As RA itself is known to be related to an increased risk of infection [24], it is of great interest to know which other factors presented by the patients may lead to an additional risk. Some of these factors can be specific to each population, with different socioeconomic conditions, management protocols and access to treatment and there is little data available about the South American population.
We found an incidence of 13 infections per 100 patient-years. In 2002, Doran [3] saw an incidence of 9.57 SI per 100 patient-years, whereas the incidence of all infection events in this cohort was 19.64 per 100 patient-years. More recently, in 2019, a large national US cohort [24] showed a high frequency (19.6 per 100 patient-years) of SI when following patients for long periods (15 years). However, in 2020, Wang observed 10.8 SI per 100 patients-year after a year of segment in an Australian cohort [25].
Our study associated the occurrence of SI events with the presence of comorbidities – such as pulmonary fibrosis, CKD, central nervous system diseases –, the use of moderate doses of corticosteroids, and reduced functionality as assessed by the HAQ. These results were similar to those already described in other cohorts [8,9,10,11,12, 26] and some of these factors can be associated, such as higher corticosteroid doses and pulmonary fibrosis. In a recent Taiwan cohort [27], Ng KH et al showed a relationship between corticosteroid daily use and mortality due to infection and disease activity in patients with pulmonary fibrosis associated with RA.
In contrast, factors that were also related to the occurrence of infectious events in other cohorts, such as disease duration, disease activity assessed by CDAI, elevation of inflammatory reactants and diabetes [11, 12, 24, 28] did not achieve statistical significance to be included in our final model. This can be justified by the homogeneity of the cohort sample, in which patients with moderate disease activity and with a long disease duration (14 years on average) predominated. Furthermore, the association between SI and diabetes was not always achieved in RA cohorts [15, 25, 29]. BIOBADABRASIL, Brazilian registry for biologic drugs, didn’t found association between diabetes and SI in patients with rheumatic disease either [15].
Regarding the use of corticosteroids, much effort has been done to identify a dose limit considered safe for use in the treatment of RA. Previous studies were able to show that the use of corticosteroids, even at low doses, such as equal to or less than 5 mg of prednisolone (or equivalent) per day, was associated with a higher risk of infections. This risk increases with the dose escalation of the medication [8, 11]. In this cohort, the association between corticosteroid use and SI also occurred in a dose-dependent manner, with the highest association found with doses equal to or higher than 15 mg of prednisolone (or equivalent). According to the most recent recommendations of the EULAR and ACR, if steroids are necessary as initial or bridging therapy, they should be discontinued as soon as possible [30, 31].
We found no statistically significant association between the use of any type of DMARD and the occurrence of SI. This finding differs from what is described in the literature [13,14,15, 29]. In the South American registry for biologic monitoring [32], Ranza et al. found an adjusted hazard ratio (HR) of 2.03 [1.05–30.9] comparing biologic DMARDs and synthetic DMARDs, and Quartuccio [29] observed that this risk was higher in the beginning of any biologic drug.
Reduced functionality assessed by the HAQ was another important factor associated with SI in the REAL cohort. Similarly, Weaver et al found a 30% increase in the risk of SI for every 0.4-unit HAQ-DI increase [9]. This metric can be influenced by pain, swollen joints, damage, deformities but also by fatigue and depression [33]. Previous studies showed that early treatment, tight disease control and biologic use can reduce progression of disability on RA [34, 35].
When performing the additional univariate analysis, “other coronary disease” and COPD were associated with SI with an OR of 7.48 (95% CI: 2.45–22.81) and 3.92 (95% CI: 1.78–8.59) respectively. The association between coronary disease and infections complications has already been described in literature, wherein certain infections agents have been implicated in atherosclerotic disease [36, 37]. Furthermore, SI is associated with 10-fold risk of 30-day death after an acute myocardial infarction [38] However, no causal relationship between chronic coronary disease and SI has been found and further studies are needed for better understanding this data. In turn, COPD is a known risk factor for SI and the risk for chronic infections and multidrug-resistant organisms is also higher compared to the general population [39].
