
記住我




In total, 75 BM biopsies were stained for CCN2 by the 10095S antibody, of which 55 MPN cases (10 × ET, 10 × post-ET MF, 10 × PV, 10 × p-PV MF, 5 × pre-PMF, 10 × PMF) and 20 control cases with normal marrow. The control group encompassed 15 males and 5 females, with a median age of 63.5 years (range 44–77 years). The MPN group encompassed 32 males and 23 females, with a median age of 60 years (range 16–77 years), being not significantly different from the control group. In the MPN group, 39 cases (71%) contained a JAK2 V617F mutation, 12 cases (22%) a CALR mutation, 2 cases (4%) an MPL mutation, 1 case (2%) was triple negative, and in 1 case, the driver mutation could not be determined due to insufficient DNA quality.
CCN2 expressionWhen stained for CCN2 by the 10095S antibody, the BM biopsies showed a variable degree of cytoplasmic staining of the megakaryocytes, while the myeloid and erythroid cell lineages were negative. The megakaryocytes showed variable staining, both within and between biopsies. The intensity of staining was scored semi-quantitatively on a scale from 0 to 3 (0 = no staining, 1 = weak staining, 2 = moderate staining, 3 = strong staining) as illustrated by Fig. 2. There was no extracellular staining, which is remarkable as CCN2 is generally considered to be an extracellular protein. Throughout the literature, this appears to be a consistent finding for CCN2 staining, also in other tissues [17, 18], and it was confirmed with 2 additional independent antibodies in the present study. Possible explanations for this finding have thus far largely remained speculative.
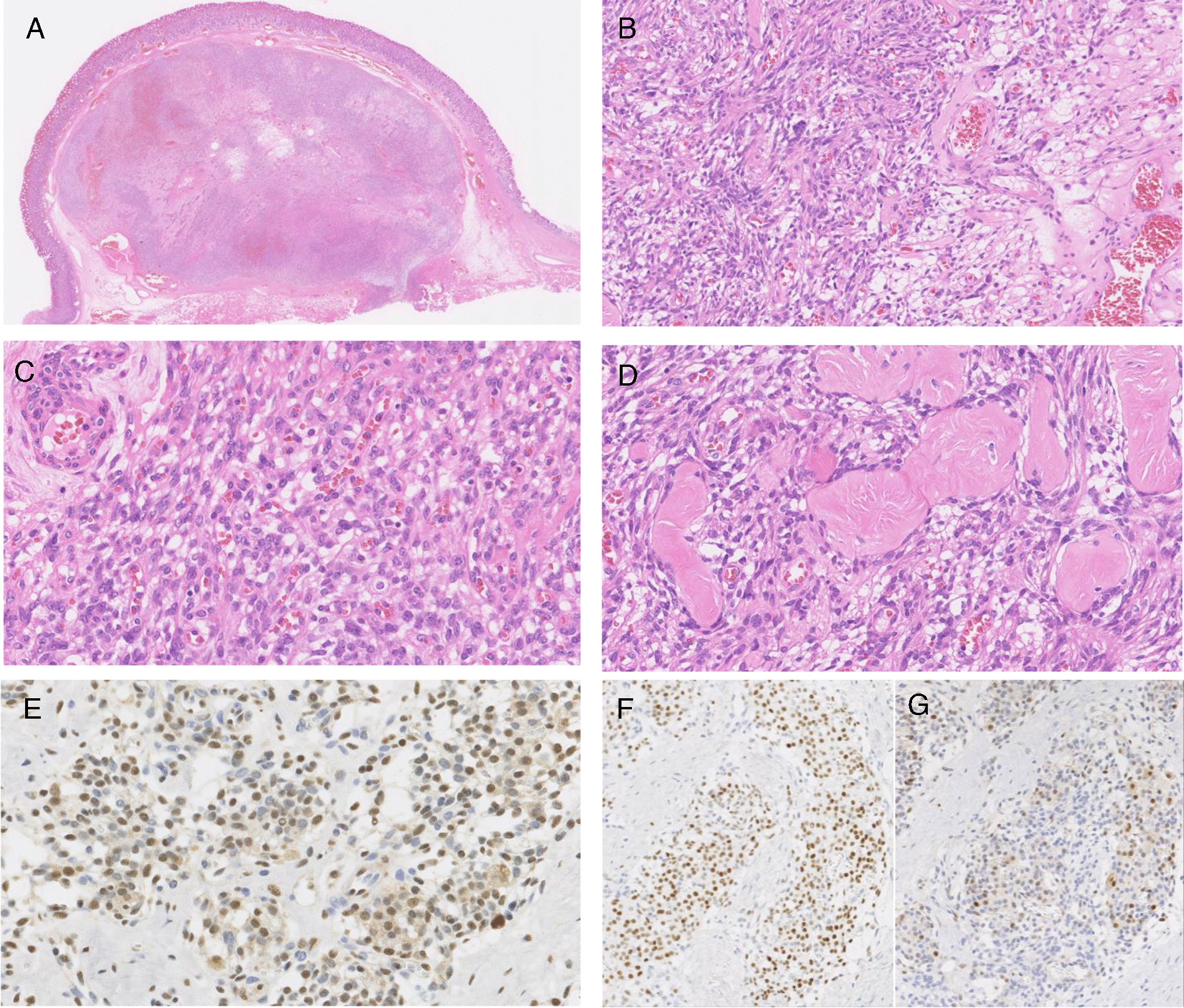
Fig. 2
CCN2 scoring of megakaryocytes. Megakaryocytes stained for CCN2 demonstrating a no staining (score: 0), b weak staining (score: 1 +), c moderate staining (score: 2 +), and d strong staining (score: 3 +)
In normal BM, the majority (96–100%) of megakaryocytes in the biopsy showed no or weak staining as illustrated in Fig. 3a. A small number of megakaryocytes (up to 4%) within each biopsy displayed moderate or strong staining, with strongly staining megakaryocytes accounting for at most 2% of the total number of megakaryocytes. The CCN2 expression score ranged from 0.05 to 1.26 with a median score of 0.62.
