Study participants and setting
The present study, as the first part (quantitative phase) of a sequential explanatory mixed-method study was conducted from January 2023 to September 2023. The permission was received from the Ethics Committee of Tabriz University of Medical Sciences (Ethical approval code: IR.TBZMED.REC.1401.211). To determine the psychometric characteristics of the Persian version of the MFKI and FFKI, two steps were used to validate and determine the psychometric properties of MFKI and FFKI. In the first stage, the translation of the tool and the pilot were done for content validity, face validity, and reliability evaluation. The second step was to evaluate the psychometric properties with a significant sample size to check the construct validity.
The psychometric evaluation of the scaleTranslation procedure
After acquiring permission from the main designers of the tool (Olekalns et al.) [14], the translation process was done based on the World Health Organization (WHO) guideline [18] and using the dual panel approach, and Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. In the first approach, the translation process was done in three stages [19]. The first panel consisted of a group of 10 expert panel include: Three expert in Midwifery, two expert in reproductive health, one clinical psychologist, one expert in Medical Surgical Nursing, two expert in Psychiatric Nursing and one expert in Community Health Nursing. The second panel (layman panel) consisted of 10 eligible women and their husbands. In the third stage (the target group panel), 1200 participants (600 women and their husbands) completed the questionnaire anonymously. The second approach occurred during five stages, including, Stage I: Initial Translation, Stage II: Synthesis of The Translations, Stage III: Back Translation, Stage IV: Expert Committee, Stage VI: Pretesting [20].
In the first step, the original version of the tool in the Farsi language was translated independently by two Farsi-speaking people who are fluent in English and experts in the field of tool preparation and childbearing. Then, the two translators compared their translated versions with each other, and after resolving the conflicts, they presented a final version. In the second step, to completely ensure the conformity of the Persian translation and the accuracy of the sentences of the Persian text, the final version created in the Persian language in the previous step was translated back into English by two people who had not seen the original version and were not involved in the translation process of the original version. Then, the two English backward and original versions were compared to check the transfer of the same concepts. Lastly, the translated questionnaire was given to 10 Iranian couples (10 qualified women and their husbands) for a preliminary evaluation of the comprehensibility of the questions and the simplicity of the concepts. Finally, based on the opinions of women and their husbands, changes were made in the Persian version regarding the fourth criterion, including Semantic Equivalence, Idiomatic Equivalence, Experiential Equivalence, and Conceptual Equivalence [21].
Content validity
To check the content validity, a qualitative method was used based on the evaluation of the expert committee, and a quantitative approach was used based on the calculation of the content validity ratio (CVR) and content validity index (CVI). In the qualitative method, the opinions of 10 experts were collected regarding the content, Persian language grammar, appropriateness with social-cultural characteristics, and adding new items, and then, based on their feedback, corrections were made, and the questionnaire was edited [22].
For quantitative evaluation, CVI was evaluated based on the content validity index of Waltz and Basel [23]. In this regard, questions were asked about each item's three criteria of relevance, clarity, and simplicity based on a four-point Likert scale, in which experts determined the degree of relevance, clarity, and simplicity. For example, the response options for simplicity were “1= not simple”, “2= somewhat simple, “3= simple” and “4= quite simple”. To this end, CVI scores were the sum of the 3 and 4 (highest possible) marks given by the experts to each item divided by the number of experts. Acceptance of items based on CVI score was higher than 0.79 [24]. Then, in the next step, to determine the CVR, questions were asked about the necessity of each item based on a three-point Likert scale (necessary, useful but unnecessary, unnecessary), and it was calculated using the formula \(CVR=\frac\). CVR > 0.78 confirmed the necessity of items [25].
Face validity
For face validity, quantitative and qualitative approaches were used. The quantitative approach was evaluated by calculating the impact score, and the qualitative approach was based on the opinions of the expert committee and target groups' views [26]. Questionnaire items in the face validity form include the first part (qualitative evaluation), checking in terms of difficulty levels, irrelevance, and ambiguity. The second part (quantitative evaluation) was included in calculating the impact score, checking the importance of the items based on a 5-point Likert scale (completely important, important, moderately important, slightly important, and not important). Then, the convenience sampling questionnaire was given to 10 eligible women and their husbands. Lastly, the score of each item was calculated using the following formula: Impact Score = Frequency (%) × Importance. Finally, the items with an impact score of more than 1.5 were accepted [27].
