In the Polish healthcare system, the National Health Fund of Poland is the only institution contracting and accounting the healthcare services financed by public funds. Citizens paying mandatory health insurance are entitled to healthcare access. Simultaneously, the private health insurance sector is poorly developed so the NFZ nationwide data can be considered as the most complete and reliable. So, our study has covered the Polish population.
The cancers epidemiology
In the current study, we have analyzed selected the most common cancers diagnosed in Poland in 2015–2021, based on the National Cancer Registry database and our previous study concerning two regions of southern Poland: the Silesian and Subcarpathian voivodeships [5]. It was colorectal cancer, lung and bronchus cancer, skin cancers (without melanoma), kidney cancer except for renal pelvis, and two gender-related cancers: breast cancer among women and prostate cancer among men. Such structure of most prevalent cancers does not differ from Western societies with high Human Development Index (HDI). Our results correspond with available data [9].
One of the most common cancers diagnosed in Poland in 2015–2021 was colorectal cancer. This disease remains the third of the most frequent cancers diagnosed worldwide and the second cause of cancer-related deaths because of insufficient diagnostics and ineffective therapy [2, 11,12,13]. The high incidence of colorectal cancer observed in Poland might be affected by the socio-economic transformation of the 1990s and progressive changes in lifestyle and Western diet change as well as the low utilization of screening programs (such as screening colonoscopy). The high prevalence of low physical activity, overweight and obesity, smoking, and excessive alcohol consumption remain serious problems for the nationwide health policy. The stabilization of the colorectal SIR in 2015–2019, observed in our study, corresponds with the Xi and Xu findings, according to which in the high-developed countries the burden of CRC stabilizes at a relatively high level, over four times greater compared to the countries of low HDI [2].
The lung cancer were the second of the most frequent cancers diagnosed nationwide in 2015–2021 without gender differences. The available data underline the relationship between smoking and air pollution and the risk of lung cancer [14,15,16,17,18]. Also, in Poland lung cancer incidences and air pollution are linked [19], especially that according to the World Bank Group, Polish cities remain 36 of 50 of the most polluted urban areas of the European Union [20].
Our results show that the incidence rate of lung cancer has decreased in 2015–2021 all over the country. This could be affected by the social changes already observed over ten years ago resulting from the decrease in the smoking prevalence in 2015 compared to 1999 [21] and the changes in the smoker’s structure [3].
The high prevalence of skin cancer (C44) observed in our study does not deviate from most of the countries with the domination of Caucasians. In the last thirty years, skin cancer morbidity has tripled in the United States and Europe [22].
The decrease in skin cancer’s APC in most of the northern and northern-west subregions may be associated with the limitations of the healthcare system resources such as low numbers of healthcare providers and available assets, such as in-hospital beds and the limited number of medical doctors in those areas (Fig. 1a and c). Such findings correspond with Augustin et al. results indicating that the availability of medical doctors, especially general practitioners, and potential difficulties in accessing them are associated with the number of skin screening tests [22].
Breast and prostate cancers were the most frequent oncological diseases diagnosed in Poland in 2015–2021 among women and men, respectively. Those cancers are the most frequent oncological diseases diagnosed in highly developed countries.
In our study we found increased morbidity for prostate cancer in 2015–2019, meanwhile, the prevalence of breast cancer remained stable. The increased burden of breast cancer in 2015 was observed in wealthy subregions including the largest urban centers: cities of Łódź, Poznań and Warsaw as well as the subregions of Tricity and Konin. Those findings correspond with previous results. Pacelli et al. have shown that after the period of increase of incidence the morbidity and mortality of breast cancer in most developed countries have stabilized or even decreased slightly in the last 15–20 years [23]. It may be caused by the wide spreading of social campaigns and screening programs reducing inequalities and improving accessibility of mammography [24]. Moreover, when assessing the breast cancer burden, especially in survivors, we should not ignore the progress in the therapy, in particular HER2-positive and luminal subtypes. The increased morbidity of breast cancer, observed in our study, corresponds with Didkowska et al. results [9].
We found an increased SIR of prostate cancer in 2015–2019 as well. According to the previous study, the C61 APC was the highest among the most common cancers diagnosed in Poland [9]. The etiology of prostate cancer is relatively weakly examined compared to other cancers. The early diagnosis is essential but over 75% of men aged over 45 have never performed the PSA measurement.
