
記住我



LNC with and without SEMA were prepared using generally recognized as safe (GRAS) excipients, and their composition is described in Table 1. The phase inversion method was performed as previously described [9]. The average size obtained was ~188.3 ± 3.40 nm, with a homogeneous population of nanoparticles (PDI < 0.2) and a negative surface charge (-9.6 ± 2.34 mV). The encapsulation efficiency of SEMA was 90.5 ± 0.82% (Table 2). Representative images of both RM-LNC and SEMA-RM-LNC are depicted in Supplementary Information Fig. S1.
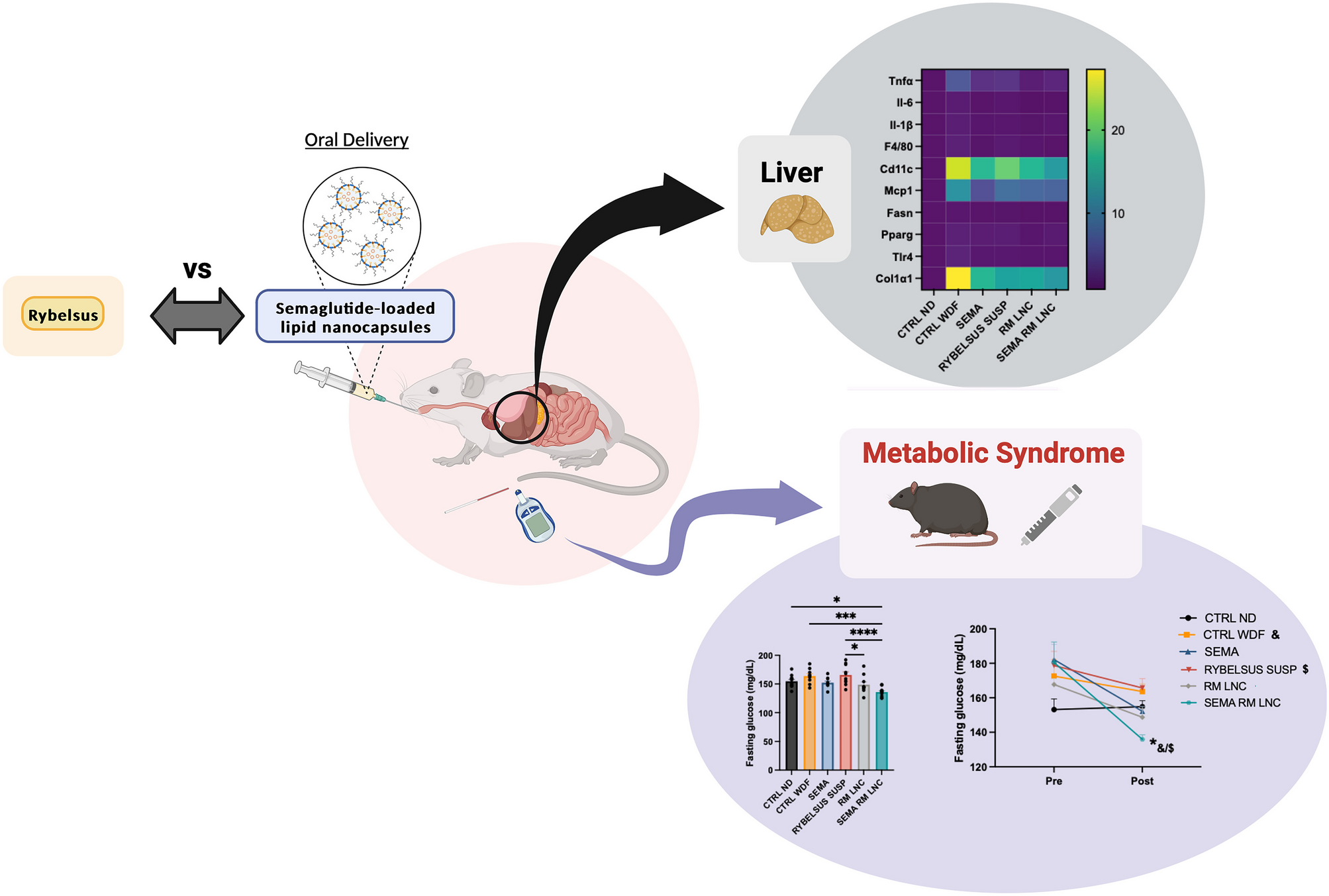
Table 2 Physicochemical properties of semaglutide-loaded lipid nanocapsules (PDI: polydispersity index; EE: encapsulation efficiency (n=3))SEMA-RM-LNC had a greater impact on the metabolic syndrome associated with MASLD than EXE-RM-LNC, RM-LNC and Rybelsus®To assess the effectiveness of our treatment strategy in MASLD, an in vivo experiment in which C57BL/6 J mice were fed a western diet plus fructose in the drinking water (WDF) for 20 weeks was conducted. During the induction period of the disease, several parameters were analyzed: body weight gain, fasting glycemia, fasting insulin levels and HOMA-IR score. After 20 weeks of diet intake, the mice fed a WDF were obese with a weight gain of 24.60 ± 0.43 g compared to a 11.27 ± 0.52 g in the mice fed a normal rodent diet (ND).The average glycemia levels were 176.4 ± 3.86 mg/dL in the WDF group and approximately 153.2 ± 6.17 mg/dL in the ND group. Insulin levels were also significantly higher in the WDF-fed mice than in the ND-fed mice (ND: 1.060 ± 0.1 ng/mL vs. WDF: 2.027 ± 0.13 ng/mL). Similarly, the homeostatic model assessment of insulin resistance (HOMA-IR) was calculated, indicating the presence of insulin resistance, which is characteristic of MASLD and a major driver of the disease. The results are presented in the supplementary information (Fig. S2). The mice were then randomized into the different treatment groups to form body weight-matched groups (Supplementary information Fig. S3). After the 20 weeks, a 4-week daily chronic treatment was conducted, with daily gavage of either water, SEMA in solution, Rybelsus® in suspension, RM-LNC (no SEMA) or SEMA-RM-LNC (500 μg/kg). In the clinic, semaglutide is given in 3 mg, 7 mg, or 14 mg doses. During this period, both fasting and non-fasting glycemia were assessed, and the body weight was controlled daily (Fig. 1A).
Fig. 1