Construct validity (exploratory and confirmatory factor analysis)
For construct validity, a cross-sectional study was carried out on 1200 participants (600 women with their husbands) living in the northwestern region of Iran (Tabriz and Urmia health centers), via cluster random sampling. The samples size to perform construct validity in factor analysis is 5 to 10 for each item. Based on the rule of thumb, the sample size for exploratory factor analysis is classified as 50= very poor, 100= poor, 200= fair, 300= good, 500= very good and 1000= excellent [28]. The sample size in this study is equal to 1200 participant (600 women and 600 of their husbands) who were considered for exploratory and confirmatory factor analysis. To determine the sample size in this study, the sample size was calculated based on the results of Olekalns et al.'s study [14] about men's knowledge of fertility and considering Mean=8.86, SD=3.05, d=0.05 and Alpha=0.05 equal to 182 participant and about women's knowledge about fertility and with Considering Mean=10.35, SD=3.19, d=0.05 and Alpha=0.05, it was calculated equal to 146 participant. Due to the larger sample size calculated based on the knowledge of men and cluster sampling (Design effect = 1.5) and considering the 10% possible dropout, the final sample size was estimated to be 300 participant. Three hundred couples (300 women and 300 husbands) were examined in each city (Tabriz and Urmia).
In the present study, to do the sampling process, sampling was done in two centers of East Azerbaijan (Tabriz) and West Azerbaijan (Urmia). The cluster random sampling method was used for sampling in each province center. First, a quarter of the centers were randomly selected using the www.random.org website, then the researcher went to the chosen centers and extracted the list of women along with their telephone numbers from the SIB system (integrated health system), the number of women selected from each center was proportionally calculated concerning the sample size. The researcher made a phone call with the chosen women and, during the same phone call, checked the women and their husbands in terms of inclusion and exclusion criteria, and if they were eligible to enter the research, the researcher offered them information about the research, how to conduct it and the confidentiality of the information, and offered them to participate in the study. If the couples agreed to participate in the study, they were asked to be present at the health center with their husbands at a certain time. In the face-to-face visit, informed consent to participate in the research was obtained from the participants. The aims and methods of the study were fully explained to all eligible couples, and if they were willing to participate in the study, written informed consent was obtained from them. The questionnaires of socio-demographic characteristics, MFKI and FFKI were completed anonymously by the couples.
The inclusion criteria consisted of married women and men living in the northwestern region of Iran, being in reproductive age (women aged 18-49 and men aged 18-59), not having a history of primary infertility, women and men who have been married for more than a year and do not have children, and women and men who have passed more than three years since their last child. Couples having more than one child, widowed or divorced women and men, mental illness in each of the couples, taking antidepressants, including tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs), monoamine oxidase inhibitors (MAOIs), and noradrenaline (NA), stressful events such as divorce, death of first-degree family members, and diagnosis of an incurable disease for one of the family members during the last three months, and the presence of a specific or chronic illness such as cancer or heart and kidney diseases in each of the couples were excluded from the present study.
Measures
The two questionnaires used in this study included socio-demographic questionnaire, MFKI or FFKI.
Socio-demographic questionnaire
The socio-demographic questionnaire included information such as age, husband's age, marriage age, marriage duration, gravidity, number of abortions, type of childbirth, woman's education, occupation, monthly income adequacy, marital satisfaction, smoking status, exercise, contraception, assisted reproductive methods, husband's occupation, and husband's education.
