Characterized for the first time in 2009, the DICER1 syndrome is a multi-tumor condition caused by germline pathogenetic variants in the DICER1 gene and associated with different neoplastic lesions affecting the lungs, thyroid gland, ovaries, and kidney [7]. For the syndrome to occur, typically, a loss-of-function variant, resulting in the inactivation of the affected DICER1 allele, and a second “hotspot” pathogenetic mutation affecting the RNase IIIb domain of DICER1 are required [12].
Patients with DICER1 syndrome, typically in pediatric or adolescent age, face an increased risk of developing a variety of thyroid lesions, spanning from TFND to malignant thyroid tumors [29,30,31]. Even though this syndrome is important to recognize, it should be stressed that somatic DICER1 aberrations in thyroid nodules are likely to be more prevalent than germline mutations [17]. Given the rather widespread occurrence of these somatic mutations in thyroid nodules, there is a significant clinical need to ascertain the clinical relevance and extent of these alterations, as well as whether the finding of these alterations would require germline testing to rule out syndromic disease [19, 21, 32, 33]. Moreover, as the detection rate of DICER1 mutations in thyroid tumors will rise as more pathology centers rely on next-generation sequencing, identifying potential genotype–phenotype correlations is crucial, especially for centers that require specific conditions for case submission for sequencing.
