
記住我


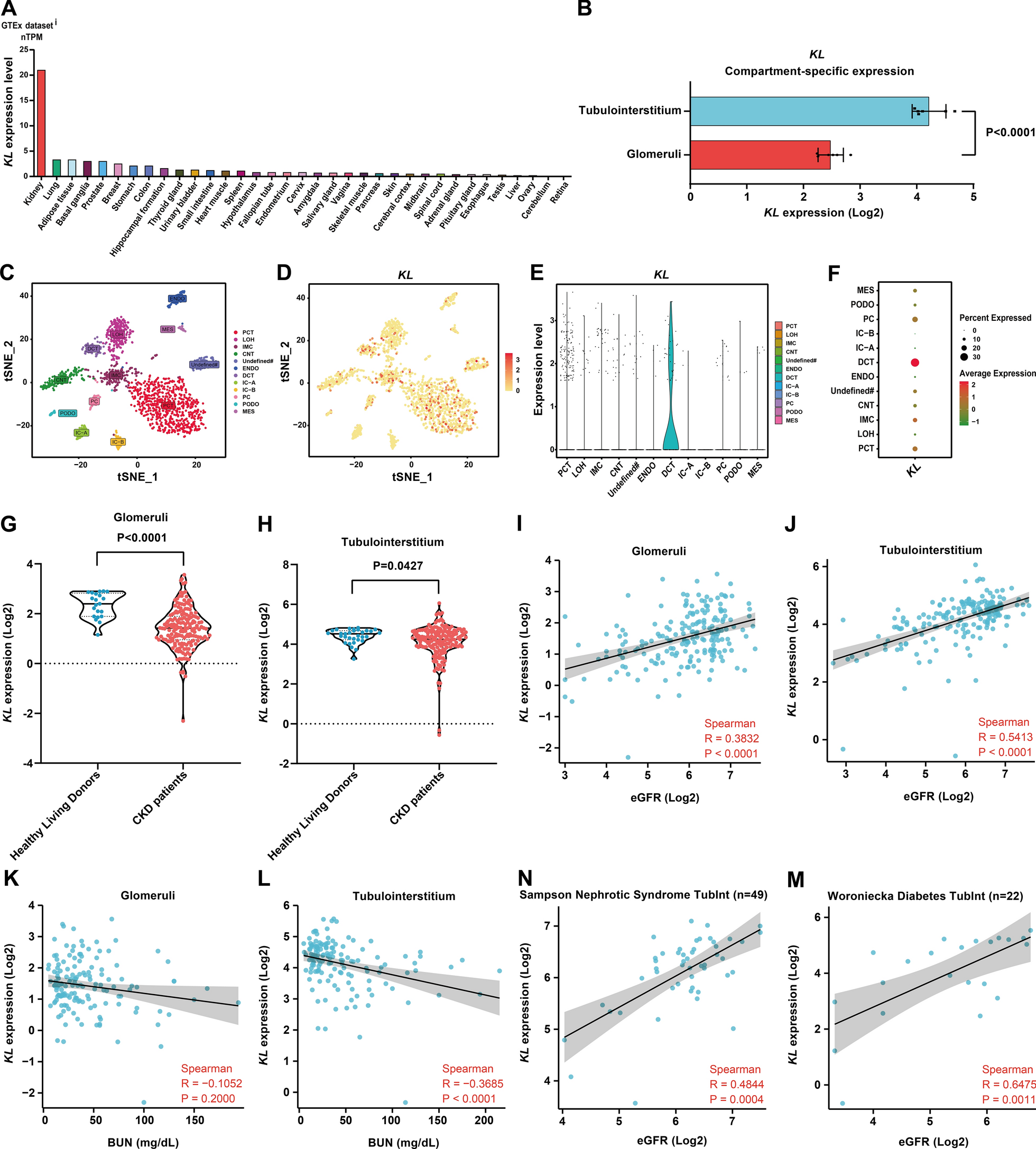

Given that the study reported that Klotho was mainly derived from the kidney [53], we analyzed the expression of KL in major organs/tissues throughout the body (data from the Human Protein Atlas database, Protein Atlas version 23.0) and found that the Klotho gene displayed a highly kidney-specific expression (Fig. 1A). We further analyzed KL expression in different compartments of normal kidney (data from the Nephroseq v5 database, raw data from GSE21785), and KL expression was significantly higher in the tubulointerstitium compared to the glomeruli (fold change = 3.334, P < 0.0001) (Fig. 1B). We also analyzed the expression of KL in normal adult kidney cells by snRNA-seq data (data from GSE118184) and found that KL was mainly expressed in distal convoluted tubule epithelial cells, followed by proximal convoluted tubule epithelial cells and also expressed in immune cells (Fig. 1C-F).