SEMA-RM-LNC has a greater impact on the metabolic syndrome than RM-LNC and Rybelsus® under non-fasting conditions throughout the one-month treatment. A Schematic representation of the treatment period of 4 weeks, B Body weight (%), C Pre/Post: Body weight (%), D Body weight change (%), E Non-fasting glucose (%), F Pre/Post: Non-fasting glucose (%), G Non-fasting glucose change (%), H Active GLP-1 levels (pg/mL) measured in portal plasma, I Total GLP-1 levels (pg/mL) measured in cava plasma. Pre: beginning of treatment; Post: end of treatment. The results in D, G were calculated by subtracting the post values from the pre values. P values in H, I were determined by One-way Anova followed by Tukey’s post hoc test or the Kruskal-Wallis followed by Dunn’s post hoc test (*P < 0.05, **P < 0.01, ****P < 0.0001). The data are presented as the mean ± SEM (n = 9–10)
A 5 to 10% weight loss can lead to MASH resolution in humans [4] and in rodents [16]. In our study, all mice lost between 1 and 5% of their body weight, with no significant difference between the groups during the 4-week treatment period (Figs. 1 and S4), which is relatively short compared to the 48–72 week treatment period performed in clinical trials. Glycemia was measured under 2 different conditions: non-fasting glycemia was measured weekly, and fasting glycemia was measured before and at the end of the treatment period. Regarding non-fasting glycemia, although statistical significance was not observed, a positive trend was observed with SEMA-RM-LNC when compared to the other groups tested. Moreover, it should be highlighted that SEMA-RM-LNC had a better trend than SEMA ORAL, RYBELSUS SUSP and RM-LNC and better than our exenatide-loaded lipid nanocapsules (EXE-RM-LNC), which were used in our previous studies [10]. SEMA-RM-LNC decreased glycemia levels by approximately 14.2 ± 4.04% while glycemia levels in the other groups decreased by 6.7 to 8.3% (Figs. 1E–G and S4). In this study, we observed a better trend for glucose reduction with SEMA-RM-LNC than with the nanoparticles alone (Fig. 1E–G). We observed significant differences in the fasting glycemia values on the last week of treatment (POST), as mice treated with SEMA-RM-LNC exhibited a significantly lower fasting glycemia than almost all other groups, with almost normalized glycemia (Fig. 2B). The results from before and those at the end of the treatment period were compared and designated as PRE and POST, respectively. Significant differences in fasting glucose were detected between our strategy group (SEMA-RM-LNC) and the CTRL WDF and Rybelsus suspension group when comparing the PRE and POST results (SEMA-RM-LNC: 135.9 ± 2.59 mg/dL vs. CTRL WDF: 163.7 ± 4.36 mg/dL vs. Rybelsus: 165.7 ± 5.48 mg/dL) (Fig. 2E). Despite observing an effect on glycemia, we did not observe significant differences in the insulin (Fig. 2F) or HOMA-IR (Fig. 2G). This finding supports our hypothesis that a peptide with a long half-life might be more efficient in the context of MASLD treatment.
