Individuals exhibiting mild-to-moderate cholestasis in the context of MASLD presented diverse signs and clinical features compared to those with a hepatocellular pattern, showing additional important issues regarding diagnosis and prognosis. In this setting, some relevant aspects must be emphasized. First, the cholestatic pattern was shown as often as the hepatocellular pattern in the overall MASLD cohort. Second, individuals showing a hepatocellular pattern had more necroinflammatory activity in the histology compared with those with a cholestatic pattern, whilst this latter showed more frequently cirrhosis. Third, the accuracy of NITs detecting advanced fibrosis, particularly FIB-4, and HFS, was decreased in the presence of a hepatocellular pattern. And fourth, the prognosis was worse in patients with a predominant cholestatic pattern. Therefore, we should consider different MASLD phenotypes according to the biochemical presentation, which is easy to identify, with significant consequences for the making-decision process in clinical practice.
MASLD is an entity typically associated with a hepatocellular pattern; this is a predominant elevation of transaminases (AST and ALT) instead of enzymes of cholestasis (particularly ALP). In this setting, little is known about the prevalence of the cholestatic pattern in MASLD. About an one-fourth of patients in the HEPAmet registry (one of the largest registries worldwide) showed a cholestatic pattern, whilst other studies have reported between 27 and 43% [6, 16]. Besides, we observed some baseline features that differ between the patterns beyond the liver profile. Interestingly, the cholestatic pattern was associated with older age and higher BMI, and individuals showing a hepatocellular pattern had higher levels of triglycerides, cholesterol, and glucose, despite the rates of metabolic conditions (i.e. T2DM or arterial hypertension) were similar. While the association between age and BMI with the cholestatic pattern has been reported previously, the relationship between a worse control of metabolic factors and the hepatocellular pattern is novel [6, 16, 17]. This latter could be explained, at least in part, by the fact that some metabolic conditions (such as T2DM) can promote liver inflammation [18].
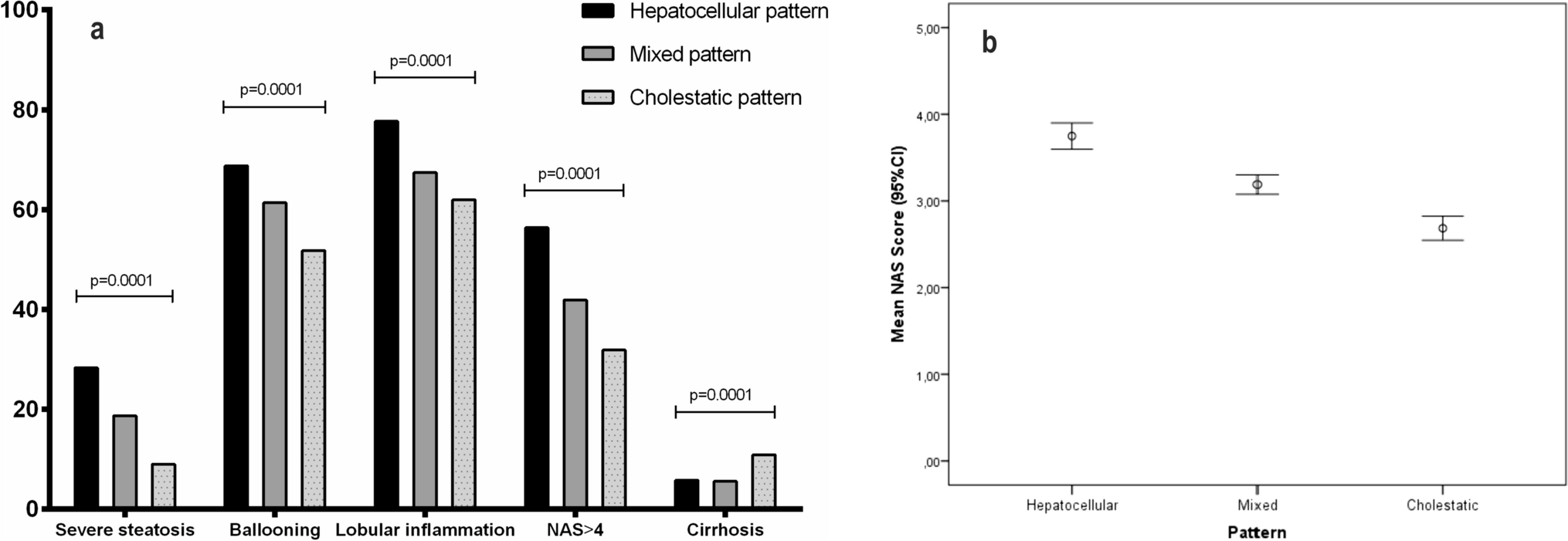
The cholestatic pattern has been associated with a higher liver fibrosis stage by an Italian study in 582 patients (only 435 with biopsy-proven MASLD) [6] and an Israeli study in 106 patients [16]. However, they evaluated neither ballooning nor lobular inflammation in the liver biopsies. Our study represents the largest cohort (n = 2156) of biopsy-proven MASLD patients evaluating the histology depending on the biochemical pattern. In this setting, we observed that the single components of NAS (steatosis, lobular inflammation, and ballooning) were significantly more frequent in patients with a hepatocellular pattern, and, consequently, they had higher NAS and more presence of MASH. These findings are not surprising, given that this pattern is defined by a predominant elevation of ALT and AST, which usually has been associated with a higher necro-inflammation in the histology. By contrast, patients with a cholestatic pattern doubled the risk of cirrhosis compared to the mixed and hepatocellular pattern, and, probably, this fact explains the lower percentage of MASH [19] and albumin levels in the presence of cholestasis. Cholestasis secondary to chronic liver injury may denote a more severe disease course and development of end-stage liver disease [20]. In a small subgroup of subjects stratified for these patterns, a significant down-expression of NR1H3, RXRα and VCAM 1 genes was found in patients with cholestatic compared to those with the hepatocellular pattern [6]. Thus, a MASLD patient with a cholestatic pattern, despite showing normal transaminases, should be monitored to look for advanced fibrosis more carefully than others.