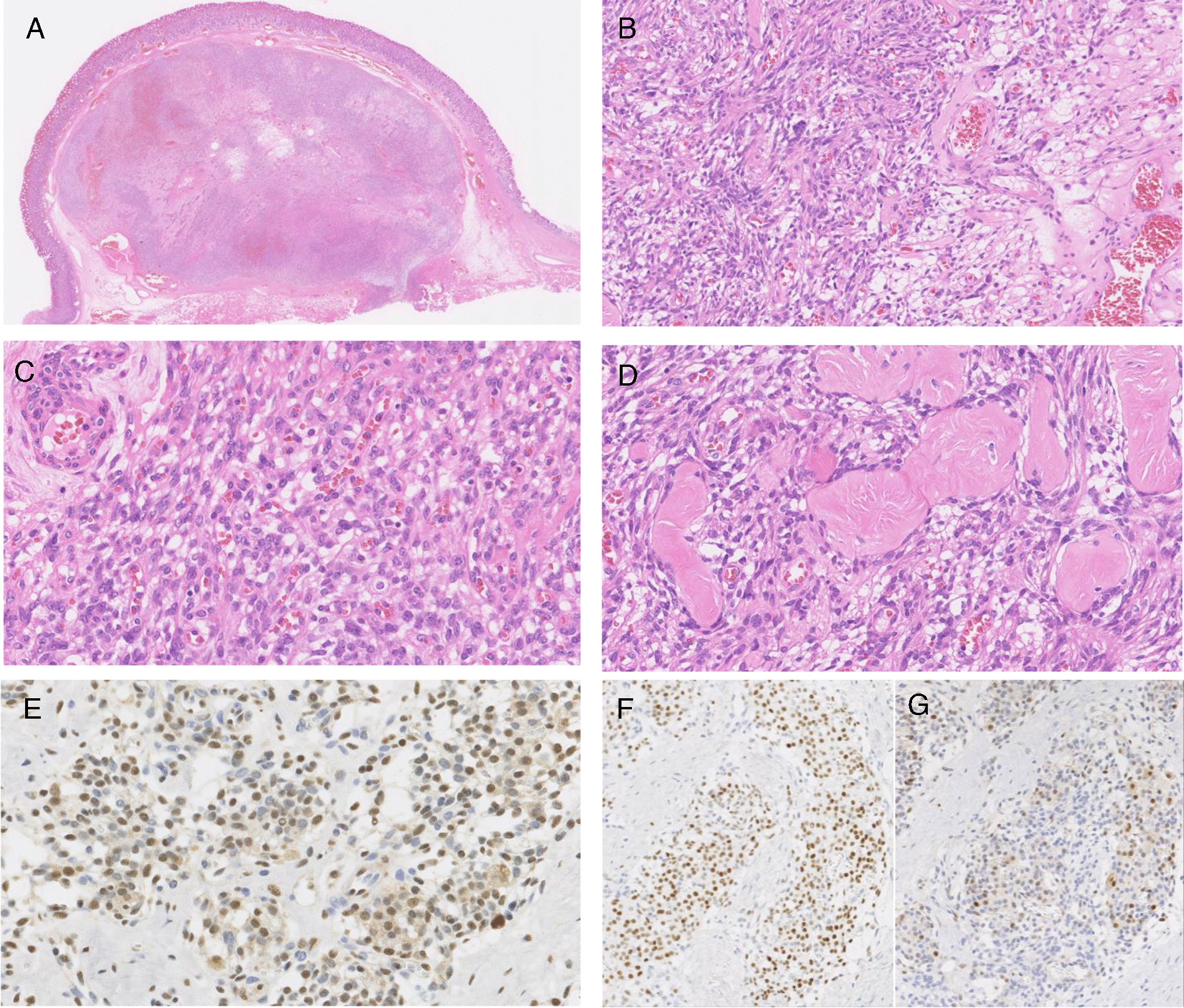
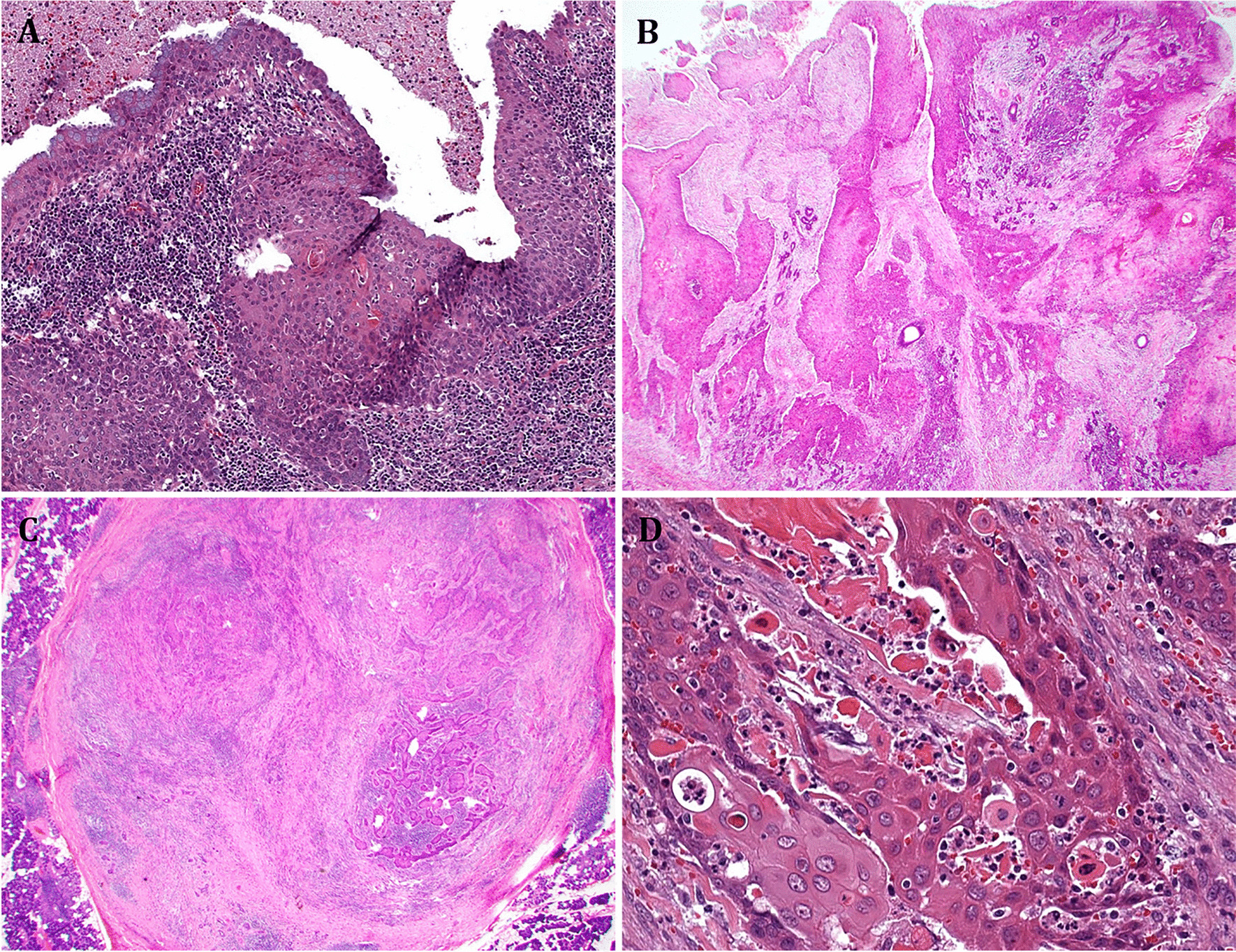
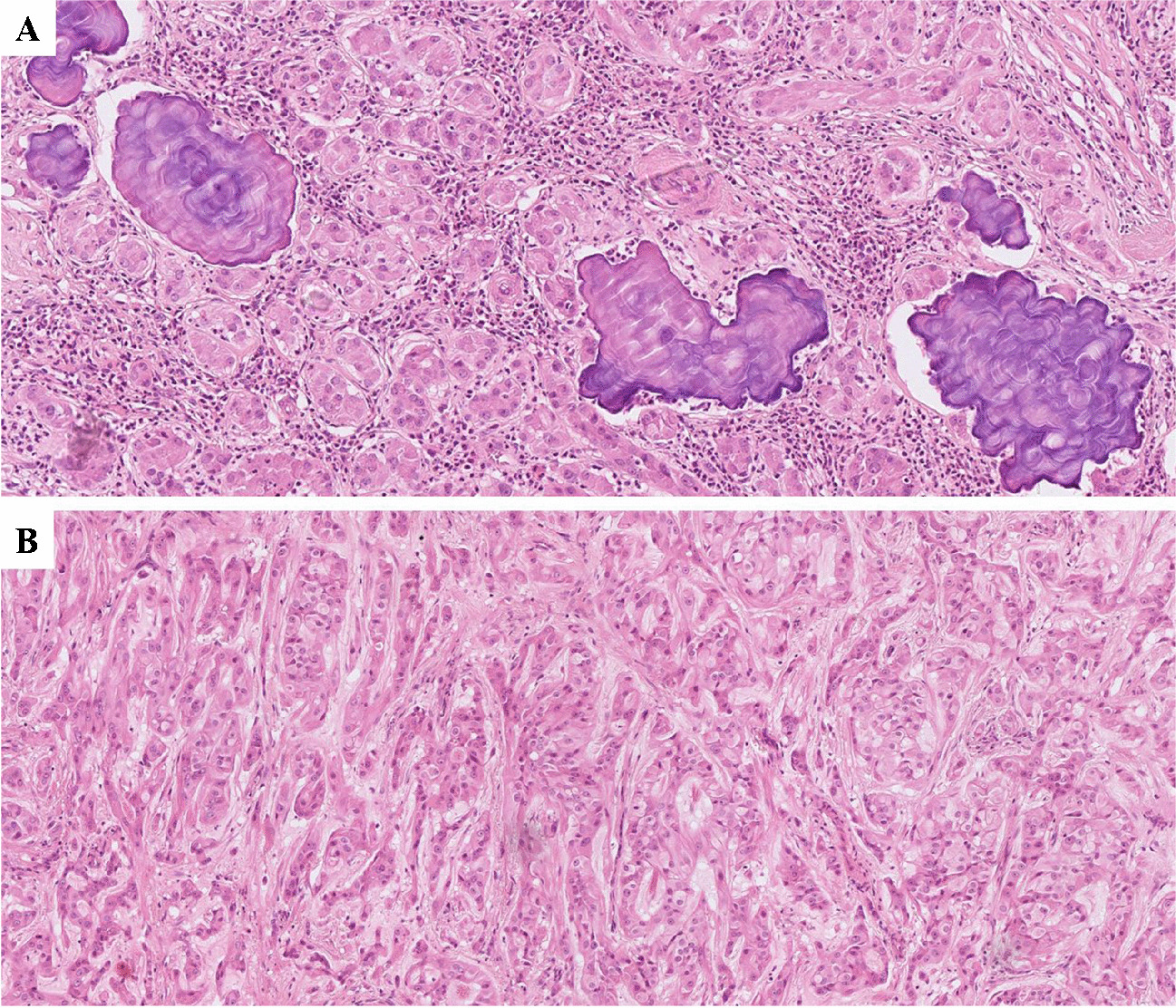
In this study, we gathered molecular, histopathological, and clinical data from thyroid tumors at two distinct institutions (European and North American) to examine whether our initial observations regarding a genotype–phenotype correlation remain consistent in larger cohorts obtained from diverse centers. Our investigation affirms that specific histological features, such as macrofollicular growth and atrophic changes distinctly correlate with the presence of DICER1 mutation in follicular-patterned thyroid tumors, corroborating the previously assumed association between macrofollicular variants of follicular thyroid tumors and inactivating somatic DICER1 mutations reported in previous studies [26, 27, 34, 35]
Interestingly, the identification of atrophic areas seems to be strongly associated with this genetic aberrancy, as only 2 out of 35 DICER1 wildtype cases with RAS mutations exhibited such areas. It is not known if atrophic changes are unique to follicular cell-derived thyroid tumors or if they are also visualized in unrelated thyroid tumors