
記住我
This randomized double-blinded placebo-controlled human intervention study covered a total duration of 8 weeks, including three parallel treatment arms (See Fig S1 supplementary data). The study consisted of an observation period of 4-weeks (week 1–4), which was similar for all treatment arms, followed by a 4-week intervention period (week 5–8). The observation period was added to assess the variation, without any treatment, for all outcome measures to be included as baseline [21, 22]. During the intervention period subjects received either a probiotic supplement, a fiber supplement, or a placebo supplement, to serve as control. Stratified randomization, using random numbers, ensured balanced allocation across treatment groups for BMI, age, and sex. An independent, unblinded scientist conducted the randomization and assignment to the treatment groups after enrollment. Successful randomization was confirmed by the balanced distribution of baseline characteristics between the three treatment groups (Table 1). Study subjects and investigators remained blinded until all analyses were completed.
The primary outcomes of this study were stool frequency, stool consistency and stool mass. Secondary outcomes, were IBS severity, constipation symptoms, anxiety and depression scores and QoL. Before the start of the study subjects were informed about all study procedures via an online information meeting. At the start and at the end of both study periods, subjects completed the validated questionnaires, consisting of irritable bowel severity scoring system (IBS-SSS) [23], the patient assessment of constipation symptoms (PAC-SYM) [24], the patient assessment of constipation Quality of Life questionnaire (PAC-QOL) [25], the Hospital anxiety and depression scale (HADS) [26], and the Food frequency questionnaire (FFQ) to measure their habitual dietary intake [27]. During both study periods, subjects also completed short daily questionnaires via ecological momentary assessment (EMA) application on their phone (LifeData LLC, Marion, IN, USA), which recalled stool frequency and consistency, GI-complaints, and supplement compliance. Stool consistency was a self-reported scale and scored on the Bristol Stool Scale (BSC), ranging from hard pellets (score 1) to watery diarrhea (score 7) [28]. In case of a stool frequency of > 1 stool per day, the BSC of the first stool was scored. The last 5 days of both the observation and intervention period, subjects were asked to collect and weigh all of their stools, in order to record a 5-day stool mass. To standardize this measurement subjects received a measurement scale and strict collection instructions. During the entire study, subjects were requested to maintain their normal routines concerning their diet and exercise patterns.
