Men and women with COVID-19 infection had different profiles: women were generally older than men, had lower socioeconomic status, lived in LTC facilities more frequently and had a higher morbidity burden. Women also had a higher frequency of COVID-19 infection than men.
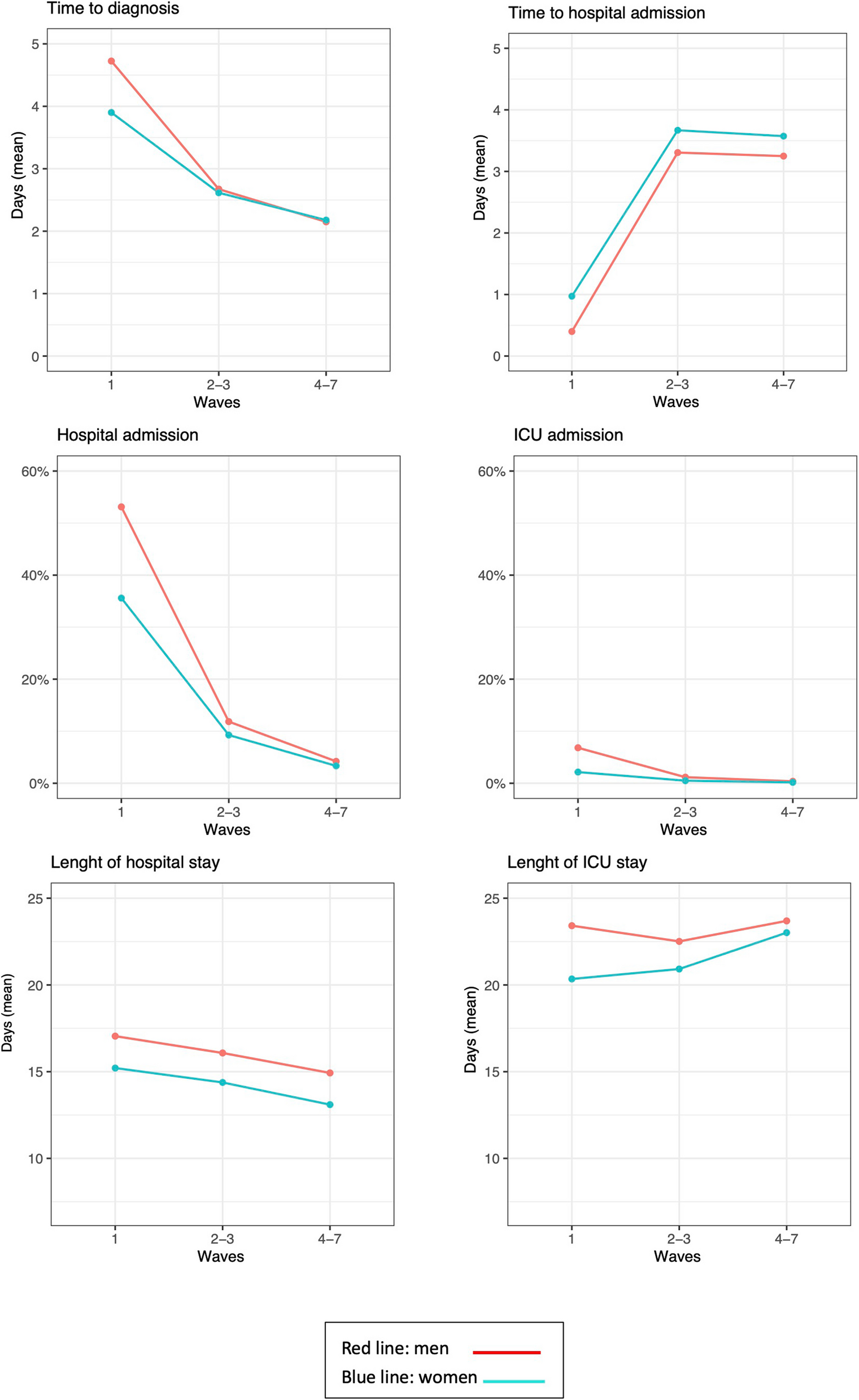
The health care received throughout the pandemic differed between men and women, with gender inequalities being observed. Women were diagnosed earlier than men, but these differences disappear in the last waves of the COVID-19 pandemic. Women were admitted to hospital and ICU less frequently than men and their stays were also shorter. Overall, these differences narrowed throughout the pandemic, but persisted for all the period analysed, even after adjusting for other characteristics such as age, socioeconomic status, morbidity burden or the patient's place of residence. Differences in sociodemographic characteristics and morbidity between women and men could explain partially the gender differences found, mainly in the later phases of the pandemic, but not in the first waves. Particularly striking is the importance of residing in an institution in the early phases and the high importance of socioeconomic status throughout the pandemic as explanatory factors for the gender inequalities found.
As widely described, the incidence of COVID-19 in women was higher than in men [15]. There are a number of circumstances that have been associated with these gender differences, such as genetic or hormonal factors [16], but also other factors that generate greater vulnerability in women, such as their lower socio-economic status [17].