with DICER1 mutations, for example, thyroblastoma [36, 37]. Upon reviewing the current literature, we did not observe such an association. However, future research investigating the potential role of atrophic changes in this tumor type would indeed be of interest in order to increase our understanding of this phenomenon.
Moreover, while atrophic changes have not yet been described on the cytological level, there are reports suggesting that macrofollicular structures and papillary excrescences may also be detected in fine needle aspirates of DICER1-mutated thyroid nodules [38]. Further studies in cytological preparations could possibly help delineate important clues already at the preoperative level. The specific mechanism underlying the atrophic changes is not known, but one might speculate that the aberrant micro-RNA expression patterns conferred by the DICER1 mutations potentially instigate an atrophic state. Indeed, several micro-RNAs have been associated with thyrocyte maturation and differentiation [39]. Moreover, DICER1 deficiency in the retinal pigment epithelium has been associated with oxidative stress and geographic atrophy, and DICER1 knock-out mice develop prostate atrophy [40, 41].
The DICER1-mutated cohort from Karolinska was assembled via NGS analysis, specifically targeting cases that exhibited specific epidemiologic and/or histologic criteria. By screening only those lesions meeting specific criteria, the percentage of positive cases—indicating patients with the aforementioned mutation—comprises > 50% of the total material. This should be compared to observations made in a large, unselected material of > 400 TFND and follicular-patterned tumors in which the DICER1 hotspot mutational frequency was approximately 3% [25]. This underscores our demonstration that employing specific criteria can substantially elevate the proportion of patients with detected DICER1 mutation in clinical practice.
In the present study, not all patients underwent analysis for mutations in constitutional tissue. Additionally, prior research indicates that most of these mutations are somatic [19, 20]. The critical question, therefore, revolves around the significance of detecting such a genetic aberration in clinical routine. Presumably, this approach allows pathologists to guide cases to surgeons for further clinical genetic management. Although the majority of patients may test negative for constitutional mutations, identifying individuals with syndromic forms of the disease holds substantial clinical value, justifying meticulous genetic mapping. Nevertheless, firm conclusions in this regard necessitate larger studies with available constitutional data.
