Breast cancer resistance represents a major challenge to the treatment of breast cancer. The incidence rates of breast cancer have increased significantly over the past few years and breast cancer is the leading cause of cancer death for women worldwide (Organization, 2019). Assays for receptors including estrogen receptors (ER), progesterone receptors (PR) and human epidermal growth factor 2 (HER2) are used to classify the tumors into subtypes and are vital in evaluating therapeutic treatments. For example, patients with tumors expressing estrogen receptors are treated with endocrine therapy and a small portion of these patients also receive chemotherapy. Immunotherapy in combination with certain small molecule inhibitors is used against tumors expressing HER2 receptors. Finally, patients with triple-negative tumors are treated predominantly with chemotherapy (Waks and Winer, 2019, Bray et al., 2015). Rather than a simple disease that involves only few genes, proteins and signaling pathways causing progression, breast cancer is a heterogenous and complex disease with unique morphological and molecular characteristics. Recent studies have shown that patients with the same subtype of breast cancer canrespond differently to a treatment. This indicates a high heterogeneity in this disease. Human cancers, especially breast cancers, are such heterogenous diseases that current treatments leave a significant proportion of patients at risk of over-treatment and a variety of possible side effects.
Gene expression profiles, identification of tumor heterogeneity and molecular classification of breast cancer have become possible due to the advent of molecular techniques such as RNA sequencing. So far, six subtypes of breast cancer have been identified. Their classification is based on the expression of estrogen-associated genes, estrogen receptor, progesterone receptor, genes associated with progression and proliferation such as HER2 and other associated genes in the chromosome 17 region (Harbeck et al., 2019). Luminal A and luminal B, ER+ tumors with the expression of epithelial markers, HER2+ or HER2- enhanced tumors where the HER2 gene is overexpressed, triple negative breast cancer (TNBC) characterized by the lack of ER, PR and HER2 expression, and claudin-low that is enhanced in epithelial-to-mesenchymal transition (EMT) features represent the six subtypes of breast cancer (Prat et al., 2010). However, some researchers recognize only five subtypes and do not consider claudin-low a subtype.
New marker identification is necessary not only for improved diagnosis but also for prognosis and improved patient response. This is essential since breast cancer is a heterogenous disease and each patient has different and individual characteristics. The treatments for breast cancer are also specific for the subtype by targeting the molecular targets that are functionally altered in the specific subtype. In addition to chemotherapy the predominant type of treatment for the tumors with hormone receptors (ER and PR) (luminal A and luminal B) is endocrine therapy (Parisot et al., 1999, Berry et al., 2000). Endocrine therapy works by interfering with the activity of hormones such as estrogen and progesterone and thus helps to inhibit the growth of hormone receptor-positive breast cancer. There are several different types of endocrine therapies that may be used individually or in combination, depending on the specific characteristics of the breast cancer and the patient's overall health. Some of the commonly used endocrine therapies for breast cancer are included (Fan et al., 2015):
Selective Estrogen Receptor Modulators (SERMs): such as tamoxifen, work by binding to the estrogen receptors in breast cancer cells, thereby blocking their growth (An, 2016).
Aromatase Inhibitors (AIs): including drugs like letrozole, anastrozole, and exemestane,work by blocking the enzyme aromatase, which is responsible for converting androgens into estrogen. By reducing the production of estrogen AIs help to suppress the growth of hormone receptor-positive breast cancer cells (Bahrami et al., 2020, Geisler et al., 2008).
Luteinizing Hormone-Releasing Hormone (LHRH) agonists: such as goserelin and leuprolide, are commonly used in premenopausal women to suppress the production of estrogen by the ovaries. These drugs work by temporarily shutting down ovarian function, leading to a decrease in estrogen levels and thereby inhibiting the growth of hormone receptor-positive breast cancer cells (Lu et al., 2021).
Selective Estrogen Receptor Down regulators (SERDs), such as fulvestrant, work by binding to estrogen receptors and targeting them for degradation, effectively reducing the number of available estrogen receptors in breast cancer cells. This leads to the inhibition of cancer cell proliferation (Shagufta et al., 2020).
