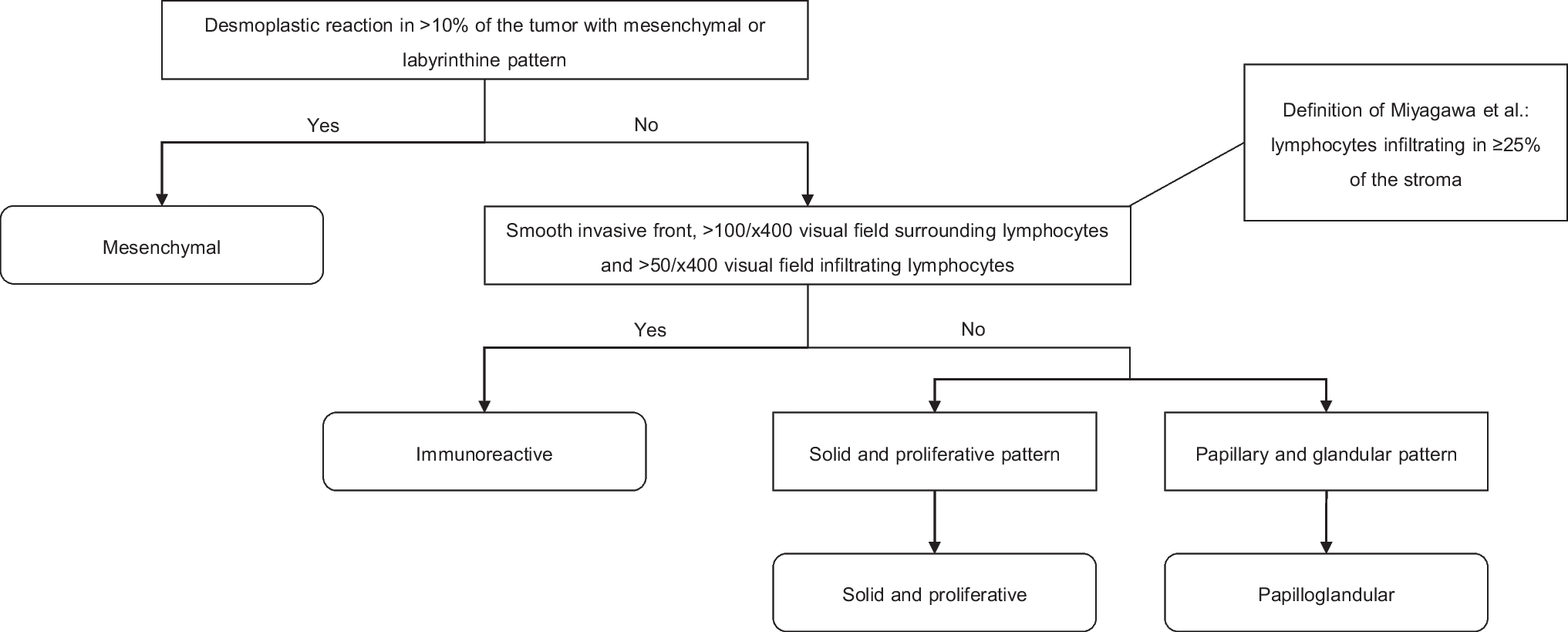
In this study, we classified 208 HGSOC cases into mesenchymal, immunoreactive, solid and proliferative, or papilloglandular subtypes, based on histopathological criteria established by Murakami et al. and Miyagawa et al. [13, 14]. We observed only a fair interobserver agreement for each method. Importantly, no differences in 5-year progression-free and overall survival rates were observed between the subtypes, irrespective of the classification method employed. Consequently, subtyping HGSOC based on the currently available histopathological classification methods offers no clear advantage in clinical practice.
To make well-informed treatment decisions based on the predicted prognosis and treatment response of the histological subtypes, it is crucial that these subtypes are consistent and reproducible. In the study of Murakami et al. (2016), six observers classified the cases, resulting in an average concordance rate of 74% (range: 61–89%, average Cohen’s κ = 0.65, range: 0.46–0.85), a rate they regarded as suboptimal for use in clinical practice [13]. In their subsequent study by Miyagawa et al. (2023), the application of the Murakami et al. criteria yielded a Fleiss’ κ of 0.348 between four observers. After refining the definitions of the mesenchymal, solid and proliferative, and papilloglandular subtypes, and adjusting the definition of the immunoreactive subtype due to challenges in observing cellular details on WSI, the coefficient increased to 0.549 [14]. In our study, two specialized gynecological pathologists reached a 62.5% concordance rate (Cohen’s κ = 0.34), utilizing the refined criteria of Miyagawa et al., except for the immunoreactive subtype, which was based on the criteria of Murakami et al. It was not possible to calculate Cohen’s κ for the cases classified using Miyagawa et al. criteria due to reclassification of tumors jointly classified as immunoreactive, solid and proliferative, or papilloglandular under the Murakami et al. criteria. However, using the immunoreactive definition of Miyagawa et al. likely has a limited influence on the determined Cohen’s κ, as only 13 out of 86 cases changed subtype. We argue that this reproducibility rate is not robust enough for clinical utilization in individual patients [16, 17].