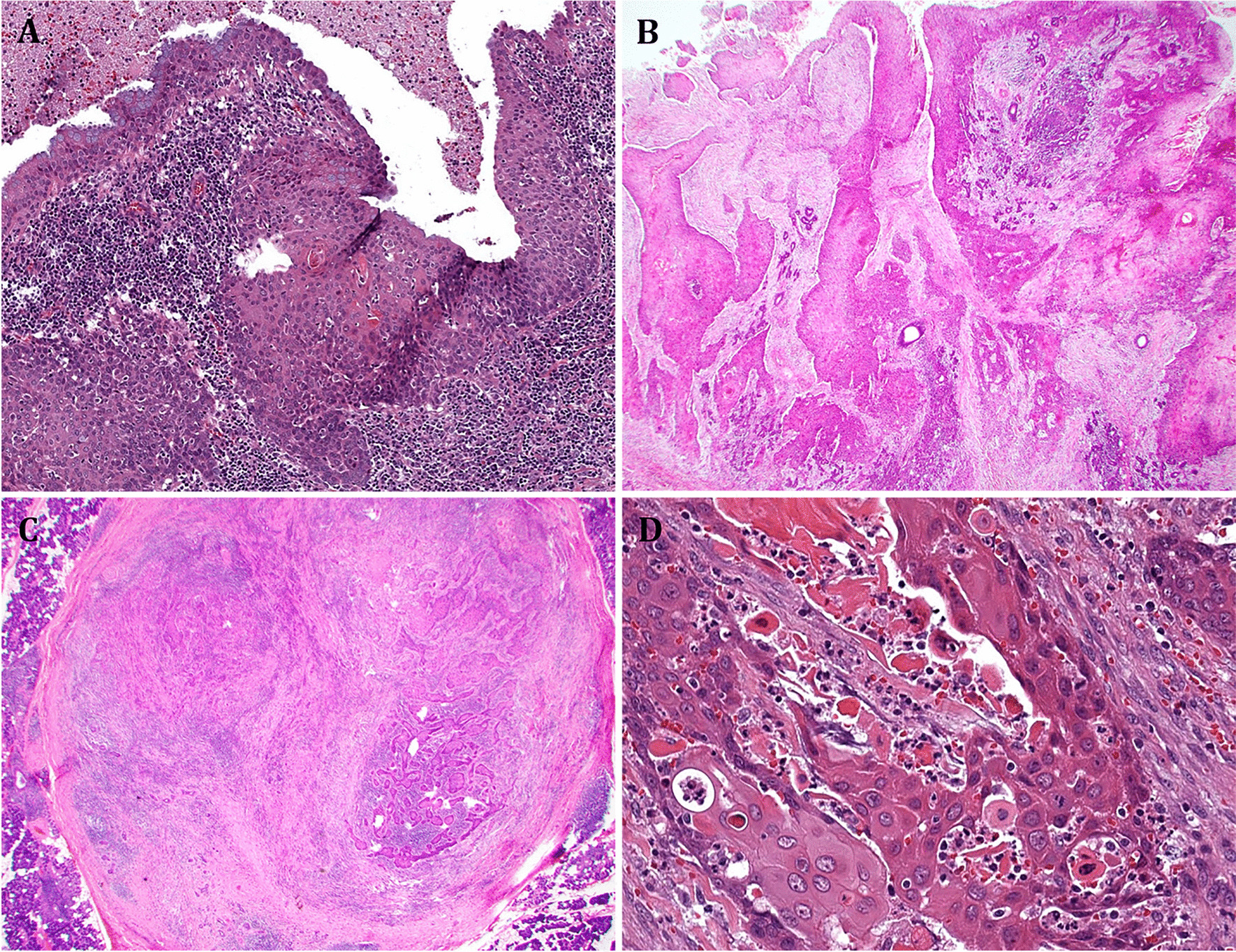
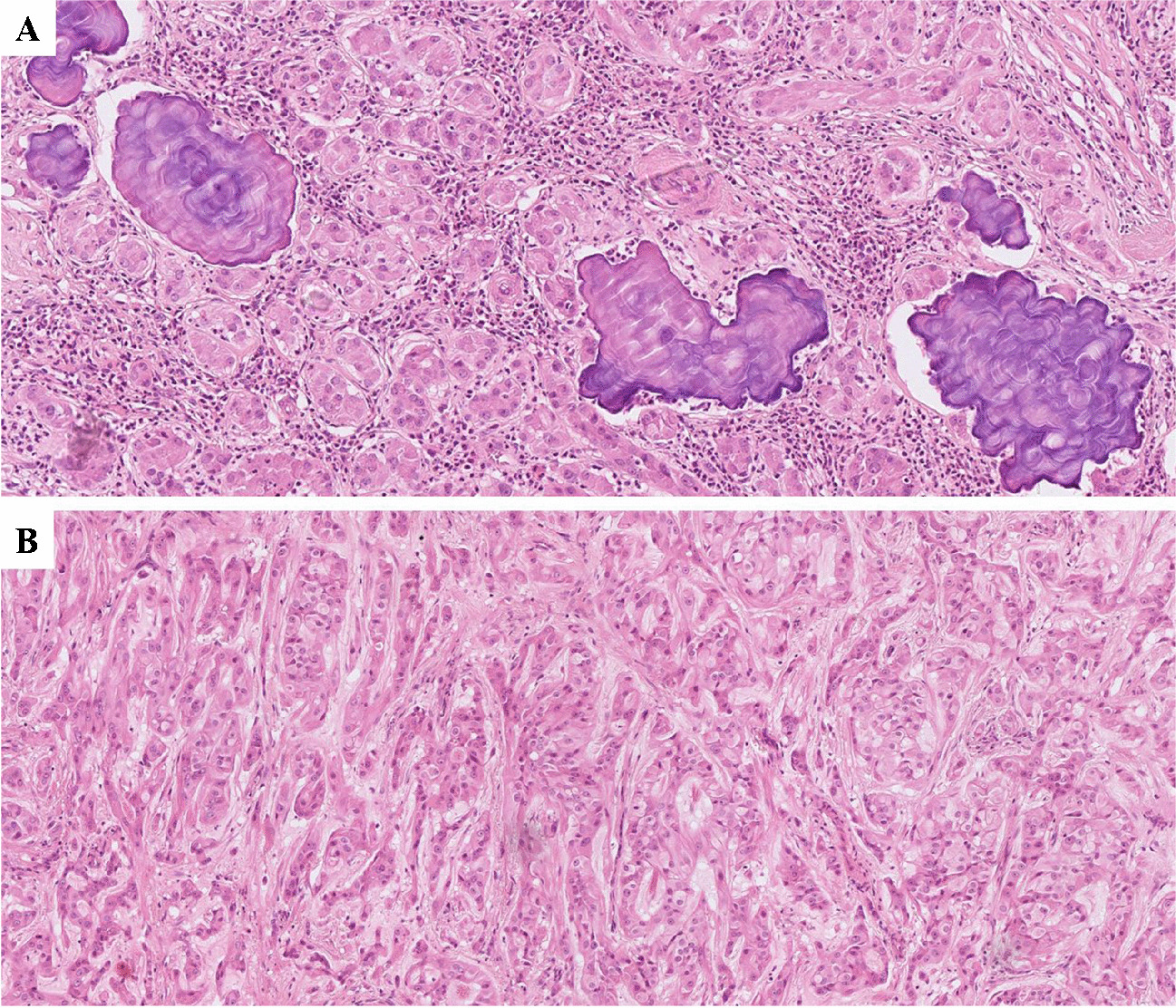
Fig. 3
CCN2 immunohistochemical staining of bone marrow biopsies. a Normal bone marrow, in which megakaryocytes show no or only weak staining, with only rare megakaryocytes displaying moderate staining. Granulopoiesis and erythropoiesis are negative. b An example of a myeloproliferative neoplasm displaying marked overexpression of CCN2 with many megakaryocytes showing moderate to strong cytoplasmic staining
In MPN, the findings were largely similar, although a few cases (N = 7, 13%) clearly stood out by a much stronger staining of the megakaryocytes with a markedly increased number of megakaryocytes displaying moderate or strong cytoplasmic staining, as illustrated in Fig. 3b. The moderate/strong staining megakaryocytes could morphologically not be discerned from the negative/weak staining megakaryocytes within the same biopsy. The CCN2 score ranged from 0.00 to 5.90 with a median score of 0.54. The CCN2 score of the MPN group as a whole was not statistically different from the normal control group (p = 0.741).