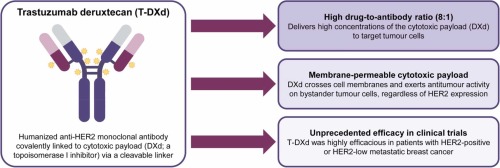
Endocrine therapy may be used as adjuvant therapy after surgery to reduce the risk of cancer recurrence or as the primary treatment for advanced or metastatic breast cancer (Fan et al., 2015).Monoclonal antibodies and tyrosine kinase inhibitors that recognize the HER2 receptor (extracellular domain) (trastuzumab and lapatinib) along with RNAi-mediated silencing are used for HER2 positive tumors (Tai et al., 2010). Trastuzumab (Herceptin) is a well-known monoclonal antibody that specifically targets the extracellular domain of the HER2 receptor. It works by binding to the HER2 protein on the surface of cancer cells, which impedes the receptor's activity. Trastuzumab can directly induce antibody-dependent cellular cytotoxicity (ADCC), leading to the destruction of HER2-positive breast cancer cells by the immune system. It can also inhibit the downstream signaling pathways of HER2, thus reducing cell proliferation and promoting apoptosis of cancer cells (Vu and Claret, 2012).
Lapatinib (Tykerb) is an example of a tyrosine kinase inhibitor that targets the HER2 receptor. It acts by blocking the intracellular domain of both HER2 and EGFR (epidermal growth factor receptor). By inhibiting the tyrosine kinase activity of these receptors, lapatinib disrupts the signaling pathways responsible for cell growth and survival (Opdam et al., 2012).
Potential therapeutic targets for antibody drug conjugates (ADCs) in breast cancer, including HER2, TROP-2, PTK7, and LIV-1. LIV-1, a transmembrane protein associated with estrogen-induced gene expression and epidermal-to-mesenchymal transition, is expressed in moderate/high levels in most breast cancers. Clinical trials, including those for the ADC ladiratuzumab vedotin targeting LIV-1, have shown promising activity in breast cancer patients, either as monotherapy or in combination with other agents, including immune checkpoint inhibitors (Rizzo et al., 2022a).
RNA interference (RNAi) is a mechanism that can be utilized to silence specific genes and their expression. In the context of HER2-positive breast cancer, RNAi can be used to target and inhibit the production of HER2 receptor protein. Small interfering RNA (siRNA) molecules can be designed to specifically bind to and degrade the mRNA molecules that code for HER2. This prevents the translation of HER2 mRNA into protein, effectively reducing the amount of HER2 receptor available on cancer cells. RNAi-mediated silencing can be achieved through various delivery methods, including nanoparticle-based systems or viral vectors (Faltus et al., 2004). Sometimes endocrine therapy is also used for HER2 tumors with positive hormone receptors. The conventional mode of treatment for TNBC is chemotherapy. and lately several research groups have identified molecular targets including epidermal growth factor (EGFR), androgen receptor (AR), poly-(ADP-ribose)-polymerase (PARP) and vascular endothelial growth factor (VEGF).
Other treastments have been explored in addition to conventional treatments such as endocrine therapy, targeted therapy and chemotherapy. These include cyclin-dependent kinase 4/6 (CDK 4/6) inhibitors, immunotherapy, microRNAs (miRNAs), clustered regularly interspaced short palindromic repeats (CRISPR), tyrosine kinase inhibitors (TKIs), drug repurposing, electrochemotherapy, and nanotechnological approaches (Fig. 1). These conventional approaches paired with new treatment strategies can offer significant benefits by overcoming resistance and mitigating side effects. Rizzo et. al., discusses the challenges in treating triple-negative breast cancer (TNBC) despite advancements. Immune checkpoint inhibitor (ICI) monotherapy showed effectiveness in a small group of metastatic TNBC patients, supporting further exploration. Chemoimmunotherapy is emerging as a first-line treatment, and ongoing clinical studies may reshape TNBC treatment, emphasizing the importance of identifying biomarkers for treatment response prediction (Rizzo et al., 2022b). A recent meta-analysis examined sex-related differences in response to immunotherapy, revealing slight variations in antitumor efficacy between male and female patients. This study, considered the most updated and comprehensive on the topic, emphasizes the significance of addressing and discussing the underexplored aspect of sex-driven differences in immune checkpoint inhibitors' efficacy (Santoni et al., 2022). Similarly, a research group conducted a MOUSEION-03 study a meta-analysis to assess the possibility of achieving complete remissions (CR) with immunotherapy in cancer patients. Analyzing 85 randomized studies with 49,425 patients, the study found that the use of immune checkpoint inhibitors (ICIs), either alone or in combination with other agents, significantly increased the likelihood of achieving CR compared to control treatments. The highest odds ratio for CR was observed in immune-based combinations with two ICIs. The study highlights the potential of ICIs to enhance complete remissions rates in various solid tumors (Santoni et al., 2023).



留言 (0)