In children aged 0–11 years old, between 1998 and 2018, poisonings from DWRDs decreased by 33%, while paracetamol poisonings increased by 43%. For all medicinal poisonings combined, no change in incidence rates was demonstrated over the study period. Children living in the most deprived quintile areas were at a 30% increased risk of poisoning compared to children living in the least deprived quintile, for all medicinal poisonings combined. However, this risk was roughly 2-fold for prescribed medication (DWRD) poisoning for children living in the most deprived quintile areas compared to children living in the least deprived quintile, but showed no variation by area-level socioeconomic deprivation for over-the-counter medication poisonings.
Mbeledogu previously showed a decrease of 20% in medicinal poisoning admissions in under-5-year-olds in England from 2000 to 2011 [16]. Our analysis suggests no further reduction in overall medicinal poisoning admissions over time, but when examined by the specific medicines involved, different patterns emerge. Paracetamol poisonings increased over time and poisonings from DWRDs decreased. The authors are not aware of comparable recent data from the UK. One study from the USA has previously shown paracetamol poisonings in children decreasing by 16.7% from 2011 to 2016 [26], while another showed no change in over-the-counter medication poisonings in under-5s from 2001 to 2008 [27]. Two studies using poisoning database data showed increases of up to 200% in opioid poisonings in under-5s in the USA from 1997 to 2012 [27, 28]. While Wang et al., using similar data, showed opioid poisonings in under 6 year olds roughly halved between 2010 and 2018 [29].
The decrease in poisoning admissions in children aged under 5 from DWRDs is contrary to the increase in prescriptions of such medications seen over time in the UK. Among adults, prescriptions for weak opioids nearly doubled from 2005 to 2012 [8], while prescriptions of strong opioids increased four- to six-fold from 2000 to 2012 [8, 30]. There was a 28% increase in antidepressant prescribing among 6–18-year-olds from 2003 to 2013 in Wales [31], and a doubling of antidepressant prescriptions among > 14-year-olds in the UK from 1995 to 2011 [7]. In combination with the increase in paracetamol poisonings demonstrated, these findings suggest that messages relating to safe storage of medicines may be leading to positive changes in behaviour with prescribed medication, but that medications deemed to be ‘weaker’ or ‘less dangerous’, such as paracetamol may be stored less safely.
The deprivation gradient we have shown in admissions for childhood poisonings updates existing evidence from the UK. From 1995 to 97, in the Trent region of England, hospital admissions for medicinal poisonings were shown to be 2.5 times higher in the most deprived, compared to least deprived quintile [10]. Admission data from 2000 to 2011 in England showed a weakening of the deprivation gradient in unintentional poisonings over time, from 2.37 times the risk for children living in the most deprived areas compared to the least deprived in 2000, decreasing to 1.54 times the risk in 2011 [16].
Furthermore, we examined the risk by medicinal substance. Our finding of no deprivation gradient for over-the-counter medications, alongside a 2-fold increased risk for children living in the most deprived areas for the most common prescribed medications (DWRD), suggests medication availability may be a key factor here. Among adults in the UK, there is evidence of a deprivation gradient in prescribing of opioid [8, 21], gabapentinoid [21] and antidepressant [21] medications, with higher prescribing to people living in areas with higher levels of deprivation for each substance.
With evidence that education and the provision of safety equipment improves safe medicines-storage [32, 33], that providing education to families in disadvantaged areas is cost-effective in promoting safe storage of medicines [34], and that safety equipment schemes reduce childhood injuries [35], the current findings would strengthen the argument that measures such as home safety assessments, as recommended by NICE [36], should be targeted at households in areas of higher deprivation.
To our knowledge, this is the largest and most up to date study examining trends in the specific medicinal substances involved in childhood poisonings in the UK. As CPRD has been shown to be broadly representative of the UK population [37], these results should be generalisable to the wider UK and other similar countries. By using routinely collected healthcare data for both outcomes and exposures, we have minimised the risk of recall or reporting bias.