Fig. 1
Analysis of Klotho gene expression in kidney and its relationship to renal function in CKD. A KL expression in major human organs/tissues displayed a highly kidney-specific expression pattern. B KL expression was prominently higher (fold change = 3.334, P < 0.0001) in tubulointerstitium (n = 6) compared to glomeruli (n = 6) based on t-test statistics. C The tSNE plot indicated that the clustering of snRNA-seq of adult human kidney identified 12 distinct cell types. That included proximal convoluted tubule (PCT), loop of Henle (LOH), distal convoluted tubule (DCT), connecting tubule (CNT), principal cell (PC), intercalated cell type A (IC-A), intercalated cell type B (IC-B), podocyte (PODO), endothelium (ENDO), mesangial cell (MES), Immune cell (IMC), and Undefined cell (Undefined#). D-F Expression of KL in 12 different cell types as demonstrated by tSNE plot, Violin plots and Dot plot. G KL expression of glomeruli in CKD patients (n = 172) and Healthy Living Donors (n = 21). H KL expression of tubulointerstitium in CKD patients (n = 170) and Healthy Living Donors (n = 31). I Correlation between KL expression of glomeruli and eGFR of CKD patients (n = 192). J Correlation between KL expression of tubulointerstitium and eGFR of CKD patients (n = 186). K Correlation between KL expression of glomeruli and BUN of CKD patients (n = 150). L Correlation between KL expression of tubulointerstitium and BUN of CKD patients (n = 142). N, M Correlation between KL expression of tubulointerstitium and eGFR of patients in an independent CKD cohort (Sampson Nephrotic Syndrome TubInt) and a DN cohort (Woroniecka Diabetes TubInt). KL, Klotho gene; eGFR, estimated glomerular filtration rate; BUN, blood urea nitrogen; CKD, chronic kidney disease; DN, diabetic nephropathy; Spearman, Spearman correlation analysis; R, correlation coefficient R; P, P-value
We also analyzed KL expression in the kidney of CKD and its relationship with renal function. Since the expression of KL in the glomeruli and tubulointerstitium differed significantly (Fig. 1B), we analyzed them separately (data from the Ju CKD Glom and Ju CKD TubInt datasets in the Nephroseq v5 database). We found that KL expression in both glomeruli and tubulointerstitium was significantly lower in CKD patients than in Healthy Living Donors (p < 0.0001 and P = 0.0427) (Fig. 1G, H). We further analyzed the relationship between glomerular and tubulointerstitial KL expression and eGFR or BUN in CKD by Spearman correlation analysis, respectively, and found that both glomerular and tubulointerstitial KL expressions in CKD were positively correlated with eGFR (R = 0.3832 and 0.5413, all P < 0.0001) (Fig. 1I, J). However, when analyzing the correlation between KL expression and BUN, only KL expression in the CKD tubulointerstitium was negatively correlated with BUN (R =−0.3685, P < 0.0001) (Fig. 1L), while KL expression in the CKD glomeruli was not correlated with BUN (R =−0.1052, P = 0.2000) (Fig. 1K). The results obtained indicate a stronger correlation between KL expression in the renal tubulointerstitium and renal function than in the glomeruli. We also analyzed two independent tubulointerstitial transcriptome datasets for CKD (data from the Nephroseq v5 database) and found that KL expression was positively correlated with eGFR in both the Sampson Nephrotic Syndrome TubInt and Woroniecka Diabetes TubInt datasets (R = 0.4844 and 0.6475, P = 0.0004 and 0.0011) (Fig. 1N, M), which further confirmed that Klotho gene expression in the tubulointerstitium was well correlated with renal function.