The study was performed from March until July 2021 in the Netherlands and was conducted in a corona-proof setting, completely at home and online. An online information meeting was organized prior to the start of the study, to explain all study procedures and measurements. Ethical approval for the NUTRIC study was obtained from the Medical Ethical Committee of Utrecht. The trial is registered at ClinicalTrials.gov (NCT04798417) and conducted according to the declaration of Helsinki. A digital written informed consent was obtained from each participant prior to inclusion in the study.
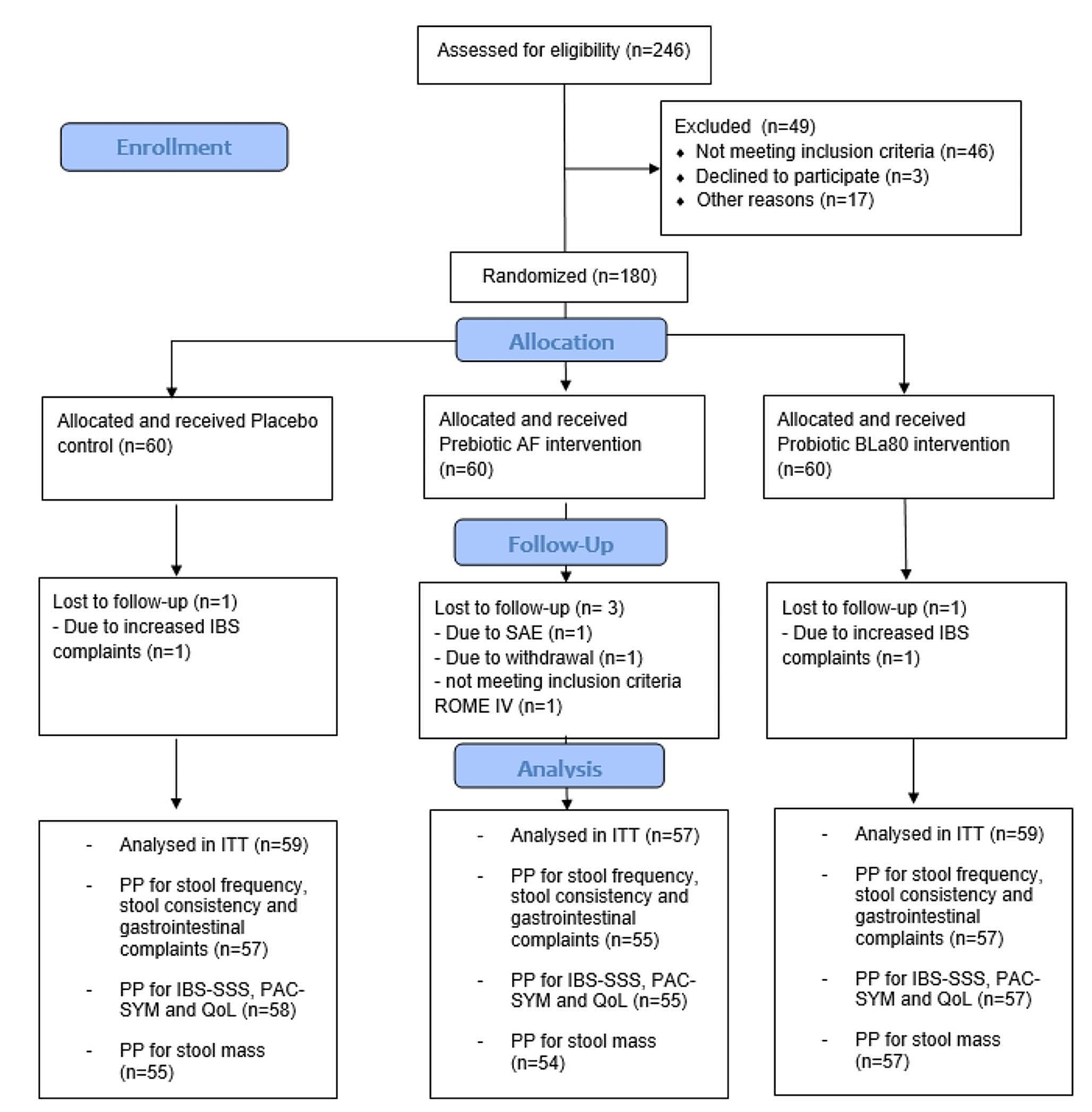
Study subjects and complianceWe aimed to include 180 subjects with IBS-C in the study. Subjects meeting the Rome IV criteria [29] for IBS with constipation, aged 18–70 with a BMI between 18.5 and 30 kg/m2, maintaining a stable dietary pattern, and owning a smartphone, were eligible for participation. Exclusions applied for those with certain chronic diseases or using specific medication or supplements that could influence the study outcomes (such as antibiotics, antidepressants, prebiotics or probiotics within 4 weeks before the study), recent intestinal surgery (except appendectomy/cholecystectomy) or endometriosis, pregnancy, breastfeeding, excessive alcohol use, smoking, or drugs/nitrous oxide consumption. Over-the-counter laxatives use was allowed, but had to remain constant during the study. A participant flowchart is shown in Fig. 1.
Supplement use and deviations from habitual diet and fluid intake were questioned daily via the Lifedata app. Using this self-reported data, a supplement compliance rate was calculated and deviations from the habitual dietary pattern were reported as protocol deviation. Subjects who dropped-out (n = 4) were excluded from the intention-to-treat (ITT) population. One additional subject was excluded from the ITT, as they did not meet all inclusion criteria for the ROME IV criteria at screening. Five others had major protocol deviations (due to medical reasons, medication, or supplement use), and were excluded from all per protocol (PP) analyses (n = 170). One participant with less than 75% daily questionnaire compliance was excluded from the PP analysis of the daily measurements (n = 169). Four participants with incomplete 5-day stool collection were excluded from the PP analysis on stool mass only (n = 166).
