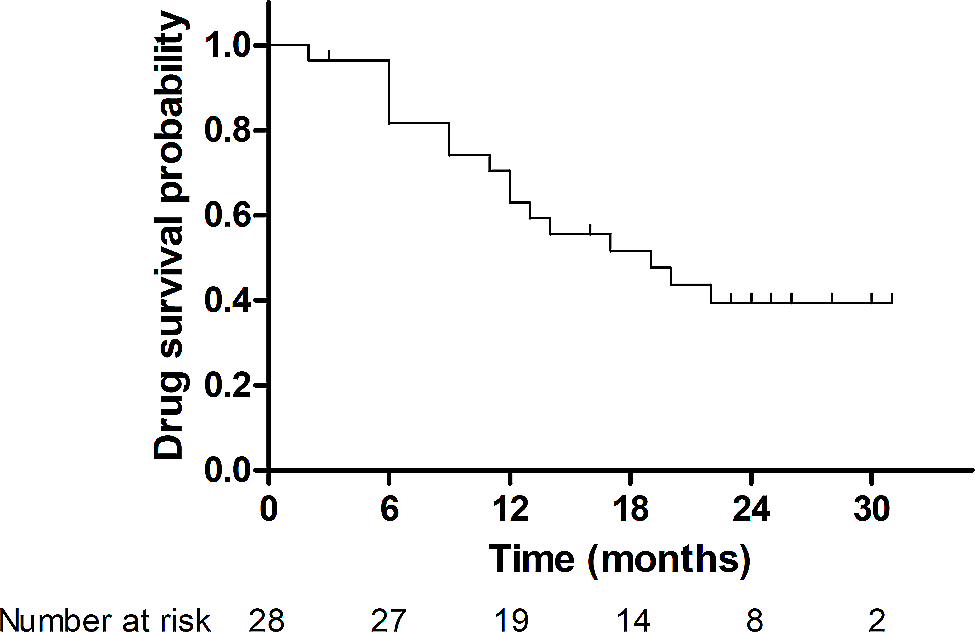
In this study, we showed that in patients with difficult-to-treat RA who failed to bDMARDs after failure to a JAKi, a second JAKi has a drug survival rate of up to 40% at 2-year. Given that all patients included had difficult-to-treat RA, the drug survival rate was acceptable, suggesting that the second JAKi is a potential therapeutic option available to patients with difficult-to-treat RA who failed to a JAKi and one or more subsequent bDMARDs.
In vitro kinase assays have demonstrated that different JAKis have different JAK selectivity. Tofacitinib is a potent inhibitor of JAK1 and JAK3 and is less specific to JAK2 and tyrosine kinase 2 (TYK2); baricitinib is a selective JAK1 and JAK2 inhibitor with moderate activity against TYK2 and less activity against JAK3; and upadacitinib is a selective JAK1 inhibitor [17,18,19]. Considering that distinct cytokine signaling pathways are mediated by varying JAK complexes, different JAKis with different JAK selectivity, may have different effects in the treatment of RA [20]. This could be a rationale for using another JAKi in patients with RA who have previously failed to a JAKi. Indeed, a previous study has reported sequential use of second JAKi after failure to a first JAKi as an efficacious option in patients with RA [14]. Our data add to the previous study that a second JAKi could also be considered as a therapeutic option when a patient with RA has failed to a JAKi and to subsequent bDMARDs.
Regarding drug survival, the estimated 2-year drug survival rate of the second JAKi was 39.3%. This drug survival rate is relatively low compared with a previous post hoc analysis evaluating drug survival of JAKi (tofacitinib, in particular) in patients with RA that reported an estimated 2-year drug survival rate of 75.5% [21]. This is not surprising considering that all patients included in our study fall into the definition of difficult-to-treat RA [16] at the time of initiation of the second JAKi. As we included only the patients with RA who failed to a JAKi and one or more subsequent bDMARDs, all patients received at least two ts/bDMARDs prior to the second JAKi. In contrast, the mean number of bDMARDs used by the patients included in the previous post hoc analysis prior to the use of tofacitinib was 1.6 [21]. Therefore, although the drug retention rate of the second JAKi in our study seems relatively low, it could be interpreted that as much as 40% of patients with difficult-to-treat RA who previously failed to a JAKi still have chance to improve upon treatment with another JAKi. Moreover, in our country, as per the national insurance reimbursement policy, patients with RA using JAKi or bDMARD are mandated to get their disease activity assessed every 6-month. Only if the effectiveness observed at the first 6-month of use is maintained thereafter can the JAKi or bDMARDs be used persistently. Given these circumstances, we presume that drug survival could be considered as a proxy of drug effectiveness in our study population.
The use of the second JAKi was effective at 6-month in terms of improving TJC, SJC, VAS, CRP, and DAS28. Given that all patients included had difficult-to-treat RA, the effect of the second JAKi on the change of disease activity observed at 6-month is encouraging. However, as shown in Fig. 2, the degree of change in disease activity parameters varied among patients. For instance, ΔDAS28-ESR (i.e. change of DAS28-ESR from baseline to at six months of use of the second JAKi) was as large as -4.79 in one patient, whereas in another patient DAS28-ESR was rather higher at six months of treatment (ΔDAS28-ESR = 0.15). An important clinical question arises as to whether there is a subgroup of patients that responds better than the others. In particular, given that all patients failed to a JAKi previously, we sought whether the reason for discontinuation of the previous JAKi is associated with the effectiveness or drug survival of the second JAKi. When ΔDAS28-ESR was compared according to the reasons for discontinuation of the previous JAKi, no significant difference was observed among groups (p = 0.486, data not shown in the Results). In addition, the drug survival rate of the second JAKi also did not differ among patients who discontinued treatment with the previous JAKi for different reasons (p = 0.423, data not shown in the Results). Moreover, as shown in Table 4, no association was observed between the reason for discontinuation of the previous JAKi and the outcome of the second JAKi, indicating that the reason for the discontinuation of the previous JAKi does not necessarily mean that the second JAKi will be discontinued for the same reason. For instance, of the 16 patients who discontinued treatment with the previous JAKi owing to primary failure, excluding one patient who discontinued the second JAKi of insurance coverage issue, four patients experienced primary failure with the second JAKi, three patients experienced secondary failure with the second JAKi, one patient experienced adverse event with the second JAKi, and the other seven patients were maintained on the second JAKi as it was effective (Table 4). Therefore, the so-called class effect does not seem to apply to JAKis, and switching to another JAKi after failure to a JAKi and subsequent bDMARDs, could be considered regardless of the reasons for the discontinuation of the previous JAKi.
Table 4 Reasons for discontinuation of first and second JAK inhibitorsThe following limitations should be noted in our study. First, we lack data on other disease activity parameters including Clinical Disease Activity Index and Simplified Disease Activity Index. Second, the observation duration was relatively short and the number of patients small to make a robust conclusion. Third, this study was retrospective in design. As this was a retrospective study, glucocorticoid was not used in a predefined standardized protocol. Fourth, as this was a study based on an electronic medical record review, information on adverse events and treatment discontinuation may have been underreported. Further prospective randomized controlled trials with larger sample size and longer follow-up are needed to confirm our observations.







留言 (0)