Portal hypertension (PH) has various etiologies other than cirrhosis including prehepatic, hepatic, and posthepatic conditions [1, 2]. When signs and symptoms of PH develop in the absence of liver cirrhosis, the condition is designated as non-cirrhotic portal hypertension (NCPH) [3, 4]. Many disorders are associated with NCPH, such as infiltrative diseases (i.e., sarcoidosis), vascular malignancies, schistosomiasis, congenital hepatic fibrosis, and primary liver diseases (i.e., primary biliary cholangitis, autoimmune hepatitis). The diagnosis of idiopathic non-cirrhotic portal hypertension (INCPH) is possible if all these disorders have been excluded [5, 6].
The term of INCPH was used for the first time in 2011 for the presence of PH without underlying liver disease and cirrhosis [7]. Various terms were used to date such as hepatoportal sclerosis, non-cirrhotic portal hypertension, idiopathic non-cirrhotic intrahepatic portal hypertension, idiopathic portal hypertension, non-cirrhotic portal fibrosis, incomplete septal cirrhosis, obliterative portal venopathy, and nodular regenerative hyperplasia for this entity [4, 6, 8,9,10,11,12,13,14,15]. Since similar histomorphological findings and clinical courses were observed and varying terms were confusing, the term of INCPH was introduced to standardize the nomenclature as a distinct single entity with various pathological aspects, rather than different clinicopathological entities [7].
INCPH is a vascular condition with unknown etiology causing PH and related clinical symptoms and laboratory findings [7, 16, 17]. Although the etiology is unknown, various circumstances such as immune function disorders, infectious etiologies, hematologic factors, metabolic factors, genetic predispositions, and drug exposure are thought to be playing role in disease development [3, 16, 18]. Cases without a defined underlying cause leading to INCPH were reported in 53% of a series comprising fifty-nine patients [8].
Liver biopsy is required for the diagnosis of INCPH due to the lack of definitive diagnostic tests and to rule out cirrhosis [5, 19]. Various histological changes, especially in portal/periportal areas, have been described in liver biopsies. However, INCPH may be underdiagnosed, because of inconspicuous and heterogeneously distributed histologic findings, in addition to the unawareness of the pathologists to this entity and evaluation of the biopsies without enough clinical information [6, 9,10,11, 18, 19]. The biopsy may appear nearly normal at low magnification. However, being aware of this diagnostic possibility and through examination of the liver biopsy may reveal some histological findings for the correct diagnosis [16,17,18,19,20]. Even though both portal tracts and lobular areas are affected, the most common striking features of INCPH are observed within the portal tracts. The histomorphologic findings of INCPH are summarized below:
Portal/periportal findings
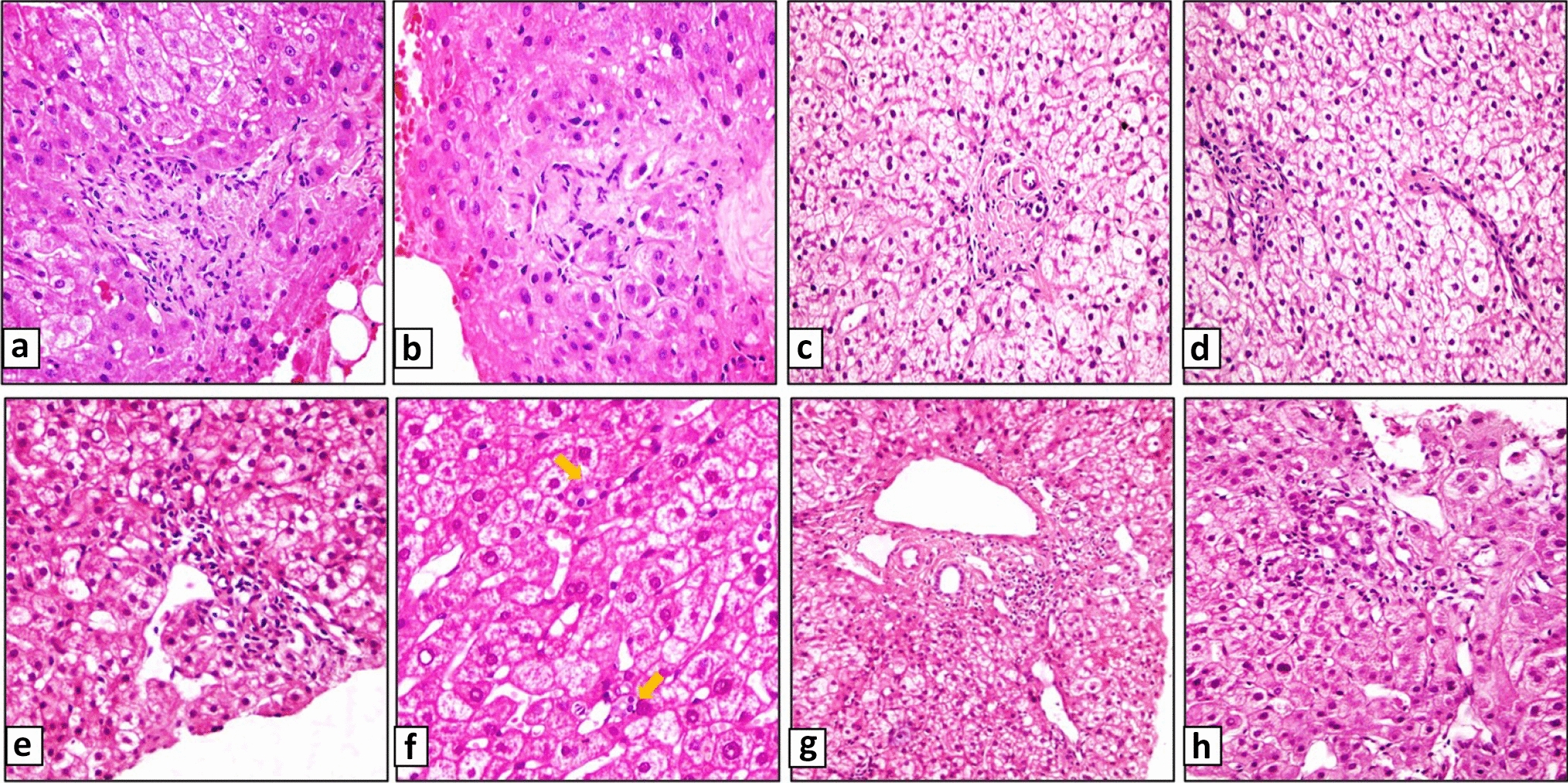
