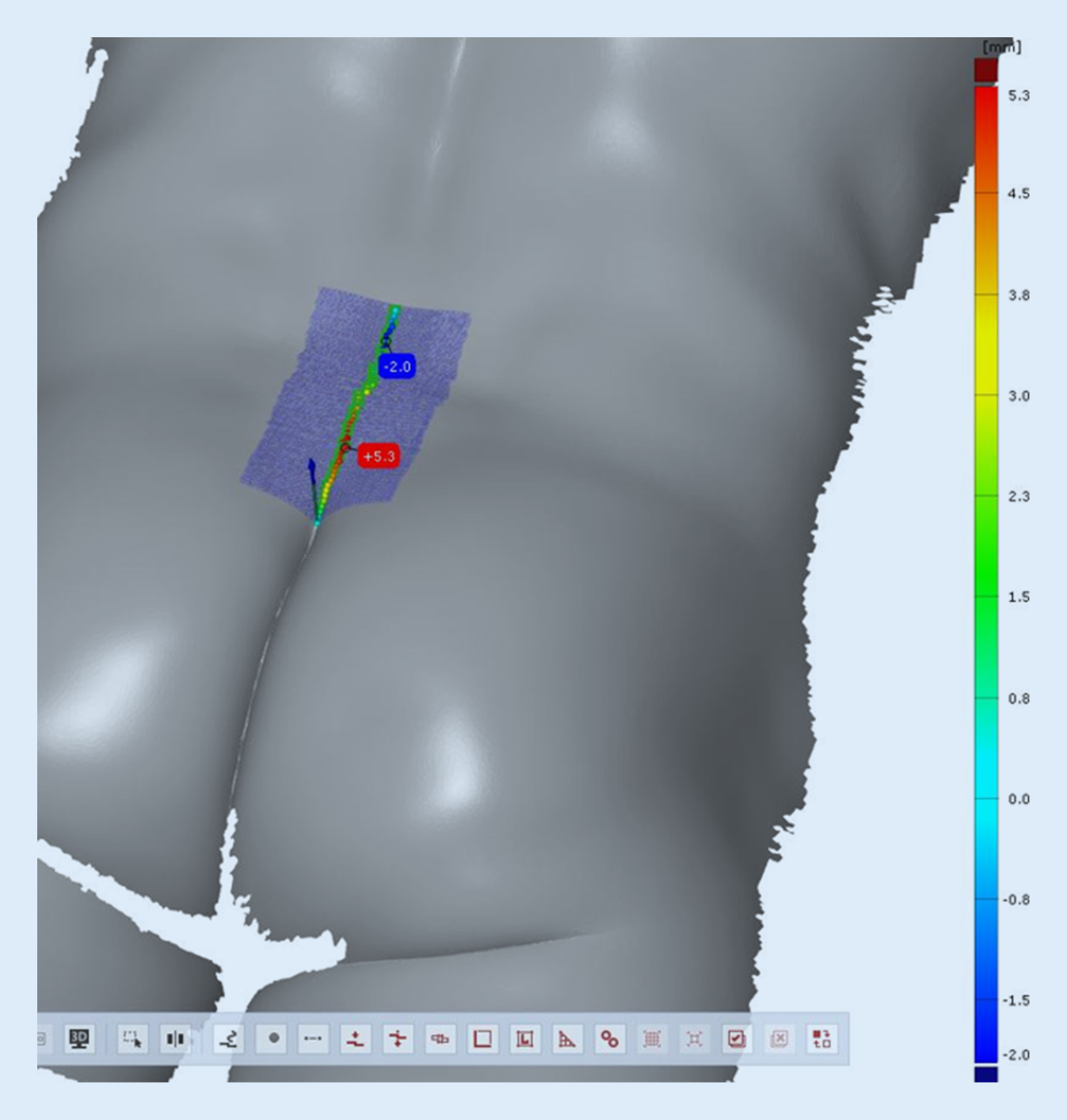
This study marks the first endeavor to delineate the anatomical trajectory of cut hair fragments from the neck down to the intergluteal opening, a site commonly harboring pilonidal injections and hair nests. Leveraging a novel optical scanning tool commonly used for high-end industrial product quality control and building scanning, we successfully employed the 3D volume scanning technique on the region spanning from the thoracolumbar area to the intergluteal fold. This innovative approach allows for measurement without the risk of soft tissue displacements of unknown magnitude that may arise when using mechanical measuring devices.