The main limitation from this study is about selection bias, since data were collected only in tertiary centers. In these hospitals, there is a greater number of patients with severe and refractory diseases, for whom the use of biological medications and small molecules are available according to the national treatment protocol [39]. Theoretically, these patients with severe disease and a high level of immunosuppression form the group with the greater risk of SI [7, 9].
Furthermore, information was not available on some variables that could potentially influence access to the health system and the risk of SI such as color and education level. However, social level, another potential influencer of access to the healthcare system, was included and did not reach statistical significance (p > 0.05).
Given the important frequency of respiratory infections in this cohort, the lack of information on vaccination coverage is another limitation. Data was collected before the COVID19 pandemic, but airway infections such influenza, pneumococcus and Hemophilus B are important causes of SI that are potentially preventable with vaccination. In a systematic review, Furer et al showed a higher incidence and prevalence of vaccine preventable infection in patients with autoimmune inflammatory rheumatic disease (AIRD) compared to general population [40]. Other cohorts have shown a suboptimal vaccine coverage through patients with AIRD [41], even in tertiary centers [42, 43].
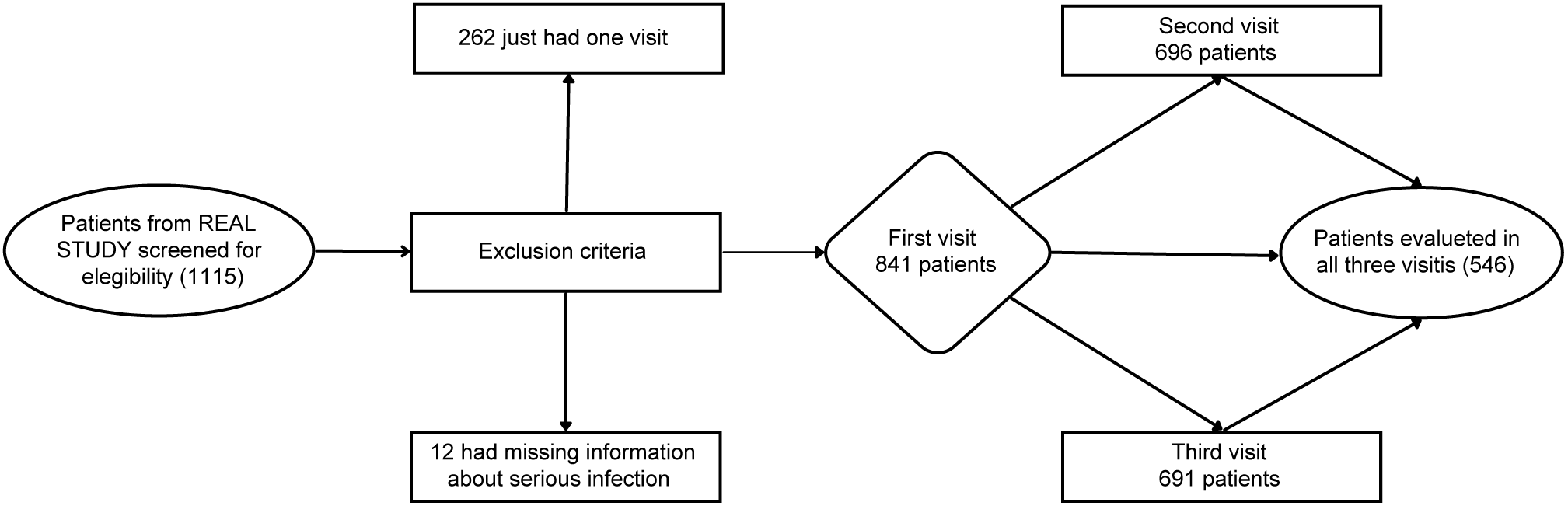
In addition, as this is an observational study, information and confounding biases are possible. This may justify the absence of sepsis diagnoses among SI and the small number of patients with a history of SI (16 patients) before the start of the follow-up. Another study limitation was the number of patients who did not attended all the visits (35%), as expected in a real-life study, in which losses are usually higher.
Despite those limitations, this study, as derived from a real-life nationwide cohort (REAL study), included a large representative population sample. Data assessing SI in this population in Brazil are still scarce.







留言 (0)