Klotho gene expression is mainly negatively associated with the inflammatory response in CKD tubulointerstitiumThe Klotho gene is mainly expressed in the tubulointerstitium, and its expression correlates well with renal function in CKD. Therefore, we focused on its main regulatory pathways in the CKD tubulointerstitium. We first investigated its major negative regulatory pathway in CKD tubulointerstitium. We respectively used the GSE104954 (CKD) and GSE108112 (CKD) datasets to screen the genes that were significantly negatively associated with KL expression by Spearman correlation analysis (correlation coefficient R < -0.5, P < 0.05). Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses were performed on the above screened genes in the DAVID database. In both the GSE104954 (CKD) and GSE108112 (CKD) datasets, the biological process most associated with Klotho gene is the inflammatory response (Fig. 2A, E), the cellular component most related to the Klotho gene is extracellular exosome (Fig. 2B, F), and the molecular function most associated with Klotho gene is protein binding (Fig. 2C, G). Both datasets in the KEGG analysis exhibited some pathways related to inflammation (Fig. 2D, H). The above results suggest that Klotho may negatively regulate the inflammatory response mainly through extracellular secretion and protein binding. We next used gene set variation analysis (GSVA) by GSE104954 (CKD) and GSE108112 (CKD) datasets to determine enrichment scores for inflammatory response processes. Correlation analysis between enrichment scores and KL expression showed that Klotho gene expression was negatively correlated with inflammatory response-related functions in both datasets (Fig. 2I, J), except in the GSE104954 (CKD) dataset, where there was no correlation with the chronic inflammatory response to antigenic stimulus (Fig. 2I). These results suggest that Klotho may mainly negatively regulate the inflammatory response in CKD tubulointerstitium.
Fig. 2
Klotho gene expression is predominantly negatively associated with the inflammatory response in CKD tubulointerstitium. A-D The top 5 biological processes (BP), cellular components (CC), molecular functions (MF), and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways were mostly related to the Klotho gene in the GSE104954 (CKD). E-H The top 5 biological processes (BP), cellular components (CC), molecular functions (MF), and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways were mostly related to the Klotho gene in the GSE108112 (CKD). I, J The heatmaps showed Klotho gene expression and enrichment scores of inflammatory response functions of each patient in the GSE104954 (CKD) and GSE108112 (CKD). The samples were arranged in ascending order of Klotho gene expression. The bar and point line plots on the right showed the correlation coefficient R and P-value of the Spearman correlation analysis
Klotho may affect immune cell infiltration in CKD tubulointerstitiumGiven that the Klotho gene expression is mainly negatively associated with the inflammatory response in CKD tubulointerstitium, and soluble Klotho primarily originates from cleaved membrane-bound Klotho [54], exerting its influence on the physiological functions of neighboring cells through paracrine secretion, as well as the presence of immune cell infiltration in the CKD tubulointerstitium [55], we next investigated the relationship between Klotho and immune cell infiltration in CKD tubulointerstitium. We studied the percentage of 22 immune cells in the GSE104954 and GSE108112 datasets using the online tool CIBERSORTx (Fig. 3A, C) and found that in GSE104954, the percentage of Mast cells activated, Dendritic cells resting and B cells naive in CKD were significantly lower than those in normal controls (all P < 0.05), while the percentage of Mast cells resting, Macrophages M1, T cells gamma delta and B cells memory in CKD were significantly higher than those in normal controls (all P < 0.05) (Fig. 3B). These analyses were not performed in the GSE108112 dataset due to the small number of normal controls (5 cases). We next analyzed the correlation between the percentage of 21 immune cells and Klotho gene expression in GSE104954 (CKD) and GSE108112 (CKD) and found that the percentage of Neutrophils and T cells gamma delta was negatively correlated with KL expression in both GSE104954 (CKD) and GSE108112 (CKD) datasets, and T cells regulatory (Tregs) was positively correlated with KL expression in both datasets (all P < 0.05) (Fig. 3D). These findings suggest that Klotho may be involved in the regulation of immune cell infiltration in CKD tubulointerstitium.