Gender inequalities in health care have been observed. Men are admitted more often to hospital and ICU and stay longer in hospital, which results in a greater therapeutic effort. This phenomenon is well known and, unfortunately, is not limited to health crises. It has already been observed that, facing the same health problem, hospitalization rates are generally lower in women than in men [18, 19] which suggest that women could face more obstacles in accessing health care. So, women tend to stay at home, rather than being hospitalized and the length of hospital stay is generally shorter [20], which could be explained by their caring role, as it has been already described [21]. But there are other factors that may be involved in gender inequalities in health care, like health attitudes, health behaviours and health care needs [22]. In the context of the COVID-19 pandemic there are also other circumstances that may have contributed to gender inequalities. Men are usually cared by women in their homes but women, often older, are referred to nursing homes when they are ill. Women living in LTC facilities are in a situation of greater vulnerability, which increases if they also suffer from dementia, which has been associated in this context with a higher risk of not being admitted to hospital [23]. The greatest impact of the COVID-19 pandemic on institutionalized people has been associated with physical and psychological factors, living conditions and deficient policy responses [24,25,26], which seems to be associated with difficulty in accessing health care. Finally, women have lower socioeconomic status than men, a factor classically associated with poorer health care attention [27, 28].
Differences in all indicators of access to and use of health services are greater at the beginning of the pandemic and tend to decrease as the pandemic progresses, but do not disappear completely. These results show that, in times of health system crisis and great uncertainty, existing inequalities are exacerbated. In the case of COVID-19, the lack of clear protocols for action and a limited definition of the disease in the early stages of the pandemic that did not take gender differences into account may explain these greater inequalities in utilisation [29]. Moreover, as some authors point out [29], hospital and ICU admission are indicators of the severity of the disease, but also of the diagnostic and therapeutic effort required. In our study, and as it has been described in the literature [30], men had higher mortality rates than women. However, when we described the use of health services only in patients who died within 30 days of diagnosis, the gender inequalities in the use of services remained (results not shown). In these sub-analyses, men also showed a higher frequency of hospital admission than women, for all three time points analysed. Thus, in wave 1, men who died within 30 days of COVID-19 diagnosis had a hospital admission in 76.7% of cases, while in women this percentage was 69.6% (p = 0.031). The length of hospital stay was also longer in men, with statistically significant differences for the three time points analysed. Finally, admission to the ICU was also more frequent in men than in women, with the greatest differences in wave 1 (10.7% in men vs. 3.6% in women). This fact has been already observed in Spain, where the probability of admission to the ICU was higher in deceased men than in deceased women, which could indicate, among others, a greater therapeutic effort in men than in women, implying a gender bias in health care [31].
In addition, it should not be overlooked that some authors point to a higher percentage of undiagnosed excess COVID-19 mortality in women, related with an underreporting of COVID-19 deaths among women who died in LTC facilities, especially during the first wave [32], a higher frequency of deaths in women from other causes consistent with COVID-19 [31] and a greater hospital access and care in men [33] that have implied higher reporting of deaths in men in the pandemic. This aspect requires further attention and underlines the need for a gender-sensitive definition of the disease and for sex-disaggregated information in future pandemics [34].
In the first pandemic waves, especially in the first wave, when gender inequalities are greater, these inequalities are not justified either by sociodemographic factors or by morbidity factors of the subjects. As mentioned above, the confluence of factors such as older age, greater morbidity burden, lower socio-economic status and residence in a LTC facility explain, at least partly, the differences found between men and women in the later phases of the pandemic, but not at the beginning of the pandemic. Several factors could explain these differences between the early and late phases of the pandemic. Confinement may have made it particularly difficult for women to seek medical care, due to the burden it entails, which may have prevented them from seeking medical assistance [35]. There were also situations of gender-based violence, in which women did not seek medical care [8, 36]. Finally, the great heterogeneity of existing protocols in the initial phases may have increased the existing gender bias [4].
This study has some limitations. The sex disaggregation available in the electronic registers is binary in nature, which does not necessarily equate to the sex of the subject, and does not allow for the identification of persons with diverse gender identities. Unfortunately, this is the only information available. There are also some limitations inherent to observational studies, such as the existence of incomplete information. In this sense, quality of the data may have changed across the waves. The cause of hospital admission was not available. In order to solve this problem, a range from -15 to 30 days from hospital admission to COVID-19 diagnosis was applied. Some of the patients living in LTC facilities who were not hospitalized could have been treated in one of the “COVID centers” set up in Aragón in the first waves of the pandemic. Unfortunately, this information is not available. Other information not available was the severity of the infection. This aspect is relevant as it could have conditioned the use of health services by patients, mainly aspects such as the decision to be hospitalized or to be admitted to the ICU. However, as noted above, we replicated our analyses only in patients who died within 30 days of diagnosis, as a proxy for high-severity COVID-19 cases, with results similar to those in the general population. Finally, it is important to note that what is statistically significant is not always clinically relevant, and further studies are needed to understand the medical implications of the observed inequalities in health care utilization. On the other hand, this work has many strengths. This is a populational study based on a European population of 1.3 million people. We used data from administrative health data sources combined with electronic health records.





留言 (0)