
記住我
This retrospective case series study was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology, China. Before any study procedures were conducted, all patients or their guardians were informed about the available treatment options, and written informed consent was obtained for the procedures.
Over the period from March 2018 to June 2023, a total of 105 patients with CTPV were treated at our center. The majority of patients experienced relief from symptoms of portal hypertension (such as abdominal pain, bleeding, or ascites) following the administration of anticoagulants, endoscopic treatment, TIPS, or splenectomy/splenic embolization. Patients who have failed traditional treatments (including portal vein recanalization, TIPS, endoscopic treatment), experience recurrent bleeding or refractory ascites despite receiving traditional treatments, or refuse to undergo the traditional treatments, are considered eligible candidates for Transjugular Extrahepatic Portosystemic Shunt (TEPS). During this period, this study consecutively enrolled 22 eligible patients with CTPV, all of whom experienced complete PV obstruction where the obstruction in the MPV exceeded 90% or the MPV trunk was replaced by fibrous cords.
In 22 patients, 20 had concurrent cirrhosis, while 2 did not have a cirrhotic background. The diagnosis of cirrhosis was primarily established through a comprehensive evaluation using clinical, radiological, and histopathological criteria. Clinical criteria included evidence of chronic liver disease, such as prolonged jaundice, hepatomegaly, ascites, or hepatic encephalopathy (HE). Radiological criteria involved imaging studies, such as ultrasound, CT scans, or MRI, demonstrating characteristic features of cirrhosis, such as nodular liver surface, splenomegaly, or signs of portal hypertension. Histopathological confirmation was obtained through liver biopsy or surgical specimens in selected cases.
Among the 22 cases, 13 patients experienced recurrent bleeding following traditional treatment, eight had recurrent/refractory ascites, and one had acute bleeding but declined endoscopic treatment. The demographic and disease status of the included patients in this study are shown in Tables 1 and 2.
Table 1 Baseline characteristics of patients undergoing TEPS for CTPVTable 2 Pre-TEPS details of patientsTEPS procedurePatients underwent abdominal enhanced computerized tomography and 3D reconstruction of the portal venous system within 7 days before the TEPS procedure to evaluate the location and degree of PV obstruction and to perform a preliminary assessment of the surgical and guidance methods that may be used during the procedure. Additionally, preoperative CT examinations allow us to evaluate the anatomical relationship among the inferior vena cava, major biliary radicals, organs, and adjacent portal collaterals. This information aids in planning the surgical procedure and identifying potential areas of concern. The TEPS procedure was performed on all patients by the same experienced surgical team (LWF, ZCZ, CDL, and ZYJ) under either local or general anesthesia (for those undergoing transmesenteric vein shunt).
Based on preoperative imaging evaluation and under ultrasound guidance, a percutaneous transhepatic puncture was carried out on the portal venous tributary within the liver. A 5F/6F catheter sheath was then inserted to explore the PV leading to the superior mesenteric vein (SMV) or splenic vein (SV). If entry to the PV or SMV/SV was not successful via a percutaneous transhepatic route, SV splenic tributary was punctured under ultrasound guidance. Subsequently, the catheter wire was directed to the PV or SMV/SV for portal venography. This was done to further confirm the puncture site of the PV and the shunt pathway as well as to measure the PVP. The PV puncture site, known as the B point, is typically found in the extrahepatic portal vein (EPV), the root of the SMV, the hepatic side of the SV, or within the abdominal or retroperitoneal collateral (Fig. 1). When choosing collateral vessels for shunting, it is essential to consider the collateral' diameter, their blood flow direction in relation to the SMV and SV, their distance and spatial relationship with the inferior vena cava, as well as the surrounding tissues (typically the pancreas, intestines, and major vessels). Additionally, a minimum collateral diameter of 6 mm is deemed suitable for shunting, aiming to establish the safest and most direct shunting pathway. The catheter was superselected into the variceal vascular mass of the esophageal fundus, and the variceal vein was embolized using a mixture of spring coil (Interlock, Boston Scientific, USA) and embolization glue (Beijing Kangpaite Medical Equipment Co., Ltd., China)/papaverine ethyl iodide (Hengri Company, China). Subsequently, a pig-tail catheter or balloon with a diameter of 6–8 mm was positioned at the site of the pseudo-puncture, acting as the marker for the PV system's puncture. In addition, in cases where the hepatic artery and the adjacent portal vein are in close proximity, the use of the hepatic artery catheter as a marker can also be considered. If the patient has previously undergone TIPS, the lower end of the original stent can serve as a marker.