Fig. 3
Immune cell infiltration analysis in CKD tubulointerstitium. A, C The percentage of 22 immune cells for each sample of GSE104954 and GSE108112. B Comparison of the proportion of each immune cell in the tubulointerstitium between Control and CKD groups. D Correlation between Klotho gene expression and the percentage of each immune cell of each sample in GSE104954 (CKD) and GSE108112 (CKD). The width of the band represented the correlation coefficient R in the chord diagram. The red band represented a positive correlation; the green band represented a negative correlation. The color of the upper outer band represented the P-value. The correlation was tested by Spearman correlation analysis. R represented correlation coefficient. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001
To verify that Klotho may affect immune cell infiltration, we performed in vitro experiments. Considering that Klotho could modulate monocyte inflammatory factor release [56], and there was also a negative correlation between the percentage of monocytes in GSE104954 (CKD) and GSE108112 (CKD) and the expression of KL (with P < 0.05 in GSE108112) (Fig. 3D), we chose monocytes for the transwell invasion assay. Our results showed that Klotho could alleviate monocyte invasion under different induction factor conditions (Additional file 2: Fig. S1A, B), suggesting that Klotho may affect immune cell infiltration in CKD tubulointerstitium.
Klotho gene expression is mainly positively associated with lipid metabolism in CKD tubulointerstitiumWe have analyzed that the main negative regulatory pathway of Klotho in CKD tubulointerstitium may be the inflammatory response, but its main positive regulatory pathway is still unclear. Therefore, we also respectively used the GSE104954 (CKD) and GSE108112 (CKD) datasets to screen the genes that were significantly positively associated with KL expression by Spearman correlation analysis (correlation coefficient R > 0.5, P < 0.05). GO and KEGG analyses were performed on the above screened genes in the DAVID database. In the GSE104954 (CKD) and GSE108112 (CKD) datasets, the most relevant biological process with Klotho gene is fatty acid β-oxidation, followed by fatty acid metabolic process and lipid metabolic process (Fig. 4A, E), and the cellular components related to the Klotho gene are mitochondrion, mitochondrial matrix and extracellular exosome (Fig. 4B, F), and the molecular functions associated with Klotho gene are catalytic activity, oxidoreductase activity, flavin adenine dinucleotide binding, and electron carrier activity (Fig. 4C, G). Both datasets in the KEGG analysis show mainly metabolic pathways (Fig. 4D, H). The above results suggest that Klotho may positively regulate lipid metabolism mainly through the involvement of cellular mitochondrion in fatty acid β-oxidation. We next used gene set variation analysis (GSVA) in the GSE104954 (CKD) and GSE108112 (CKD) datasets to determine enrichment scores for lipid metabolism. Correlation analysis between enrichment scores and KL expression showed a positive correlation between Klotho gene expression and lipid metabolism-related functions in both datasets (Fig. 4I, J). These results suggest that Klotho may mainly positively regulate lipid metabolism in CKD tubulointerstitium.
Fig. 4
Klotho gene expression is predominantly positively associated with lipid metabolism in CKD tubulointerstitium. A-D The top 5 biological processes (BP), cellular components (CC), molecular functions (MF), and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways were mostly related to the Klotho gene in the GSE104954 (CKD). E-H The top 5 biological processes (BP), cellular components (CC), molecular functions (MF), and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways were mostly related to the Klotho gene in the GSE108112 (CKD). I, J The heatmaps showed Klotho gene expression and enrichment scores of lipid metabolism functions of each patient in the GSE104954 (CKD) and GSE108112 (CKD). The samples were arranged in ascending order of Klotho gene expression. The bar and point line plots on the right showed the correlation coefficient R and P-value of the Spearman correlation analysis
Klotho may improve fatty acid oxidation by regulating PPARA and PPARGC1A expression in CKD tubulointerstitiumPeroxisome proliferator-activated receptor α (PPARA) and PPAR-γ coactivator-1α (PPARGC1A) are the key transcription factors that regulate the expression of fatty acid oxidation-related enzymes [57], so we analyzed the expression of PPARA, PPARGC1A, fatty acid oxidation-related enzyme genes and KL in GSE104954. We found that KL expression was significantly decreased in CKD patients compared to Living Donors (P < 0.01) (Fig. 5A), which is consistent with the former result (Fig. 1H). It was also found that the expression of PPARA, PPARGC1A, CPT1A and ACOX1 was also significantly decreased in CKD patients compared to Living Donors (all P < 0.05) (Fig. 5B-E). These results suggest that fatty acid oxidation may be hindered in CKD tubulointerstitium. We further analyzed the correlation between KL expression and the expression of the above fatty acid oxidation-related genes. We found that except for CPT1A expression, which showed no significant correlation with KL expression in GSE104954 (CKD), the remaining genes showed a clear positive correlation with KL expression in both GSE104954 (CKD) and GSE108112 (CKD) (Fig. 5G, H). Moreover, our in vitro experiments also confirmed that Klotho could positively regulate the expression of PPARA, PPARGC1A, CPT1A, ACOX1 and ACOX2 in HK-2 treated with TPA (Fig. 6I). In particular, we also demonstrated at the protein level that Klotho could positively regulate the expression of PPARα and PGC1α (Additional file 2: Fig. S2A-C). Given that Klotho ameliorated abnormal lipid metabolism in the liver by upregulating PPARA expression in type 2 diabetic mice [14], our results suggest that Klotho may improve fatty acid oxidation by regulating PPARA and PPARGC1A expression.