Fig. 2
SEMA-RM-LNC has a greater impact on the metabolic syndrome than EXE-RM-LNC, RM-LNC and Rybelsus® under fasting conditions throughout the one-month treatment A Schematic representation of the conduction of experiments under fasting conditions, B Fasting glucose (mg/dL), C Fasting insulin levels (ng/mL), D Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) calculated using the equation [fasting glucose (mg/dL) x fasting insulin (ng/mL)/405], E Pre/Post: Fasting glucose (mg/dL), Pre/Post: Fasting insulin levels (ng/mL), G Pre/Post: HOMA-IR, H Fasting glucose change. The results in H were calculated by subtracting the post values from the pre values. P values in B were determined by One-way Anova followed by Tukey’s post hoc test. P values in E were determined by Two-way Anova followed by Tukey’s post hoc test (*P < 0.05, ***P < 0.001, ****P < 0.0001). The data are presented as the mean ± SEM (n = 9–10)
LNC can induce the secretion of the native GLP-1 when orally administered. This effect was previously demonstrated in a MASLD mouse model [10]. We further confirmed this by measuring GLP-1 levels in the portal blood 1 h after the gavage of fasted mice. We chose to measure it in the fasting state to avoid the interference with food intake, which can be modulated by the treatment itself. No significant differences in the levels of active GLP-1 were detected, but there was a trend toward higher levels of GLP-1 in the RM-LNC and SEMA-RM-LNC groups (Fig. 1H). In a previous study, we showed that empty LNC significantly increased the GLP-1 levels. The experimental conditions varied between the 2 studies, which may explain the difference. Indeed, here we measured levels 1 h after gavage, while in the previous study, we measured levels 30 min after treatment, and 30 min after an oral glucose load [10]. We did observe significant differences in total GLP-1 levels in systemic circulation, which were found to be higher in WDF animals than in control healthy animals but with no difference according to treatment. (Fig. 1I).
SEMA-RM-LNC impact on liver steatosis and inflammation in early MASLDRegarding the effect observed in the liver, we analyzed several markers relevant to the disease setting. We measured liver weight, liver transaminases (ALT and AST) and liver lipid content. Compared to those in the control group (CTRL ND), feeding mice WDF increased all these parameters, but we did not observe significative differences according to treatment (Fig. 3A–D). Aminotransaminase levels can be used as biomarkers for disease onset and consequent progression or amelioration because they indicate hepatic injury; however, their use in MASLD is not always specific. Alanine transaminase (ALT) tends to increase in MASLD and aspartate aminotransferase (AST) decreases; however, as the disease progresses to cirrhosis this ratio can reverse [17]. Several biomarkers are being investigated as possible and better indicators of disease progression with the aim of replacing the standard of diagnosis, which remains an invasive procedure (biopsy) [4, 18]. Histological liver slides were analyzed and scored for the presence of steatosis (% of tissue presenting steatosis), lobular inflammation (inflammatory cell infiltrates, foci, into the liver parenchyma) and ballooning (hepatocellular injury) [19]. In Fig. 3E, the NAS score is represented as the sum of these 3 features, with no significant differences between the groups fed a WDF. The NAS score was broken down and in the ballooning score, Rybelsus group was the only group with significant differences with all the other groups fed a WDF. Regarding the fat storage in the liver, histology (Fig. 3H), liver weight (Fig. 3A) and liver lipid content (Fig. 3D) confirmed that none of the treatments reduced steatosis, possibly due to the short duration (4 weeks) of treatment. Furthermore, in addition to a diet rich in fat and cholesterol, this model also contains 30% of fructose in the drinking water. Fructose, which is not metabolized via the same pathways as glucose, can increase de novo lipogenesis and further increase the fat storage in the liver [20, 21]. Several studies have shown the ability of GLP-1 analogs to reduce de novo lipogenesis, likely through indirect mechanisms [22]. However, this deserves further exploration.