The role of the biochemical pattern on the prognosis of MASLD patients has not yet been assessed. An Italian study observed a higher risk of decompensated events in patients with a cholestatic pattern (considering that they included cirrhotic patients diagnosed by clinical features) [6]. At the same time, no studies have assessed the impact on mortality or the dynamic changes of the biochemical patterns over time. In our study, more than 1,700 patients were followed-up to evaluate these questions. First, we observed that patients with a hepatocellular pattern showed lower rate of decompensated cirrhosis, in both the overall and the cirrhotic cohorts, than in the absence of it. Second, we observed that the cholestatic pattern was independently related to higher mortality, together with older age, and the presence of T2DM and cirrhosis. Interestingly, the annual incidence of mortality was three times higher in patients with predominant ALP levels compared to those with a hepatocellular pattern. Third, we observed that patients with initial and/or final hepatocellular pattern showed about 1% of mortality during the follow-up, whilst patients with initial and/or final cholestatic pattern died around 6%. Of note, the leading cause of mortality was similar between the groups despite the hepatocellular pattern had more prevalence of MASH (typically associated with higher cardiovascular-related mortality [21]) and patients with a cholestatic pattern had more prevalence of cirrhosis (usually related to liver-related mortality [22]).
The use of NITs, including FIB-4, HFS, and NFS, is recommended in clinical practice by international guidelines [23,24,25]. Despite they have robust thresholds to detect advanced fibrosis [26], there are some circumstances, such as age, in which they must be modified to increase the specificity or the sensitivity [27]. The impact of the biochemical pattern on the accuracy of NITs has not been assessed yet in MASLD patients. Overall, FIB-4 and HFS were superior to NFS in detecting advanced fibrosis. However, we observed a significantly decreased accuracy for FIB-4 and HFS in patients showing a hepatocellular pattern. Of note, the identification of advanced fibrosis in patients above the higher threshold was particularly affected and significantly decreased compared to those without a hepatocellular pattern. These results should make us to reconsider the higher cut-offs for FIB-4 and HFS to avoid a relevant number of patients with false positive results. On the other hand, we also included patients who underwent transient elastography, although the biochemical pattern did not affect this technique.
We must recognize that the current study shows some limitations. First, despite collecting all the patients’ medications for the different comorbidities, we cannot exclude completely that some could show a drug-induced cholestatic pattern. However, the fact of including more than two thousand patients and selecting a high specificity ALP/ALT ratio decreases this likelihood dramatically. Second, the dynamic changes in the biochemical pattern were assessed in half of the longitudinal cohort. However, we consider valuable this exploratory analysis (very few patients transiting from a hepatocellular to a cholestatic pattern or vice versa) because there are no published data about the durability of the pattern in MASLD. And third, this study was not designed to perform any experimental approach to explain the underlying mechanisms of cholestasis in MASLD. However, two studies have previously identified specific features in patients with this pattern, including morphological changes and a different gene expression [6, 17]. Some drugs are being tested simultaneously for MASLD and primary biliary cholangitis (i.e. obeticholic acid, elafibranor) with a suboptimal efficacy in the presence of fatty liver, so working on the biological plausibility of some grade of cholestasis in MASLD is very attractive.
In conclusion, the current study lights different MASLD phenotypes that the biochemical pattern could easily identify. Selecting patients to undergo biopsy and anticipate liver damage, carefully monitoring at-risk patients of cirrhosis and decompensation, or receiving personalized experimental therapy in the setting of clinical trials are some of the potential clinical consequences of our research. Further studies are warranted to confirm these results and, mainly, to analyze the underlying mechanisms that explain the clinical differences between the MASLD phenotypes and guide to a specific therapeutic approach.


留言 (0)