Fig. 1
Study participant flow chart. Flowchart of study subjects from recruitment and screening to final intention-to-treat (ITT) and per protocol (PP) data analyses
Intervention productsThe probiotic BLa80 supplement (Bifidobacterium animalis subsp. animalis BLa80, WeCare Probiotics Co., Ltd, Jiangsu, China) was mixed with 50% maltodextrin (Baolingbao Biology Co., Ltd, China, DE value 16% ≤ DE ≤ 20% as a delivery vehicle. The daily dose for this compound was 4 g/day (2 × 1011 CFU/g), divided in two sachets: one sachet (2 g/sachet) in the morning and one in the evening. The daily dose of the Acacia fiber (AF) supplement (Inavea™ Pure Acacia, Nexira, Rouen, France) was gradually increased from 5 g during the first five days to 10 g during the remainder of the intervention period, to prevent increase in GI complaints due to a sudden increase in daily fiber intake. The daily dose was also divided in two sachets: one sachet (5 g) in the morning and one sachet in the evening. The same gradual increase from 5 g to 10 g divided over two sachets was chosen for the placebo (control) supplement consisting of maltodextrin (WeCare biotechnology Co., Ltd, Jiangsu, China), which is a frequently used placebo compound in IBS trials [30]. For all supplements, the most effective and regularly consumed dosage was chosen in consolidation with literature and providers of the supplements. All supplements were consumed after mixing it with a small glass of orange juice, provided by the researchers. The packages and sachets of all supplements were identical, to ensure blinding. Supplements were commercially available products safe for human consumption.
Data analysesSample size was determined based on previous studies examining the effect of comparable prebiotic and probiotic supplements on stool frequency [31, 32]. Aiming to detect a difference of a stool frequency of 1.0 per week during the intervention period, assuming an SD of 1.5 in the mean stool frequency per week, using a power of 0.80 and a significance level of 0.05, and taking into account 2 drop-outs per group, a group size of 60 study subjects per arm was required. This resulted in 180 study subjects in total.
Statistical analyses and visualizations were performed using R statistics (RStudio, PBC, Version 4.0.2). Data show the PP analysis only. A p-value < 0.05 was considered statistically significant.
Data of daily questionnairesStool frequency, stool consistency, stool mass, and gastrointestinal complaints (bloating, abdominal pain, flatulence) were compared between the Acacia fiber, Probiotic BLa80 and placebo, and analyzed using linear mixed models (LMM) with restricted maximum likelihood estimation using lmer function (“lme4” package in R). Treatment group (Placebo / AF / Probiotic BLa80) and time (observation [day 1 to 28] / intervention [day 29–56]) were included in the model as main effects and as interaction effect (time*treatment group), subject was included as random effect. The aim was to compare each treatment with placebo, not to compare the AF and Bla80 treatments with each other.
To get more insight in the clinical relevance (e.g. an increase of more than 1 stool per week, considered clinically relevant [33]), delta values were computed. For stool frequency, average stools per week, per period, were calculated per individual and averaged per treatment group. For stool consistency, bloating, abdominal pain and flatulence the average value per day for observation and intervention period was calculated. Subsequently, the average values for the intervention period were subtracted by the average values of the observation period. One-Way ANOVA analysis followed by post-hoc testing with Bonferroni correction for multiple testing was performed on these period deltas.
Data of questionnaires at week 0, 4, 8Differences in total scores of IBS-SSS, PAC-SYM, PAC-QOL, and HADS scores and dietary intake (fiber, kjoule and water intake) were analyzed with LMM with restricted maximum likelihood estimation using Lmer function (lme4 package), with week (0 / 4 / 8) and supplement included as main factors and interaction effect (time*supplement), and subject as random effect. Week was included as factor to compare week 4 versus week 8 (change intervention) and week 0 versus week 4 (change observation).
To get more insight in the clinical relevance of the data, responder variables were computed. For the IBS-SSS score, a reduction of 50 score points after treatment was considered a clinically relevant change and applied as cut-off value to compute the responder variable on the IBS-SSS outcome (1 = responder, 0 = no responder) [34], while a reduction of 0.75 point for PAC-SYM and PAC-QOL scores after treatment was applied as a cut-off value to compute the responder variable for PAC-SYM (1 = responder, 0 = no responder) [35]. Responder analyses were performed with Pearson’s Chi-squared tests.
留言 (0)