Fig. 5
Relationship analysis of Klotho gene expression with fatty acid oxidation-related genes expression in CKD tubulointerstitium. A-F Comparative analysis of the expression of KL, PPARA, PPARGC1A, CPT1A, ACOX1 and ACOX2 in tubulointerstitium of Living Donors (n = 21) and CKD patients (n = 169) based on the Mann-Whitney test in GSE104954. G, H The heatmaps showed the correlation between each of genes (KL, PPARA, PPARGC1A, CPT1A, ACOX1 and ACOX2) in GSE104954 (CKD) and GSE108112 (CKD). The correlation was tested using Spearman correlation analysis. R represented correlation coefficient. *P < 0.05, **P < 0.01, ****P < 0.0001
Fig. 6
Klotho reduced inflammatory response and improved lipid metabolism in HK-2 treated with TPA. A Representative photomicrographs of Oil Red O staining of HK-2 treated with PA, TGF-β1, and TPA. Scale bars = 50 μm. B Western blot and real-time PCR analysis of Klotho expression in HK-2 treated with TPA. The molecular weight of Klotho was about 62 kDa, representing soluble Klotho in the Western blot bands. The molecular weight of GAPDH was 36 kDa. C Representative photomicrographs of Oil Red O staining of HK-2 treated with TPA and TPA + rKlotho. Scale bars = 50 μm. D Statistical analysis of lipid droplets in each group in C. E Detection of TG concentration in HK-2 treated with TPA and TPA + rKlotho. F Representative photomicrographs of mitochondria labeled with MitoTracker in HK-2 treated with TPA and TPA + rKlotho. Nuclei was stained with Hoechst (blue). Scale bars = 60 μm. G Statistical analysis of percentage of cells with altered mitochondrial pattern and mean branch length of mitochondrion in each group in F. H Western blot analysis of pSmad3 and Smad3 expression in HK-2 treated with TPA and TPA + rKlotho. The molecular weight of pSmad3 and Smad3 was 55 kDa. I Real-time PCR analysis of SREBP1, FASN, SCD1, CD36, FATP1, FATP2, PPARA, PPARGC1A, CPT1A, ACOX1 and ACOX2 expression in HK-2 treated with TPA and TPA + rKlotho. J The concentrations of TNF-α, IL-6, and IL-1β in the culture supernatants of HK-2 treated with TPA and TPA + rKlotho. PA, palmitic acid; TPA, TGF-β1 and palmitic acid; rKlotho, recombinant human Klotho; TG, triglyceride. The results were mean ± SEM of three independent experiments. *P < 0.05, ** P < 0.01, ***P < 0.001, ****P < 0.0001
Klotho regulated inflammatory response and lipid metabolism in HK-2 exposed to a CKD-like environmentWe have found that Klotho may mainly negatively regulate inflammatory response and positively regulate lipid metabolism in CKD tubulointerstitium by bioinformatics analysis. Next, we sought to confirm our findings by establishing an in vitro model similar to CKD. We found that HK-2 showed intracellular lipid droplets accumulation after 48 h of treatment with either palmitic acid or TGF-β1, especially after HK-2 was treated with both palmitic acid and TGF-β1 (Fig. 6A). Given that lipids and TGF-β1 are elevated in CKD [58, 59], we constructed an in vitro model similar to CKD by simultaneously stimulating HK-2 with TGF-β1 and palmitic acid (TPA). We found that TPA significantly decreased the expression of Klotho and increased the accumulation of lipid droplets and TG content compared to controls in HK-2 (Fig. 6B-E). However, the addition of rKlotho treatment markedly reduced the accumulation of lipid droplets and TG content compared to TPA groups in HK-2 (Fig. 6C-E). We found that the involvement of Klotho in fatty acid β-oxidation might be associated with mitochondrion (Fig. 4B, F), so we observed the morphological changes of mitochondria with MitoTracker in HK-2 treated with TPA. We found that TPA significantly altered mitochondrial morphology and shortened the average branch length of each mitochondrion, but the addition of rklotho reversed the above process (Fig. 6F, G).
