Patients and clinical data analysis
We conducted a retrospective analysis of clinical data for newly diagnosed HIV-HL patients aged > 18 years, with a confirmed pathological diagnoses, treated at three medical centers in China, which includes the sixth people’s hospital of Zhengzhou, Peking union medical college hospital, and Chongqing university cancer hospital, from December 2013 to June 2022. Pathological results were re-evaluated by ≥ 2 experienced pathologists. Patient demographics, clinical presentations, laboratory tests, and treatment regimens were systematically analyzed. This study complied with the 2013 revised Helsinki Declaration and informed consent was obtained from all the patients.
Diagnostic criteria and clinical staging
Diagnosis was based on the 2016 World Health Organization (WHO) pathological diagnostic criteria for Hodgkin lymphoma, confirmed through morphological and immunohistochemical analysis. All patients were co-infected with HIV.
Clinical staging was performed according to the 2014 Lugano staging criteria, based on the extent of disease involvement and the presence of B symptoms. B symptoms include: (1) unexplained fever, temperature > 38 ℃ for more than 3 consecutive days, excluding infection; (2) night sweats (soaking clothes); (3) weight loss > 10% of body weight within the six months prior to diagnosis. Patients were divided into groups with or without B symptoms based on their clinical presentation.
Treatment and response assessment
All patients received the ABVD regimen (doxorubicin, bleomycin, vinblastine, and dacarbazine): doxorubicin 25 mg/m2 on days 1 and 15; bleomycin 10 mg/m2 on days 1 and 15; vinblastine 3 mg/m2 on days 1 and 15; dacarbazine 375 mg/m2 on days 1 and 15. The median number of chemotherapy cycles was 5 (ranging from 2 to 12). All patients were administered cART. cART included two nucleoside reverse transcriptase inhibitors and one non-nucleoside reverse transcriptase inhibitor. 18F-fluorodexyglucose positron emission tomography/computed tomography (PET/CT) was performed for radiological evaluation. Treatment response was primarily assessed according to the 2014 Lugano criteria [5], classified as complete response (CR), partial response (PR), stable disease (SD), or disease progression (PD).
Follow-Up
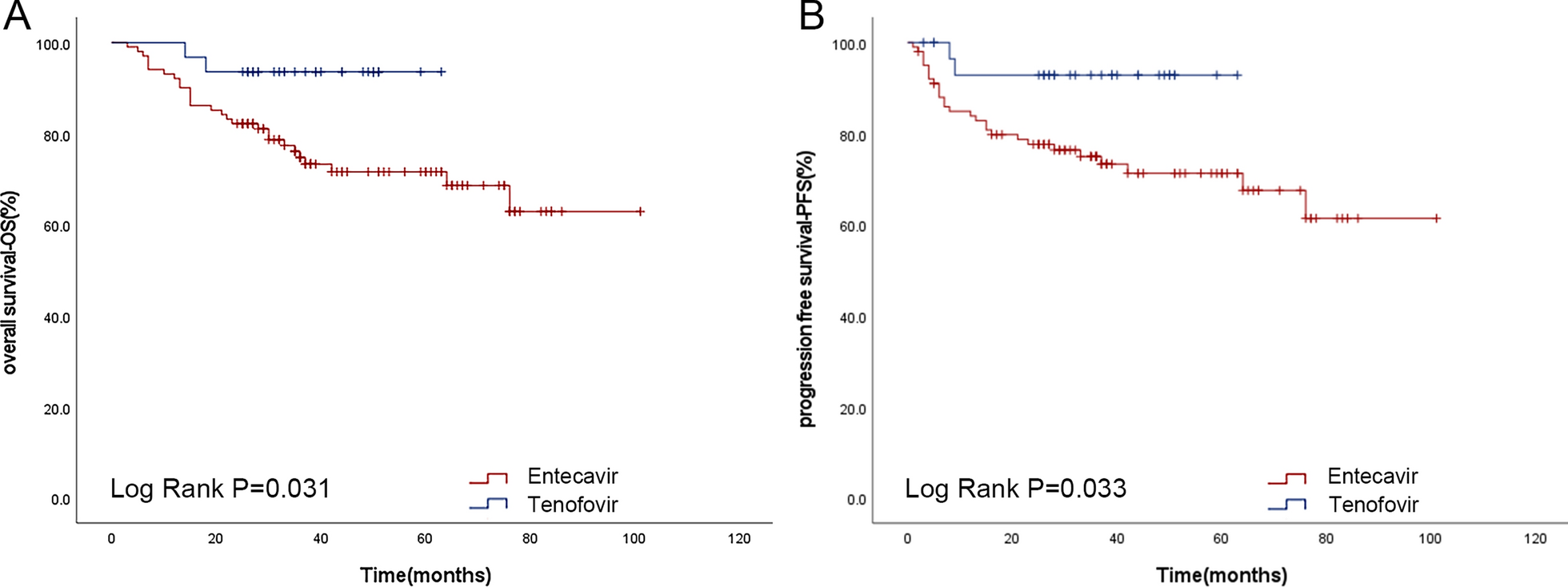
Follow-up was conducted by reviewing inpatient medical records and telephone interviews, with a follow-up cut off date of March 31, 2023, and a median follow-up duration of 46.8 months (ranging from 4.0 to 112.9 months). Progression-free survival (PFS) was defined as the time interval from HIV-HL diagnosis to disease progression, death, or the last follow-up. Overall survival (OS) was defined as the time interval from HIV-HL diagnosis to patient death or the last follow-up.
Statistical analysis
Statistical analysis was performed using SPSS 22.0 software, and graphs were generated using Graph Pad Prism Version 9.0.0. Continuous data were presented as median (range), and categorical data were presented as frequencies (%). Survival analysis was conducted using the Kaplan-Meier method.



留言 (0)