Fig. 1
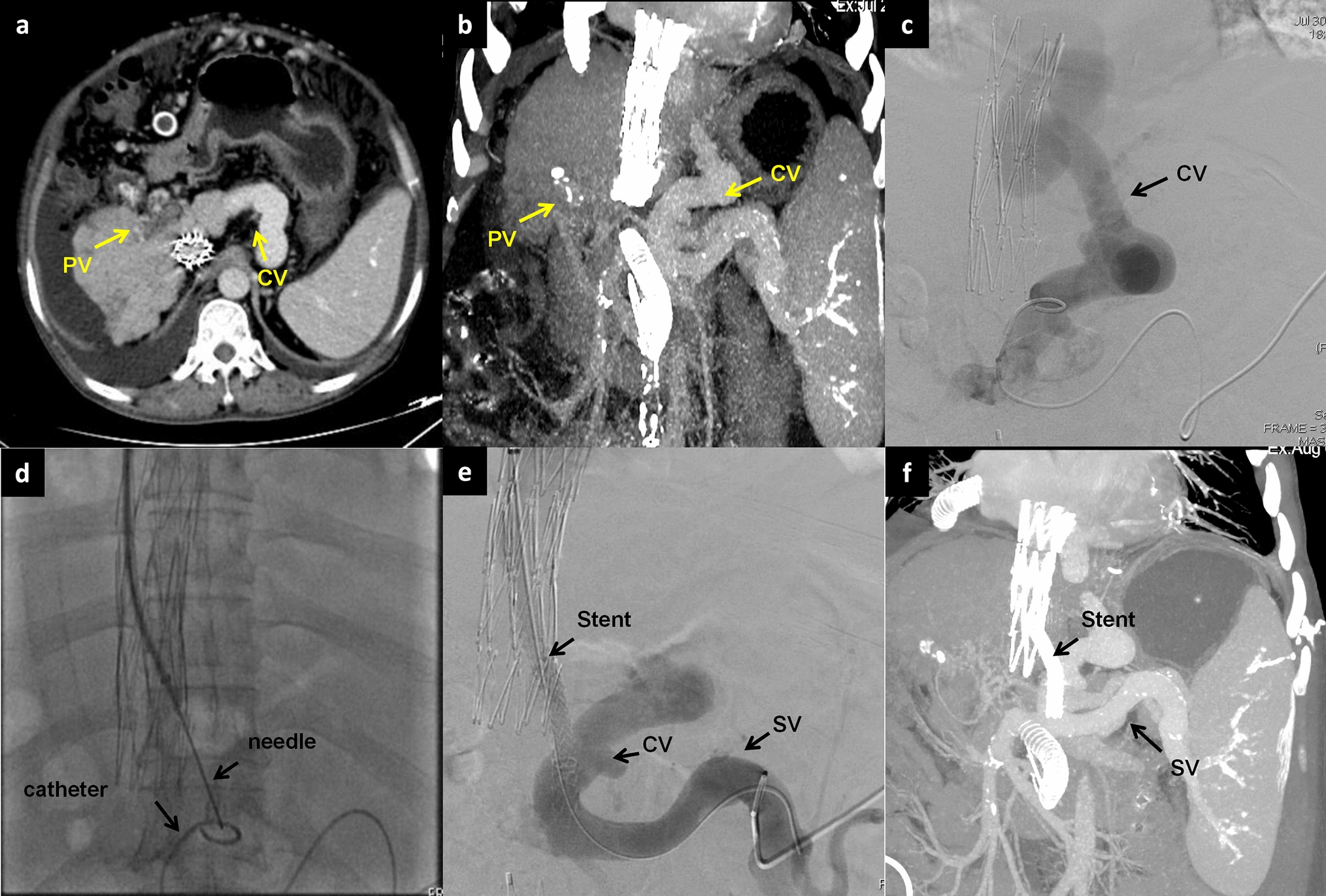
A 58-year-old male with Budd–Chiari syndrome, who had previously undergone an inferior vena cava-right atrial shunt and inferior vena cava stent implantation a decade ago, now presents with recurring episodes of esophagogastric variceal bleeding and recurrent ascites. a–b Spiral enhanced CT with multiplanar reconstruction showed cavernous transformation of the portal vein, with the presence of large retroperitoneal collateral vessels communicating with the splenic vein. c Direct portography was conducted through percutaneous splenic puncture, confirming the connection between the target collateral vessels and the splenic vein. d Under fluoroscopy, use the pig-tail catheter as a guide to target the puncture through the IVC. e A stent was successfully placed between retroperitoneal collateral vein and IVC. f The spiral-enhanced CT with multiplanar reconstruction images shows that the stent is patent at 1 month after TEPS. CV collateral vessels, PV portal vein, SV Splenic vein, IVC inferior vena cava
The internal jugular vein of each patient was punctured (the left internal jugular vein could be used if the right side vein was occluded). A RUPS-100 puncture system (Cook, USA) with a 10F-long sheath was then inserted into the inferior vena cava (IVC). After the puncture needle reached the predetermined hepatic vein or IVC (point A), the patient was instructed to hold their breath while adjusting the angle of the puncture needle under fluoroscopy and rotating the C-arm. The C-arm was adjusted to align the puncture point of the hepatic vein/IVC and the marker of the portal venous system with the direction of the puncture needle. Subsequently, the puncture marker was inserted, and the visible shift of the marker catheter or the puncture of the marker balloon indicated a successful puncture. The guide wire and 10F sheath were subsequently placed into the portal venous system to create a working channel. To minimize the risk of major bleeding, balloon dilation of the channel was avoided before the stent was implanted. The VIATORR® stent (Gore, USA) or Fluency™ stent (Bard, USA) was delivered through the 10F-long sheath to completely cover the puncture channel. Subsequently, a 7–8 mm-diameter balloon was employed to expand the puncture channel, with the proximal end of the stent positioned at the junction of the hepatic vein and IVC or within the IVC, while the distal end was placed inside the predetermined portal venous system.