Given that TGF-β1 depends on Smad3 to repress fatty acid oxidation [57], and the activation of Smad3 also mediates inflammation [60], we examined the expression of pSmad3 and Smad3 in HK-2 treated with TPA. We observed that TPA significantly activated the phosphorylation of Smad3 (pSmad3), but this was obviously inhibited by the addition of rKlotho (Fig. 6H). We next examined the transcript levels of genes related to fatty acid oxidation and found that TPA significantly inhibited the expression of PPARA, PPARGC1A, CPT1A, ACOX1 and ACOX2, but was significantly improved by the addition of rKlotho (Fig. 6I). Moreover, rKlotho also markedly downregulated the abnormal elevation of the adipogenic genes (SREBP1, FASN and SCD1) and fatty acid transporter genes (CD36 and FATP1) in HK-2 treated with TPA (Fig. 6I). Finally, we found that TPA induced the HK-2 inflammatory response to release the inflammatory factors TNF-α, IL-6 and IL-1β, but was inhibited by rKlotho (Fig. 6J). Together, these results confirmed that Klotho could reduce the inflammatory response and improve lipid metabolism in HK-2 exposed to a CKD-like environment.
Based on all the results above, we have demonstrated a good correlation between Klotho and renal function at the gene level through bioinformatics analysis. In particular, we have found that inflammatory response and lipid metabolism are the top pathways that Klotho may regulate in CKD tubulointerstitium. Moreover, our in vitro experiments also confirmed that Klotho could negatively regulate inflammatory response and positively regulate lipid metabolism. Given that a landmark study shows that inflammation and metabolism are the primary dysregulated pathways in CKD tubulointerstitium [57], in which metabolic abnormalities mainly include abnormal lipid metabolism, coupled with a parallel relationship between soluble Klotho levels in peripheral blood and renal Klotho expression levels [2], as well as dyslipidemia and elevated inflammatory markers in CKD [61, 62], we speculate that there is a close relationship between Klotho and blood lipids, inflammatory markers and kidney function in the CKD population. Therefore, we next used the clinical data from NHANES 2007–2016 containing the Klotho indicator to confirm our speculation. See Fig. 7 for the research flowchart.
Fig. 7
Flowchart of studying the NHANES 2007–2016 Klotho-related clinical data. The others include high density lipoprotein (HDL), total cholesterol (TC) and triglyceride (TG). CKD, chronic kidney disease; LDL, low density lipoprotein
Characteristics of NHANES populationAmong the 9719 adults (aged 40–79 years) from five NHANES cycles, 1520 participants were diagnosed with CKD, and the remainder were participants without CKD. Lipid biomarkers, inflammatory biomarkers and renal function biomarkers were described based on the actual number of participants with these biomarkers in the non-CKD and CKD populations. The baseline characteristics of study participants with and without CKD were summarized in Table 1. Overall, there were statistically significant differences between non-CKD and CKD participants in terms of sex, age, race, educational attainment, BMI, smoking status, CVD, DM, hypertension, Klotho, TC, TG, WBC, Neu, Mono, SII, NLR, MLR, SIRI, PIV, eGFR, serum creatinine, uric acid and serum urea nitrogen (all P < 0.05). However, no significant differences were observed between the two groups for other variables, including HDL, LDL, Lym, PLR and UACR (all P > 0.05).