The COVID-19 impact
In 2020 a visible decrease in the SIR for each of the analyzed cancers was observed. It is most likely related to the limited accessibility and availability of healthcare services for non-COVID diseases because of healthcare staff and resources’ engagement in fighting the COVID-19 pandemic. The second important aspect was the procrastination of not requiring urgent medical consultations, physical examinations, and diagnostic procedures [25]. This was caused both by the care of the medical professionals’ maintenance and patients’ and physicians’ fear of COVID-19 infection, especially before the vaccine development.
The COVID-19 pandemic has exposed health inequalities and had a dramatic impact on cancer patients. Due to pandemic restrictions, most healthcare services have been realized with the use of remote methods, such as telemedicine. The traditional face-to-face medical consultations with physical examination had been limited [26, 27]. The percentage of physicians’ teleconsultations increased from 1.2% in March to over 60% in April 2020 [28]. Such patients’ management in the pandemic reality was difficult and probably in many cases delayed diagnosis, and treatment, and have affected the suboptimal therapy. Moreover, cancer patients had a higher risk of SARS-CoV2 infection and complications [25, 28].
Our results show a print of such unfavorable pandemic conditions by the visible reduction of SIR of each of the analyzed cancers in 2020.
In 2019, just before the pandemic occurred, the burden of colorectal and lung cancer had been characterized by a clear spatially dependent decreasing division along the northern-west– southern-east axis and these findings correspond with the previous results [9]. Subsequently, in 2020 the incidence of colorectal cancer has decreased especially in the eastern subregions (those areas are characterized by relatively unfavourable economic conditions) while the lung cancer incidence rate has decreased equally across the country. The reduction of colorectal cancer was most likely affected by the abandonment of standard medical consultations and the replacement of them by remote methods. It caused a drastic limitation in the number of performed endoscopic [27].
In 2020, compared to the period preceding the COVID-19 pandemic, the slightest decrease in the incidence of CRC was in subregions of Gliwice, Łódź, Tarnów, and Cracow– rural. Those areas are large urban centers with well-developed healthcare infrastructure, including diagnostic and oncological resources. Despite the involvement of the healthcare system in the fight against the pandemic, patients living in these areas were in a more favorable situation enabling the treatment and diagnosis of diseases other than COVID-19.
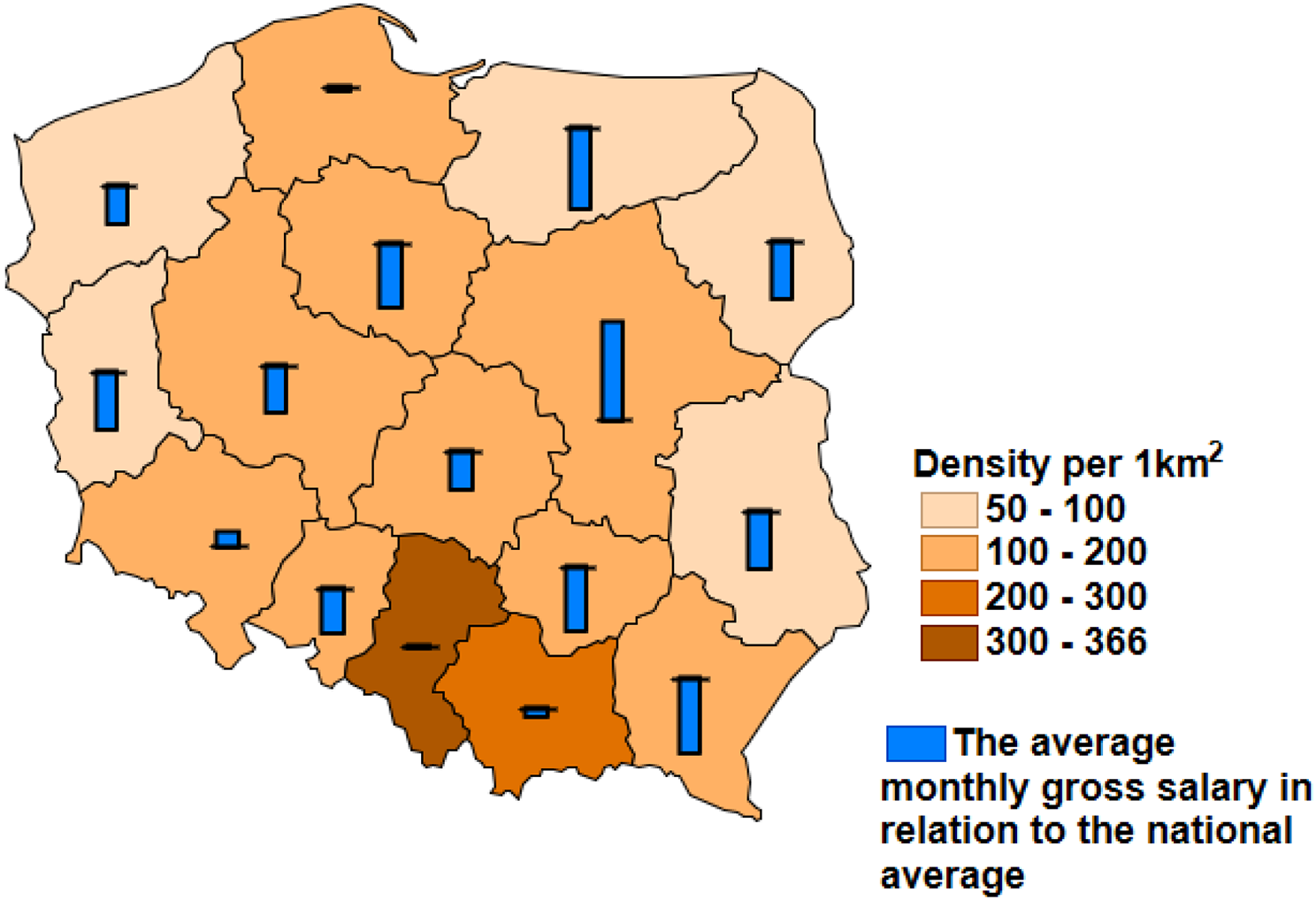