Male and Female Fertility Knowledge Inventories (MFKI and FFKI)
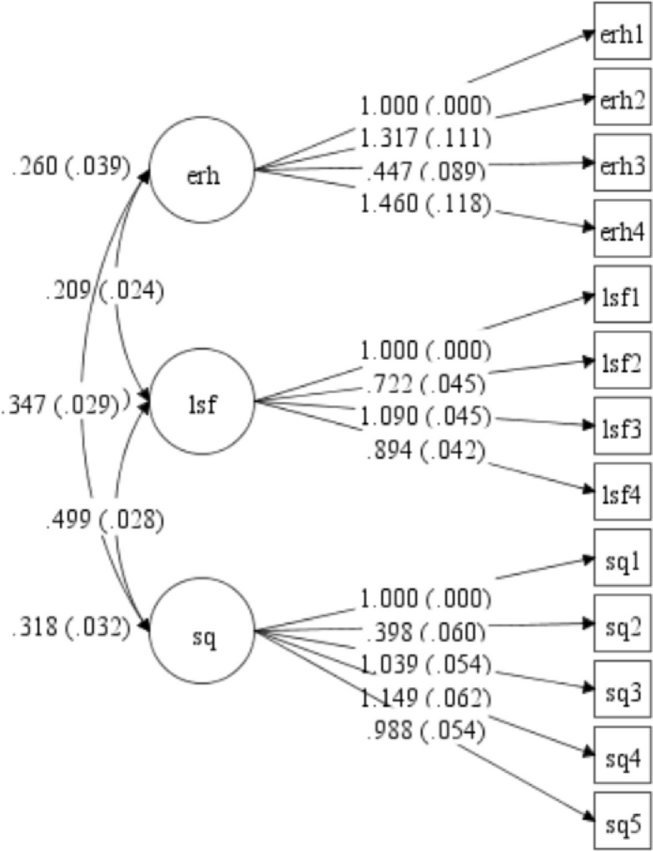
The Male and Female Fertility Knowledge Inventories (MFKI and FFKI) tools were designed separately by Olekalns et al. (2018) in Australia to measure men's and women's fertility knowledge. The MFKI tool is special for measuring men's knowledge of fertility, which has 14 items and three factors, including Environment and reproductive health (ERH) (5 items), Lifestyle factors (LSF) (4 items) and Sperm quality (SQ) (5 items). The FFKI tool is also special for measuring women's knowledge of fertility, which has 15 items and four factors, including Reproductive health (RH) (3 items), Lifestyle factors (LSF) (4 items), Chance of conception (CHC) (3 items) and Ovarian reserve and preservation (ORP) (5 items). In men and women, the tools are completed in the form of a three-point Likert scale (True, false, and I don't know). The true answer gets a score of 1, false, and I don't know choices are given zero scores. Higher scores indicate a higher knowledge of women and men regarding fertility. The validity and reliability of these tools have been proven in the Australian male and female population, respectively, with Cronbach's alpha coefficient of 0.78 and 0.77 [14].
Construct validity was examined using exploratory factor analysis (EFA), with Kaiser-Meyer Olkin (KMO) and Bartlett's test of Sphericity criteria. Then, the principal component analysis method with Varimax rotation (direct oblimin) was used to extract the factors. Likewise, the factor load value was considered above 0.3 [29]. In confirmatory factor analysis (CFA) using JASP 1.18 software, a series of indicators such as Root Mean Square Error of Approximation < 0.08, Standardized Root Mean Square Error of Approximation (SRMSEA) < 0.08, Normed Chi2 (x2 / df) < 5, comparative fit indices including comparative fit index (CFI > 0.90) and Tucker-Lewis Index (TLI) > 0.90, were used to check the suitability of the model [30, 31].
Reliability
Finally, to determine the reliability of the questionnaire, internal consistency and test-retest reliability were used [32, 33]. Internal consistency was checked by determining Cronbach's alpha and McDonald's omega coefficients for each factor and the whole tool. To assess the stability of retesting, the questionnaire was completed by 40 people (20 women and 20 men separately) via random sampling in two stages with a time interval of two weeks to determine the intra-class correlation coefficient (ICC). ICC between 0.6-0.8 was considered good, and above 0.8 as excellent. Similarly, Cronbach's alpha and McDonald's omega coefficients above 0.7 were satisfactory [34].
Ethical considerations
The Ethics Committee of Tabriz University of Medical Sciences approved the current study (Ethical approval code: IR.TBZMED.REC.1401.211). After getting the required permission from the main designers of the tool (Olekalns et al.), written informed consent was obtained from all participants. All couples were given full explanations about the process and objectives of the study, confidentiality of information, preservation of privacy, and freedom to withdraw at each stage of the study. This study was done based on the World Medical Association of Helsinki declaration.
Statistical analysis
In the current study, SPSS Statistics 14 (IBM Corp, Armonk, NY, USA), STATA 14 (Statcorp, college station, Texas, USA) and R software 4.2 (Psych package) were used for data analysis. To describe socio-demographic characteristics, data were presented as mean (SD) and frequencies (%) for quantitative and qualitative variables, respectively. Content and face validity (CVR and CVI, Impact score), EFA, and CFA were also determined for construct validity. The reliability of the tool was also calculated through Cronbach's alpha coefficient, McDonald's omega and ICC.






留言 (0)