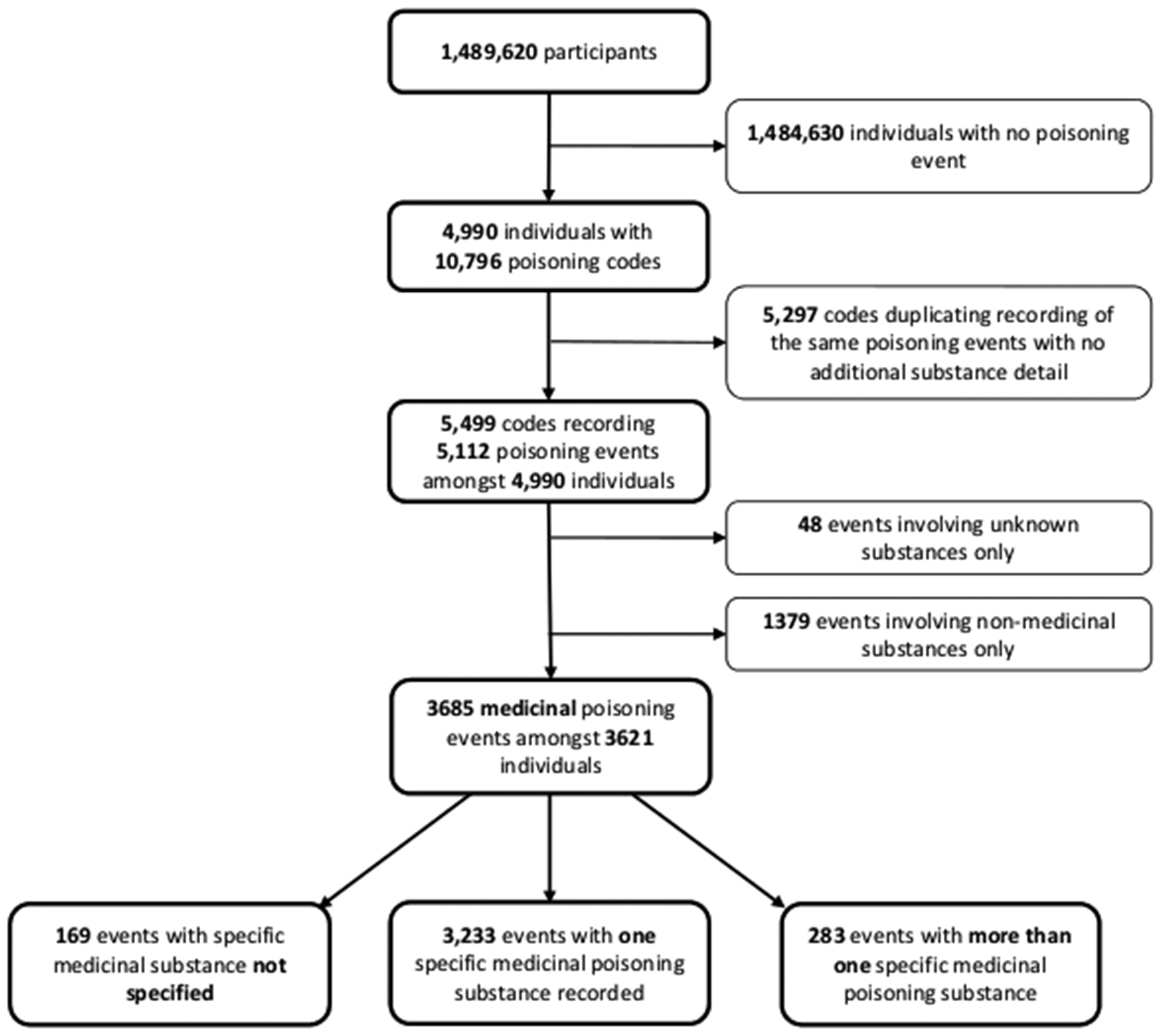
Our study focussed on the three most common groups of medicinal poisonings, which accounted for 59.7% of poisoning events. The substances involved in the remaining poisoning events were very heterogeneous, with small numbers for specific substances as shown in supplementary Table 1, precluding analysis of poisoning incidence rates by age, sex, deprivation and over time. We did not combine these heterogeneous substances into one group for analysis as the implications for prevention vary by substance (e.g. injectable drugs such as insulin, anaesthetic and therapeutic gases, topical agents, drugs most likely to be prescribed for older adults (e.g. cardiovascular drugs prescribed for grandparents)). Whilst there was some missing data in our study, this is unlikely to have had an important impact on our findings as there were only 4.6% of medicinal poisoning events for which the substance wasn’t specified and 0.9% of events where it was not specified if it was a medicinal or non-medicinal poisoning.
We were not able to include poisonings recorded only in primary care data due to insufficiently detailed recording of poisoning substances. We have therefore not captured less severe poisoning episodes, such as those presenting only to the Emergency Department or the GP, without the need for inpatient admission. Therefore, we cannot assume that our findings are generalisable to poisonings not requiring in-patient admission.
Reporting poisoning intent in this study raised some challenges. Previous evidence shows that 92% of poisoning episodes in 0-4-year-olds and 73% in 5-9-year-olds are unintentional [15]. However, the HES codes used to record outcomes in our study usually did not report intent. Therefore, it was not possible for us to report poisoning intent, although existing evidence suggests these episodes would mostly be unintentional poisonings. It was only possible to obtain deprivation data based on the IMD score of an individual’s GP practice address, which may not always accurately represent residence-based deprivation level. Coding accuracy is a potential source of bias in all database studies as data were primarily recorded for clinical and administrative purposes. However, both CPRD [38] and HES [39] have been shown to be valid for a variety of different disease outcomes.
In studies such as this, the categorisation of medications as ‘over-the-counter’ can sometimes be problematic. For instance, a number of medications, such as paracetamol, can be bought over the counter without a prescription in the UK, but can also be prescribed. The medications in the ‘over-the-counter’ group within our study would most commonly be obtained without a prescription, however in some instances these medications may have been prescribed. This does not alter the key messaging around such medications, which is that they can be dangerous if ingested by children and should be stored safely, in a raised, locked cupboard out of the reach of children, in the same way that prescribed medicines, potentially perceived as ‘more dangerous’ should be.
In summary, poisonings from dependence/withdrawal risk drugs have decreased but those from paracetamol have increased, between 1998 and 2018. The higher poisoning incidence among children living in more deprived areas relate to prescribed, rather than OTC medication. This strengthens the argument that households in more socioeconomically deprived areas will have the greatest need for, and potential to benefit from measures to improve safe storage of medicines and these households are likely to require targeted interventions. It is also important that universal promotion of the safe storage of OTC and prescribed medicines is provided by prescribers, community pharmacies and other outlets of such medication.





留言 (0)