The observed low concordance rate in subtype classification may be the underlying reason for the absence of differences in PFS and OS between the subtypes in our study. To minimize misclassification, each case was rigorously reviewed by two specialized gynecological pathologists. However, a possible overrepresentation of the mesenchymal subtype was observed, with 122 of 208 cases (58.7%) being classified as mesenchymal. This contrasts with the 36% in the study of Murakami et al., and 44% in the study of Miyagawa et al. [13, 14]. Cohen’s κ for distinguishing mesenchymal versus non-mesenchymal subtype was 0.352 (69.2% concordance rate) in our study. In comparison, the study of Murakami et al. reported a Cohen’s κ of 0.70 (85% concordance rate), while the study of Miyagawa et al. reported a Fleiss’ κ of 0.703. This difference might contribute to the contrasting survival outcomes for the mesenchymal subtype, as this study could not replicate the lower OS rate for the mesenchymal subtype observed in the study of Murakami et al. Moreover, Murakami et al. reported a higher PFS and OS rate for the immunoreactive subtype compared to the other subtypes. Our study showed a similar, although not statistically significant, trend. A potential explanation for this might be the limited number of cases we classified as immunoreactive using Murakami et al. criteria (n = 10, 4.8%). Using the revised definition of Miyagawa et al., this number increased to 23 (11%). However, this did not lead to differences in survival outcomes.
Khashaba et al. (2022) also investigated the correlation between histopathological subtypes of HGSOC and survival outcomes [18]. However, their classification algorithm differed from that of Murakami et al., encompassing variations in both the histopathological subtypes and the criteria used for the classification [13, 18]. Cases featuring a cellular stromal reaction in > 10% of tumor tissue were classified as mesenchymal. All other cases with a mitotic count of > 30/10 high power fields were classified as proliferative. Cases showing a lower mitotic count, but > 20 lymphocytes infiltrating tumor nests per high power field, were categorized as immunoreactive. The remaining cases were categorized as differentiated, and further divided into those with solid endometrioid transitional (SET) or (micro)papillary features [18]. These criteria were derived from different studies and were not compared with the gene expression-based subtypes [13, 19,20,21]. Therefore, we did not apply this classification method to our cohort. Nevertheless, Khashaba et al. identified the histopathological subtype as a significant factor for PFS (p = 0.008) in a univariate analysis, although no significant correlation was found with OS. The mesenchymal subtype demonstrated the shortest median PFS, whereas the differentiated subtype with SET features exhibited the longest median PFS. Additionally, primary debulking surgery, compared to interval debulking surgery, and administration of paclitaxel and carboplatin chemotherapy, compared to other chemotherapeutic agents, also showed correlation with a better PFS (p = 0.004 and p = 0.001, respectively) [18]. However, multivariate analysis on PFS was not conducted, probably due to the small sample size of the study (n = 85). Consequently, the correlation between the histopathological subtype based on the criteria of Khashaba et al. and PFS remains uncertain [18].
Research has also indicated that treatment responses might vary among the subtypes. Specifically, the mesenchymal subtype has been reported to have the most favorable response to taxane-based chemotherapy and potentially to dose-dense chemotherapy as well [11, 13]. Furthermore, bevacizumab is thought to be more efficacious in the mesenchymal and proliferative subtypes [12, 14, 22]. However, since the standard treatment regimen for our patients included carboplatin and paclitaxel, without the addition of bevacizumab, our study could not explore these potential differential responses to therapy.
One of the strengths of our study is that all cases were independently reviewed by two gynecological pathologists. In instances of discordance, a joint review was undertaken, ensuring consistent and accurate subtype classification. While the initial agreement between pathologists was relatively low, consensus was eventually reached for all cases. Furthermore, subtyping was performed by the same two pathologists for both classification systems. This approach effectively eliminated variance between classification systems that might arise from discrepancies in individual pathologist evaluations.
A limitation of our study was that we did not perform RNA sequencing. Consequently, we could not validate whether the subtypes, as identified by the two gynecological pathologists, aligned with those determined by gene expression analysis. In the study of Murakami et al., concordance between the gene expression-based subtypes and histopathological subtypes was examined but limited to a subset of samples (n = 59). They observed agreement in approximately 70% of the cases, showing a significant association between the subtypes (p < 0.001) [13]. However, given the observed low concordance rate between pathologists in our study, there is a clear need for more straightforward subtyping criteria, particularly for the mesenchymal subtype, as the presence of this subtype may impact the choice of treatment [11,12,13,14, 22]. Future investigations should prioritize refining these criteria to improve interobserver consistency, and subsequently examine survival outcomes.
We suggest further exploration of the application of artificial intelligence (AI) or machine learning. The feasibility of histotype classification using machine learning has already been demonstrated [23]. For HGSOC subtyping, AI or machine learning could support the refinement of HGSOC subtype criteria by identifying novel or alternative histopathological features. Moreover, these computational approaches may have the capacity to determine HGSOC subtypes autonomously. However, to facilitate such research, high-quality RNA-sequencing data is necessary, considering the current challenges in achieving adequate reproducibility rates for histopathological subtypes. Once AI or machine learning is refined through training with robust data, it could play an important role in subtyping HGSOC, enhancing diagnostic precision, and informing treatment strategies.
In conclusion, the current histopathological subtypes of HGSOC as defined by Murakami et al. and Miyagawa et al. demonstrate only fair reproducibility. Furthermore, in our cohort of 208 HGSOC patients, no differences in overall and progression-free survival between the subtypes were observed. As such, the implementation of these subtypes in clinical practice remains premature. Further research is warranted to establish criteria that are more straightforward and to investigate their association with survival outcomes.





留言 (0)