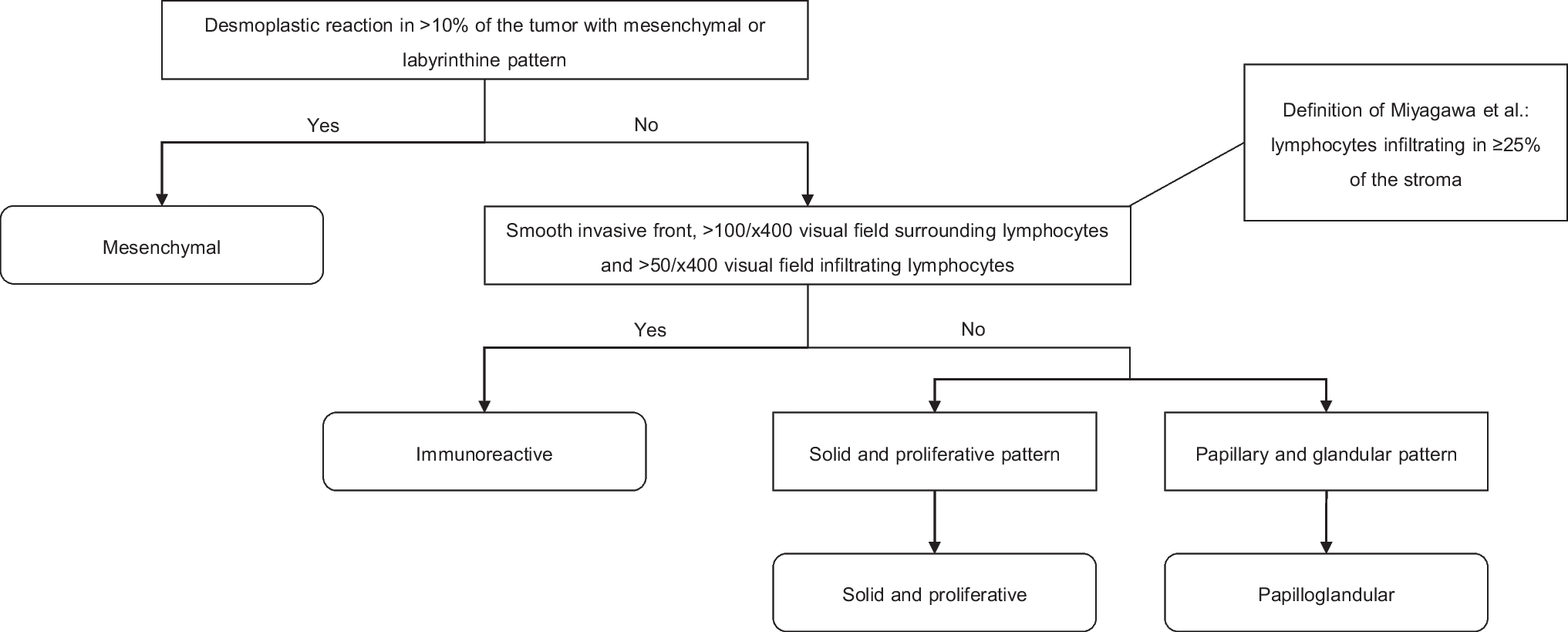
To summarize, based on morphological and histological characteristics, we suggest an algorithm that could be used to predict DICER1 mutations in follicular-patterned thyroid tumors a priori. In particular, specific features such as macrofollicular growth and atrophic changes appear to be strongly coupled to DICER1 mutations in follicular-pattern thyroid tumors. Potentially, these histological attributes, together with young age, may display a specific and unique combination that could be of clinical interest, allowing pathologists to categorize cases for genetic testing based on histological findings.





留言 (0)