In cases where the percutaneous transhepatic or percutaneous transsplenic approach proved ineffective, a midline vertical incision was performed below the umbilicus on the abdomen. This was done to expose the tributaries of the SMV with the assistance of surgeons. A 6F catheter sheath was then inserted into the main trunk of the SMV, and a 14 G metal tube and a 5.2F blue catheter, components of the RUPS-100 puncture system, was guided along the wire to the PV trunk or proximal SMV (point B). Under fluoroscopy, a pre-placed balloon in the posterior segment of the IVC was punctured, establishing a working channel in the reverse direction. The stent was subsequently implanted and dilated using the same method to achieve effective portosystemic shunting (Fig. 2).
Fig. 2
A 74-year-old male patient, who has been dealing with liver cirrhosis for 30 years, has been suffering from recurrent episodes of esophagogastric variceal hemorrhage and recurrent ascites for the recent three years. Previous interventions, including ESVD and LVP, have proven to be ineffective. a–b The multiplanar reconstruction from the spiral-enhanced CT scans demonstrated cavernous transformation of the portal vein, with patent mesenteric veins. c The transabdominal mesenteric venography reveals a patent mesenteric venous system and the presence of extrahepatic collateral vessels. d Utilizing a 14 G metal tube, part of the RUPS-100 apparatus, the tube was directed to the proximal region of the SMV with the aid of a guidewire. Following this, a pre-inserted balloon located in the posterior segment of IVC was successfully punctured. e A stent was successfully placed between SMV and IVC. f The spiral-enhanced CT with multiplanar reconstruction images show that the stent is patent at 1 month after TEPS. PV portal vein, IVC inferior vena cava, SMV Superior mesenteric vein, ESVD Endoscopic selective varices devascularization, LVP large-volume paracentesis
Follow-upFollowing TEPS, subcutaneous administration of low molecular weight heparin was initiated at a dosage of 4000 IU once every 12 h for 3 days. Additionally, rivaroxaban was administered at a dosage of 10 mg once daily for a minimum of 3 months to prevent shunt dysfunction.
In this study, patients were followed up at 3–7 days, 4–6 weeks, 3 months, 6 months, and 12 months post-procedure. The follow-up included monitoring the duration of postoperative hospitalization, symptoms and signs, shunt patency, and changes in liver and kidney function, coagulation parameters, ammonia, blood leukocytes, hemoglobin, and platelet levels. The patency of the shunt was monitored using color Doppler ultrasound and/or CTA.
留言 (0)