Table 1 Descriptive characteristics of NHANES participantsKlotho was negatively associated with inflammatory response and positively associated with lipid metabolism and renal function in general populationIn the general population, the associations of Klotho with inflammatory biomarkers, lipid biomarkers, and renal function in both categorical and continuous analyses in generalized linear model (GLM) were presented in Additional file 1: Table S2. Using the lowest tertile of Klotho level (T1) as the reference, the β and 95% CI for TC, eGFR, serum urea nitrogen, serum creatinine, and uric acid in the moderate tertile of Klotho level (T2) were β − 3.227 (95% CI − 6.288, − 0.167), β 1.689 (95% CI 0.596, 2.782), β − 0.409 (95% CI − 0.668, − 0.150), β − 0.033 (95% CI − 0.050, − 0.016) and β − 0.172 (95% CI − 0.255, − 0.088) in the adjusted model (all P < 0.05). Furthermore, using the T1 as the reference, the β and 95% CI for WBC, Neu, PLR, PIV, SII, TC, TG, eGFR, serum urea nitrogen, serum creatinine and uric acid in the highest tertile of Klotho level (T3) were β − 0.174 (95% CI − 0.319, − 0.028), β − 0.160 (95% CI − 0.288, − 0.032), β − 5.865 (95% CI − 9.028, − 2.702), β − 27.806 (95% CI − 43.335, − 12.277), β −43.053 ( 95% CI − 65.437, − 20.669), β − 4.335 (95% CI − 7.629, − 1.041), β − 12.756 (95% CI − 23.960, − 1.552), β 2.799 (95% CI 1.792, 3.806), β − 0.589 (95% CI − 0.892, − 0.285), β − 0.050 (95% CI − 0.068, − 0.032) and β − 0.351 (95% CI − 0.434, − 0.269) in the adjusted model (all P < 0.05). The continuous analysis showed that Klotho had a significant negative association with WBC, Neu, NLR, PLR, PIV, SIRI, SII, TC, TG, serum urea nitrogen, serum creatinine and uric acid, and a positive association with eGFR (all P < 0.05, adjusted model).
Klotho was negatively associated with inflammatory response and positively associated with lipid metabolism and renal function in CKD populationIn the CKD population, the associations of Klotho with inflammatory biomarkers, lipid biomarkers, and renal function in both categorical and continuous analyses in GLM were presented in Additional file 1: Table S3. Using the T1 as the reference, the β and 95% CI for WBC, Neu, Mono, SIRI, TG, eGFR, serum urea nitrogen and serum creatinine in the T2 were β − 0.365 (95% CI − 0.665, − 0.065), β − 0.293 (95% CI − 0.548, − 0.038), β − 0.033 (95% CI − 0.064, − 0.002), β − 0.178 (95% CI − 0.346, − 0.009), β − 22.273 (95% CI − 43.217, − 1.329), β 5.917 (95% CI 1.772, 10.062), β − 1.586 (95% CI − 2.562, − 0.611) and β − 0.167 (95% CI − 0.270, − 0.065) in the adjusted model (all P < 0.05). Furthermore, using the T1 as the reference, the β and 95% CI for WBC, Neu, NLR, MLR, PLR, PIV, SIRI, SII, TG, eGFR, serum urea nitrogen, serum creatinine and uric acid in the T3 were β − 0.414 (95% CI − 0.685, − 0.143), β − 0.399 (95% CI − 0.668, − 0.129), β − 0.275 (95% CI − 0.473, − 0.077), β − 0.026 (95% CI − 0.047, − 0.006), β − 7.627 (95% CI − 15.041, − 0.212), β − 74.675 (95% CI − 123.447, − 25.904), β − 0.237 (95% CI − 0.415, − 0.060), β − 97.05 (95% CI − 149.552, − 44.548), β − 21.19 (95% CI − 41.948, − 0.432), β 8.476 (95% CI 5.046, 11.906), β − 2.499 (95% CI − 3.451, − 1.548), β − 0.231 (95% CI − 0.343, − 0.119) and β − 0.581 (95% CI − 0.829, − 0.332) in the adjusted model (all P < 0.05). The continuous analysis showed that Klotho had a significant negative association with WBC, Neu, NLR, MLR, PLR, PIV, SIRI, SII, serum urea nitrogen, serum creatinine and uric acid, and a positive association with eGFR (all P < 0.05, adjusted model).