The CCN2 scores of all 75 normal and MPN cases were analyzed by a box-and-whisker plot, which showed 7 outliers (i.e., values greater than 1.5 IQR plus the third quartile), with a significant higher CCN2 expression than the rest of the cases. These cases with a high number of moderate and strong staining megakaryocytes consisted of 3 ET cases (CCN2 scores: 2.82, 3.10, and 3.38), 1 pre-PMF case (CCN2 score: 2.90), 1 post-PV MF case (CCN2 score: 4.65), and 2 PMF cases (CCN2 scores: 2.42 and 5.90).
Correlation of CCN2 expression with fibrosisAll of the normal BM biopsies and 17 of 75 (23%) MPN cases (10 × ET, 5 × PV, 2 × pre-PMF) showed no fibrosis (MF-0). Mild fibrosis (MF-1) was found in 7 MPN cases (3 × pre-PMF and 4 × PV), moderate fibrosis (MF-2) in 11 MPN cases (7 × post-ET MF, 2 × post-PV MF, 2 × PMF), and severe fibrosis (MF-3) in 18 MPN cases (3 × post-ET MF, 8 × post-PV MF, 7 × PMF). No correlation was found between the CCN2 score and the amount of BM fibrosis (p = 0.966).
Correlation of CCN2 expression with clinical parametersCCN2 scores did not correlate with age, sex, type of driver mutation, blood values (hemoglobin, leucocytes, platelets, LDH) or the occurrence of thrombovascular events in MPN patients. There was no significant difference in CCN2 score between the different MPN subgroups (p = 0.703).
CCN2 protein overexpression in MPNIn 7 MPN cases (13%), immunohistochemical staining by the 10095S antibody showed significant CCN2 overexpression of megakaryocytes. These were 3 ET cases, 1 post-PV MF, 1 pre-PMF, and 2 PMF cases. Their characteristics are shown in Table 1. Four of them were males and three were females, and the median age was 58 years (range 24–70 years), which was not significantly different (p = 0.338) from the 48 MPN cases without CCN2 overexpression (median age 62 years, range 23–77 years). Blood values (hemoglobin, leukocyte counts, platelet counts, LDH) were not significantly different from patients without CCN2 overexpression. Thrombovascular events were as common in MPN patients with CCN2 overexpression (28%) as in those without (27%). Four cases showed no fibrosis (MF-0), 2 showed moderate fibrosis (MF-2), and 1 severe fibrosis (MF-3).
Table 1 Myeloproliferative neoplasms with CCN2 overexpressionSix of the MPN cases with CCN2 overexpression contained/showed a JAK2 V617F mutation/clone with a variant allele frequency (VAF) ranging from 5.8 to 79%, not significantly correlating with the CCN2 score (p = 0.090). The seventh, one of the PMF cases, contained/showed a CALR exon 9 (p.Lys385fs, type II) mutation/clone. The presence of additional pathogenic non-driver mutations was investigated, and an additional mutation was detected in 6 of the 7 cases, being DNMT3A (ET and PMF), NFAIP3 (ET), TP53 (post-PV MF), SF3B1 (pre-PMF), and CUX1 (PMF).
One patient with PMF deceased due to a pneumonia and the patient with post-PV MF deceased after having progressed to a blast phase (in the form of an acute megakaryoblastic leukemia). One patient with ET showed progression to PV. The other patients did not show progression, albeit the follow-up time was limited.
Staining with additional CCN2 antibodiesTo assess whether the CCN2 staining of the megakaryocytes by the 10095S antibody was specific, 5 MPN cases showing overexpression as well as 5 normal BM biopsies were additionally stained by 2 other CCN2 antibodies: FG-3114 and the 86641S antibody. Like the 10095S antibody, these two other CCN2 antibodies also showed cytoplasmic staining of the megakaryocytes. In addition, the aggregated, weighted staining score for the FG-3114 and the 86641S was higher in the 5 selected MPN cases than in the controls, further supporting the notion that the staining with these 3 antibodies indeed reflects CCN2 protein expression.
留言 (0)