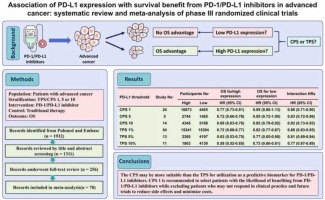
The overall survival (OS) benefit of various antibodies targeting programmed cell death-1 (PD-1) and PD-1 ligand 1 (PD-L1) has been validated in large clinical trials, and their clinical application as standard first-line or subsequent-line therapies in nearly all cancer types has been approved by various countries and regions (Ribas and Wolchok, 2018). However, the response rates to PD-1/PD-L1 inhibitors varied between 15% and 30% in most solid tumors (Das and Johnson, 2019). In addition, even in responders, the magnitude of survival benefit is highly variable (Zhao et al., 2020). Moreover, anti-PD-1/PD-L1 therapy is associated with potentially adverse effects and financial burdens (Kim et al., 2020, Postow et al., 2018). Therefore, several biomarkers, including PD-L1 expression, microsatellite instability, and tumor mutational burden, have been introduced to select cancer patients with the likelihood of benefiting from treatment with PD-1/PD-L1 inhibitors (Sharma et al., 2023). As the rationale for the development of PD-1/PD-L1 inhibitors and because of their convenience and low cost, PD-L1 expression tested by immunohistochemistry (IHC) has been widely used to predict the OS advantage of PD-1/PD-L1 inhibitors in clinical trials (Doroshow et al., 2021). In fact, PD-1/PD-L1 inhibitors were first tested and approved in patients whose tumors expressed high PD-L1 (Doroshow et al., 2021). In recent years, many trials have shown that PD-1/PD-L1 inhibitors are also effective in tumors with low or negative PD-L1 expression; therefore, some PD-1/PD-L1 inhibitors have been approved for patients regardless of PD-L1 expression (Brahmer et al., 2023, Lu et al., 2022, Qin et al., 2023, Wolchok et al., 2022). However, the definition of PD-L1-positive tumor varied across clinical trials, leaving whether PD-L1 tested by IHC is needed to stratify patients before treatment with PD-1/PD-L1 inhibitors as an area of debate. In addition to the spatial and temporal heterogeneity of tumors, variations in PD-L1 expression across clinical trials also arise from diagnostic assays (i.e., 22C3, 28-8, SP263, E1L3N, or SP142), cell subsets evaluated (i.e., tumor cells, infiltrating immune cells, or both), scoring methods (i.e., tumor cell proportion score [TPS], immune cell proportion score [IPS], or combined positive score [CPS]) and thresholds (i.e., 1, 5, 10, or 50) (Vranic and Gatalica, 2023).
Because of this heterogeneity, holistically investigating the association between PD-L1 levels and the efficacy of anti-PD-1/PD-L1 therapy is difficult. Although several reviews and meta-analyses have aimed to determine whether PD-L1 tested by IHC is needed or how to define a PD-L1+ tumor for the most effective selection of patients with the likelihood of benefiting from PD-1/PD-L1 blockade therapy, they are only descriptive or focus on specific cancer types, leaving debates unsettled (Doroshow et al., 2021, Noori et al., 2023, Shen and Zhao, 2018, Xu et al., 2023a). In addition, current approval of one anti-PD-1/PD-L1 agent was based on trials of individual cancer types, which means that even in the same cancer, different anti-PD-1/PD-L1 agents were approved at different PD-L1 cutoff points, making decision-making about which anti-PD-1/PD-L1 agents should be selected for individual patients difficult. Therefore, with the accumulation of available data from large clinical trials, we conducted this comprehensive systematic review and meta-analysis, aiming to examine the association between PD-L1 tested by IHC and the survival benefit of PD-1/PD-L1 inhibitors.



留言 (0)