Klotho has an optimal concentration range for exerting its biological functionBased on the fact that Klotho was negatively associated with WBC, Neu, NLR, PLR, PIV, SII, SIRI, TG, serum creatinine, serum urea nitrogen and uric acid, and positively associated with eGFR in the general and CKD populations (Additional file 1: Tables S2, S3), RCS was applied to examine the nonlinear relationship and threshold effect of Klotho with them. We found Klotho was linearly related to WBC, Neu, NLR, PLR and SII (all P-nonlinear > 0.05) and non-linearly related to PIV, SIRI, TG, eGFR, serum creatinine, serum urea nitrogen and uric acid (all P-nonlinear < 0.05) in the general population (Fig. 8). In the CKD population (Fig. 9), Klotho was linearly related to WBC, Neu, NLR, PLR, PIV, SII, TG, eGFR, serum urea nitrogen and uric acid (all P-nonlinear > 0.05) and non-linearly related to SIRI and serum creatinine (all P-nonlinear < 0.05). Except for indicators with P-nonlinear > 0.7, we found that the threshold effects of Klotho on the above 12 biological indicators were all close to 1000 pg/ml. The functional effects of Klotho were significantly altered in this threshold range (Figs. 8, 9). These results suggest that the optimal concentration range for Klotho to exert its biological function is around 1000 pg/ml.
Fig. 8
RCS estimated the dose–response relationships between Klotho and 95% CIs of biomarkers in general population. The model was fully adjusted for sex, age, race, educational attainment, BMI, smoking status, CVD, DM and hypertension. RCS, restricted cubic spline; 95% CI, 95% confidence interval; Blue solid line, beta value; Blue dot, the median level of Klotho; Black dashed line, reference level; Red dashed line, Klotho 1000 pg/ml level; Blue shade, 95% CI
Fig. 9
RCS estimated the dose–response relationships between Klotho and 95% CIs of biomarkers in CKD population. The model was fully adjusted for sex, age, race, educational attainment, BMI, smoking status, CVD, DM and hypertension. RCS, restricted cubic spline; 95% CI, 95% confidence interval; Blue solid line, beta value; Blue dot, the median level of Klotho; Black dashed line, reference level; Red dashed line, Klotho 1000 pg/ml level; Blue shade, 95% CI
Biomarkers of inflammation and lipid mediated the association between Klotho and renal function in general populationTo assess whether the association between Klotho and renal function may be mediated by biomarkers of inflammation and lipid in the general population, we performed a mediation analysis. In the general population (Additional file 1: Table S4), the results showed that inflammatory biomarkers (WBC, Neu, NLR, SIRI and SII) mediated the association between Klotho and eGFR, and the proportions were 3.749%, 3.747%, 2.073%, 1.448% and 2.375%, respectively (all p < 0.05). No significant mediation effects of lipid biomarkers (TC, TG, HDL and LDL) were observed in the association of Klotho with eGFR (all p > 0.05). Inflammatory biomarkers (WBC and Neu) mediated the association between Klotho and serum urea nitrogen, and the proportions were 3.594% and 2.468% (all p < 0.05). TG mediated the association between Klotho and serum urea nitrogen, and the proportion was 3.382% (p = 0.016). Inflammatory biomarkers (WBC, Neu, NLR, PIV, SIRI and SII) mediated the association between Klotho and serum creatinine, and the proportions were 2.482%, 3.158%, 2.808%, 1.913%, 1.801% and 3.113%, respectively (all p < 0.05). No significant mediation effects of lipid biomarkers (TC, TG, HDL and LDL) were observed in the association of Klotho with serum creatinine (all p > 0.05). Inflammatory biomarkers (WBC, Neu and SIRI) mediated the association between Klotho and uric acid, and the proportions were 2.134%, 1.749% and 0.688%, respectively (all p < 0.05). TC and TG mediated the association between Klotho and uric acid, and the proportions were 4.349% and 2.511% (all p < 0.05). No significant mediation effects of inflammatory biomarkers and lipid biomarkers were observed in the association of Klotho with UACR (all p > 0.05). These above results indicate that Klotho may improve renal function in the general population by regulating the inflammatory response and lipid metabolism.
Inflammatory biomarkers mediated the association between Klotho and renal function in CKD populationIn the CKD population (Additional file 1: Table S5), our results showed that inflammatory biomarkers (WBC and Neu) mediated the association between Klotho and eGFR, and the proportions were 3.478% and 3.449% (all p < 0.05). No significant mediation effects of lipid biomarkers (TC, TG, HDL and LDL) were observed in the association of Klotho with eGFR (all p > 0.05). WBC mediated the association between Klotho and serum urea nitrogen, and the proportion was 2.858% (p = 0.048). No significant mediation effect
留言 (0)