Fig. 3
SEMA-RM-LNC has a similar effect on lipid homeostasis than EXE-RM-LNC, RM-LNC and Rybelsus®A Liver weight (g), B ALT levels (U/L) measured in systemic plasma, C AST levels (U/L) measured in systemic plasma, D Total lipid content per whole liver, E Histological NAFLD activity score (NAS), F Steatosis, ballooning and lobular inflammation individual scores, G Inflammatory foci per 20× field, H Representative H&E liver sections (scale bar: 100 μm). P values were determined by One-way Anova followed by Tukey’s post hoc test or Kruskal-Wallis followed by Dunn’s post hoc test. P values in F were determined by Two-way Anova followed by Tukey’s post hoc test (*P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001). The data are presented as the mean ± SEM (n = 9–10)
In this study, we did not observe the effects of the treatments on the number of liver inflammatory cells (foci) (Fig. 3F, G). To determine the type of immune cell infiltrating the liver tissue, we conducted an immunohistochemistry assay to detect the presence of neutrophils. In chronic inflammatory diseases, such as MASLD, immune cells, including neutrophils, which are absent in the healthy tissue, are recruited to the liver. The role of these immune cells is not fully understood; however, they release toxic compounds, such as myeloperoxidase, which triggers additional production of reactive oxygen species, cytokines, and neutrophil extracellular traps (NETs), further aggravating the disease setting and progression [23]. In vivo studies revealed that mice lacking neutrophil elastase or myeloperoxidase had less liver damage. Furthermore, hyperglycemia seems to predispose neutrophils to produce more extracellular traps [24]. This ongoing cycle of damage contributes to further development of the disease, activating previously dormant hepatic stellate cells and initiating a fibrogenic state [23, 24]. The results showed that RM-LNC alone had a promising effect on neutrophil infiltration, as both RM-LNC and SEMA-RM-LNC were the only groups that were not significantly different from the CTRL ND group (RM-LNC: 0.024 ± 0.005% LY-6G+ area; SEMA-RM-LNC: 0.019 ± 0.006% LY-6G+ area; CTRL ND: 0.0016 ± 0.0003% LY-6G+ area) (Fig. 4A, B). Our nanoparticle group demonstrated superior enhancement in the management of metabolic syndrome, coupled with a more notable reduction in the levels of certain inflammatory markers, than the groups treated with semaglutide alone. Although further validation is needed, it is noteworthy that mice treated with semaglutide alone exhibited greater neutrophil infiltration. This can be attributed to the limited impact of semaglutide on both metabolic syndrome and the inflammatory state in the liver, unlike our treatment.