Portal tracts may be fibrotic, and the borders are rounded. Portal vein (PV) might be narrowed, obliterated, or lost. Obliterative portal venopathy (OPV), also known as phlebosclerosis, is considered to be the hallmark of INCPH [4]. OPV is characterized by mural fibrosis and thickening of intrahepatic small and medium-sized portal vein branches with subsequent luminal narrowing, obliteration and venopenia [12, 20]. Sometimes portal tract sclerosis or fibrosis cannot be seen, some portal tracts may be hypoplastic and only the remnants of the portal tracts might be present. PV branch is inconspicuous or absent in these portal tract remnants [16]. Identification of a narrowed PV in smallest or hypoplastic portal tracts may be difficult or they are overlooked [19]. Portal vein herniation into the periportal parenchyma, abnormal thin-walled periportal vessels, and portal tract hypervascularization creating a slit-like appearance are the other vascular findings of INCPH [9, 16,17,18,19,20].
Parenchymal architectural changes
The most common parenchymal lesion in INCPH is sinusoidal dilatation which is not specific to INCPH. It is usually due to increased sinusoidal pressure caused by changes in arterial or portal blood flow [17]. Another parenchymal finding is the close location of portal tracts to each other. Obliteration of the portal vein leads to parenchymal hypoperfusion, resulting in parenchymal extinction defined as a region with loss of contiguous hepatocytes that cause the proximity of portal tracts to each other [9, 18, 21].
Nodular regenerative hyperplasia (NRH) is another histologic finding consisting of numerous ill-defined nodules without fibrosis throughout the liver [10, 11, 13, 18, 22]. NRH demonstrates a vaguely nodular cut surface with the nodules having a pale appearance and the borders being darker in color. The pale-appearing nodules represent the areas of hypertrophy, and the borders consist of atrophic hepatocyte plates with or without any associated congestion [18].
In normal liver, sinusoidal endothelial cells do not exhibit CD34 expression. In some conditions such as focal nodular hyperplasia, macroregenerative nodule, CD34 expression can be observed in sinusoidal endothelial cells [23]. There is limited knowledge about the endothelial CD34 expression pattern in INCPH cases. Periportal sinusoidal CD34 immunoexpression has been mentioned in a few studies in patients with NRH and OPV [24, 25].
Glutamine synthetase (GS) is a useful marker in the differential diagnosis of liver tumors including hepatocellular adenomas and nodules in cirrhosis [26, 27]. In addition, abnormal hepatocellular GS expression patterns have been well documented in focal nodular hyperplasia (FNH) and nodular regenerative hyperplasia (NRH) [28, 29]. Normal GS expression is defined as a rim of 2–3 layers of strongly positive hepatocytes around the hepatic veins (perivenular pattern) [30]. In NRH, besides pericentral hepatocytes, immunoreaction in zone 2 hepatocytes [29] and diffuse hepatocellular immunoreaction were also reported [31].
Because of the ambiguous and heterogeneously distributed histologic findings and the lack of the entire set of histopathologic findings in the same biopsy, diagnosis of INCPH may be difficult, especially in small biopsies considered as nearly adequate. Portal venous obliteration, portal vein loss, and portal tract sclerosis were described as common findings. However, there are no well-established diagnostic criteria considered adequate for the histopathologic diagnosis and the amount of portal tracts displaying these findings have not been examined in detail in the literature. Furthermore, there is limited information about the utility of immunohistochemistry on the diagnosis of INCPH.
In this study, our aim was to evaluate all the histologic features as well as the endothelial CD34 and hepatocellular GS expression patterns in detail and reveal their impact on the biopsy diagnosis of INCPH.

留言 (0)