Our findings underscore the significance of glabellar cushion size, as it is smaller in PSD patients and remains so throughout their lives, rendering them susceptible to further disease despite intermittent surgical intervention. Notably, females enjoy protection against PSD due to their larger cushion height, a factor correlated with the lower incidence of the disease among women both nationally and globally [17,18,19]. This protection may be an additional consequence of the reduced axial hair force exhibited in women, contributing to their resilience against PSD [20].
Gluteal depth has recently been studied in a larger cohort, revealing no discernible differences in intergluteal fold depth between PSD and non-PSD groups [16]. Akinci [12] highlighted that the maximal depth is consistently near the anus, an area with a notably low incidence of pilonidal disease. With intergluteal fold anatomy appearing to play a lesser role, why do flap procedures yield remarkably low recurrence rates in PSD? How do these procedures alter the anatomy above and within the intergluteal region?
Interestingly, flap procedures deliberately aim to avoid the intergluteal fold, as wound healing issues are more prevalent when the wound approaches the midline in that region [21]. Irrespective of the flap technique employed, whether it be an advancement (e.g., Karydakis, Bascom) or rotation (Limberg, Dufourmentel) flap, all are executed in the region of the glabella sacralis—cranially to the intergluteal fold’s opening. These procedures shift healthy paramedian tissue into the midline. This may explain why flap procedures, regardless of their technique, demonstrate the lowest recurrence rates achievable today [13].
Our study demonstrates significant disparities in the height of the soft tissues covering the glabella sacralis between genders, with lower heights in PSD patients. Mechanistically, this makes it easier for hair to slide down and avoid being obstructed by a soft tissue cushion. Intriguingly, females display larger and higher glabellar cushions, aligning with the lower incidence of PSD observed in women [18, 19]. While PSD is undeniably a multifactorial condition, factors like reduced sweating [22], positive family history [23], and stiffer hair (higher axial hair force) put men at a disadvantage as compared to women [20]. Contributing skin resilience factors, as suggested by Karydakis, are still unexplored [24]. Obviously, anatomical shape variations have their part in this disease as well, as we have found.
The potential role of BMI in fostering PSD has long been debated, yet no concrete evidence has been presented yet. The Minnesota study, encompassing 31,497 students, failed to reveal any correlation (cited from Cowan to Dwight, derived from Franckowiak’s thesis as referenced by Obedman [25, 26]). Recent research similarly found no correlation between BMI and intergluteal fold depth (IGFD) in a German cohort of 200 patients [16]. Additionally, Balik’s comparison of obese PSD and non-PSD patients, measuring fat pad thickness at the sacrococcygeal junction, unveiled no discrepancies [27]. This suggests that obesity does not necessarily influence anatomical soft tissue changes at this junction.
Several aspects of our study setup warrant discussion. An upright position for measurements ensures that tissues remain undistorted. The alternative, a prone position, could introduce more physiological distortion. However, it remains unknown whether PSD development occurs during sitting, sleeping, or in an upright posture. Although gluteal muscle movement while walking might facilitate hair insertion into the skin, the exact posture’s role remains uncertain. Page’s 1969 study highlighted that hair movement into the sinus is promoted by walking when the orientation of the hair scale is appropriate [28].
Additionally, spinal column posture is of interest. While lumbar lordosis measurement was not studied in the current investigation, it might be valuable to ascertain whether hyperlordosis predisposes to increased hair loss and a reduced PSD risk. Hair slides downward when there is intimate skin contact, and detachment may redirect hair away from the midline. These data are present within our study and require further analysis.
These considerations, however, do not significantly alter our findings. The glabella sacralis is indeed found to be covered with a thicker protective soft tissue cushion in non-PSD participants, while PSD patients lack this protective cover, rendering them susceptible to the disease.


留言 (0)