Fig. 4
SEMA-RM-LNC reduces inflammation and infiltration/recruitment of immune cell populations in the liver A Representative LY-6G staining of liver sections per group (scale bar: 50 μm) B Quantification of neutrophils in liver sections, C Heatmap representation of the relative mRNA expression normalized to the CTRL ND group. P values were determined by One-way Anova followed by Tukey’s post hoc test or by Kruskal-Wallis followed by Dunn’s post hoc test (*P < 0.05, ****P < 0.0001). The data are presented as the mean ± SEM (n = 9–10)
To further assess the impact of our treatment on disease progression we conducted qPCR assays analyzing key markers of immune cell infiltration, cytokine expression, endotoxin-mediated inflammation, lipid metabolism and fibrosis. Promising results were obtained at ameliorating inflammation with both RM-LNC and SEMA-RM-LNC (Figs. 4C and S5). Significant differences were detected between our SEMA-RM-LNC group and the diseased control group (CTRL WDF) in terms of the expression of markers related to cytokines (Il-6: *P = 0.0247), immune cell infiltration (F4/80: *P = 0.0334 and Cd11c: no significant differences with the CTRL ND), endotoxin-mediated inflammation (Tlr4: ****P < 0.0001) and fibrosis (Col1α1: *P = 0.0122) (Supplementary Information Fig. S4).
qPCR analysis revealed that the RM-LNC group exhibited results similar to those of the SEMA-RM-LNC group. Markers related to cytokine expression (Il-6: **P = 0.0062; Il-1β: **P = 0.0062), endotoxin-mediated inflammation (Tlr4: ***P = 0.0002), lipid metabolism (Pparg: **P = 0.0099) and fibrosis (Col1α1: *P = 0.0372) significantly differed between the RM-LNC group and the CTRL WDF group (Supplementary Information Fig. S5). Based on the literature, components present in lipid nanocapsules, such as phosphatidylcholine (PC), can have a therapeutic effect on the liver, mainly in hepatic steatosis [2, 25, 26]. PC is considered an essential phospholipid and its administration in preclinical and clinical studies has shown positive effects for reducing steatosis by increasing levels of polyunsaturated fatty acids and reducing the LDL/HDL ratio and TG levels [27,28,29]. In the context of MASLD, PC primarily contributes to enhancements in plasma lipid profiles, transaminase levels, and the inhibition of fat accumulation. Additionally, the use of PC has been associated with the downregulation of genes associated with pro-inflammatory macrophages, such as IL-6 [30]. The amount of LNC that reaches the liver after oral administration is currently unknown. However, we can hypothesize that if a significant amount of LNC ends up in the liver, and the components of the formulation do contribute to ameliorating the disease, further combined with their effect on GLP-1 secretion, this could explain the significant effect observed in liver inflammation and immune cell infiltration. Alternatively, as shown in Fig. 1H, the stimulation of GLP-1 release by the RM-LNC may alone explain this observation. Furthermore, the activation of the central nervous system by GLP-1 and GLP-1 analogs has been shown to reduce TLR-mediated inflammation which can explain the significant differences observed in the TLR4 marker analyzed by qPCR [31].
Overall, we observed a significant impact on glucose homeostasis with the SEMA-RM-LNC group (post-treatment) when compared to that of the other treatment groups. We did observe a greater impact on liver inflammatory markers such as F4/80, Cd11c, Il-6, Tlr4 and Col1α1 in the experimental group than in the CTRL WDF group. However, the magnitude of the effects was insufficient to significantly impact the liver weight, NAS score or liver histology. We can speculate that the treatment period is too short (4 weeks) and that prolonged treatment would be needed to yield a tangible positive effect, as reported by the 48 to 72 week long clinical trials [7, 8]. Moreover, the effect expected in the liver is thought to be indirect due to the lack of GLP-1 receptors in the liver. This possibly explains the non-significant effect of our treatment on some of the parameters analyzed and longer periods of treatment might be needed to start showing an effect. However, we believe that, considering the short period of administration, these results are promising towards the amelioration of the inflammatory state and glucose homeostasis. Further analysis can help us better understand the effect observed. For example, the evaluation of the inflammatory state present in the adipose tissue could be a good indicator of disease amelioration. Improving glucose homeostasis and reducing insulin resistance can initiate a decrease in the inflammatory state within adipose tissue. This, in turn, results in the release of fewer fatty acids into the bloodstream, mitigating their accumulation in the liver and subsequently reducing hepatic steatosis [2, 32]. Furthermore, determining whether the effect could be model specific, particularly considering the pro-lipogenic effect of fructose, which could mask a more subtle effect, will be important.
留言 (0)