with emotion, language comprehension, visual perception, social cognition, somatosensory, motor, and cognitive functions. This highlights the importance of considering the effects of tumor-induced deformation on various cognitive functions when evaluating prognosis in glioma patients. In addition, a review by Boele et al. delves into the psychological challenges faced by patients diagnosed with gliomas. The authors emphasize the impact of psychiatric disturbances, such as mood disorders and cognitive impairments, on patients’ quality of life. Effective management of behavioral changes and psychological symptoms related to tumors in cognitive regions is crucial and often requires appropriate psychotherapy interventions [21]. Chambers et al. have published research focusing on the implementation of psychotherapeutic approaches specifically tailored to address these challenges and improve the well-being of glioma patients [22]. Taken together, these studies highlight the significance of considering the impact of tumor-induced deformations and psychological factors on the prognosis and management of glioma patients. By comprehending and addressing these aspects, healthcare professionals can deliver holistic care that considers both the physical and psychological dimensions of the disease. These studies showcase the importance of assessing these factors within an Asian context, including regions such as the Middle East (encompassing Egypt, Saudi Arabia, and Turkey) and Asian countries like India, Pakistan, and China.
The current study has several limitations that should be acknowledged. Firstly, the study utilized a limited sample size, although it was larger compared to previous studies in the field. This limited sample size may affect the generalizability of the findings to the larger population. Additionally, the study did not correlate the radiological findings with histopathological or genetic findings, which could provide valuable insights into the underlying mechanisms of GBM. Although all patients were diagnosed with GBM based on histopathological assessment, the availability of data regarding specific histopathological and genetic characteristics was limited and not considered in the analysis. Another limitation is the lack of standardization in radiological protocols, including segmentation and image acquisition processes. This may lead to variations in the interpretation of radiological findings and limit the comparability of results across different studies or centers. It is important to consider these variations when interpreting the findings and applying them to real-world clinical scenarios. Despite these limitations, the study has its merits. The utilization of a third-party dataset helps minimize possible biases and enhances the generalizability of the study findings. By utilizing a diverse dataset, the study findings may provide valuable insights into the radiological profile of de novo GBM in real-world clinical settings. However, future studies with larger sample sizes, standardized protocols, and correlations with histopathological and genetic data would further strengthen the understanding of GBM and its radiological characteristics.







留言 (0)