The visible SIR decreasing in the northern-west– southern-east axis in 2020 was observed in the case of skin cancer and breast cancer among women as well. The subregions of southern-east areas of Poland are mainly rural with relatively poor and unevenly allocated healthcare resources, especially specialized ones, e.g. lower number of the hospital beds in the oncological departments per 100,000 citizens and medical doctors combined with unfavorable economic status below the national average (as presented in Figs. 1 and 2). The pandemic-related limited access to healthcare supplies in rural areas may be the consequence of the insufficiency of the healthcare system and human resources [26]. However, it cannot be ignored that this problem is multi-faceted and it depends on the combined impact of many factors such as socio-economic, environmental, and the availability and organization of healthcare and it requires further analyzes of the impact of each factor at the local level.
The spatial differentiation of the cancer prevalence as well as the health inequalities were observed in many countries, including European states. The social determinants of health inequalities are well established but there is no exhaustive data on the spatial ones. In France at the beginning of the 21st century, the standardized mortality rate of cancers in the northern counties was almost twice as high as in the southern areas, which was caused by environmental, social, and spatial conditions. The spatial differentiation of the cancer burden was affected by the unequal access to healthcare resources occurring by the smaller use of medical services in the areas with a smaller number of medical entities. This contributes to less favorable prevention, early diagnostics, and appropriate patient management. So that remote patients have worse access to specialized health centers and lower survival chances [29].
The spatial differentiation of the cancer prevalence was found in Slovakia as well. Slovakia is close to Poland because of the similarities in the social and political transformation observed at the turn of the 80s and 90s. Since the middle of the 80s, the burden of communicable diseases had decreased, and cancers became the leading health problem in Slovakia. Moreover, the significant disproportion between the wealthy regions and the southern and western areas is noticeable both as the inequality of the socio-economic factors as well as the better quality of life and healthcare [30].
The Polish healthcare system has been underfinanced for many years and successive governments since 1990 it has been occurring as one of the leading problems that has to be solved.
In 2005 and 2019 Poland spent 1.05 and 2.3 billion euro on cancer treatment respectively [31]. The increase in the finances dedicated to oncology was associated with the development and implementation of the so-called “oncological package” which was supposed to increase the availability and efficiency of oncological healthcare. Simultaneously, according to the National Cancer Strategy 2020, one of the milestones was to increase the percentages of 5-year survivals in cancer diseases and improve the prevention and screenings [9]. According to the EUROCARE-5 study, the cancer 5-year survival rate noted in Poland was significantly lower than the EU average (43% vs. 54.6%). Those targets were essential, from the public health’s point of view because according to WHO, over 40% of cancer incidences might be avoided or successfully treated in case of early detection [32].
Unfortunately, the cancer prevention expenditures in 2012–2015 decreased by 10% [33] as a low percentage of Poles utilized screening tests, such as colonoscopy or mammography, despite the access to these programs.





留言 (0)