
記住我



The study survey was reviewed and approved by the ethical review board of the National Bioethics Committee of Bolivia at the National University San Simon. Informed consent was obtained from parents and guardians before data collection and access to identifiable data was restricted to maintain confidentiality. De-identified microdata are publicly available at http://dx.doi.org/https://doi.org/10.18235/0001649.
Study designWe conducted a randomized control trial in the 8th district of El Alto, Bolivia, to evaluate the effect of a community nutrition program on caregiver knowledge, IYCF practices, and child nutrition and growth [26]. The city of El Alto, located adjacent to La Paz in the Altiplano highlands, is the fastest growing urban center in Bolivia with the highest population density in the country. In 2016, prior to the intervention, the city had a poverty rate of 67% and was 86% indigenous, the majority identifying as Aymara. The 8th district, where the program was implemented, was predominately low-income. At baseline, most families lived in precarious housing conditions, had no sanitation or waste collection services, and exhibited poor health practices [25].
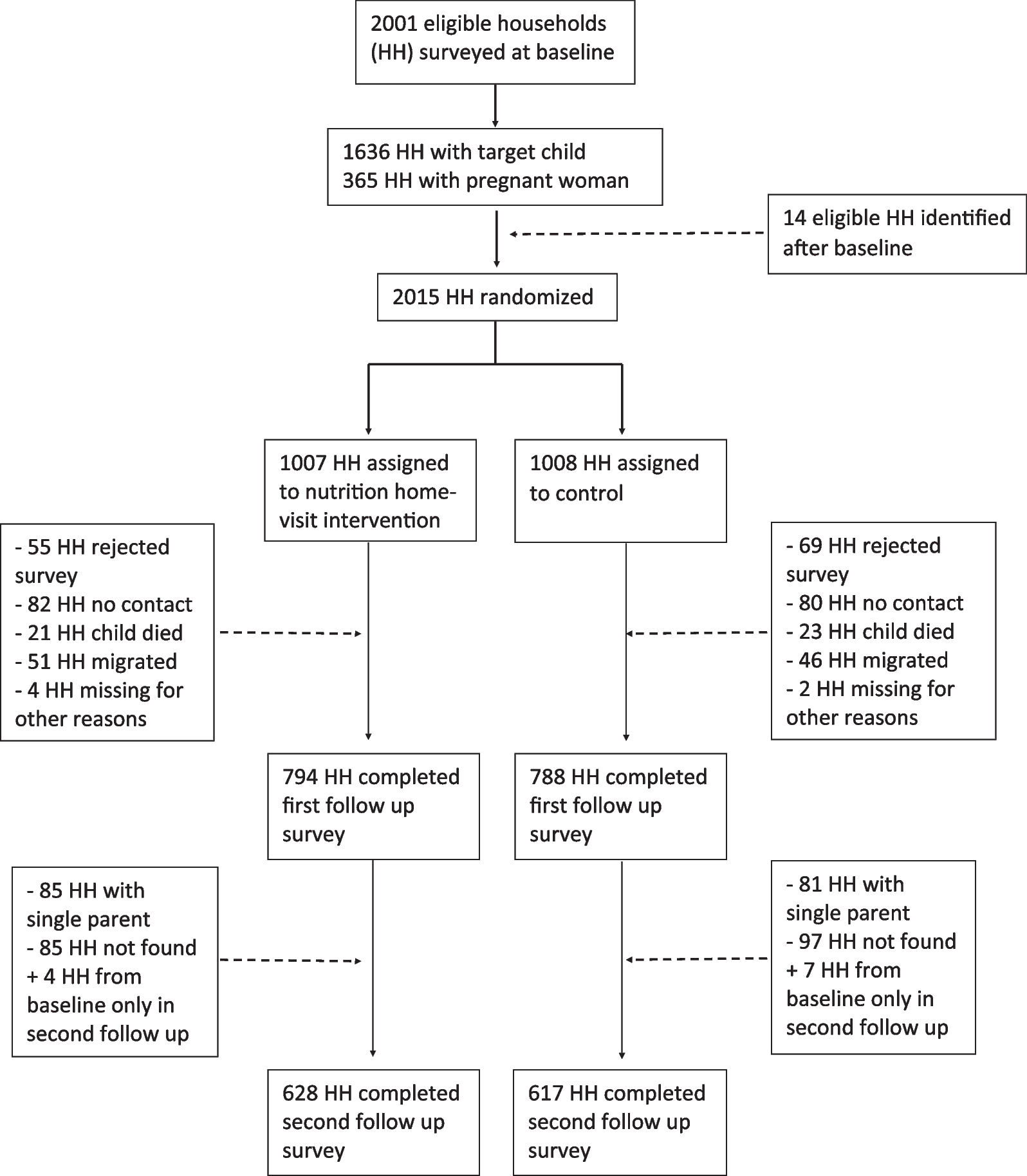
Prior to the start of the program, the research team conducted a census in the 8th district to identify households with a pregnant woman or a child under 12 months old. Two thousand and one households were eligible and baseline data were collected between March and July 2014. Following baseline, the study randomly assigned households to treatment and control groups with equal probability. Fourteen additional households were recruited after baseline and were randomized according to the same procedure. The project invited households assigned to treatment to participate in the program and enrolled a total of 1882 consenting households. Two rounds of follow-up data were collected approximately 30 months and 42 months after baseline. Martinez et al. 2018 [26] presents the results of the 30-month follow-up. This study adds a second round of follow-up data 42 months after baseline and expands the original analysis with a focus on IYCF. The study design is illustrated in Fig. 1.
Fig. 1 Description of Intervention
Description of InterventionThe Community Child Nutrition (CCN) project was implemented by the Andean Rural Health Council (CSRA, for its Spanish acronym) between 2014 and 2016 [25, 26]. The intervention used a culturally adapted entertainment-education approach to promote recommended nutritional practices and built upon previous experiences of CSRA with nutrition counseling in El Alto [26, 27]. The project’s objectives were to improve IYCF practices, hygiene, and nutritional status through a behavioral-change education strategy based on participatory play. The project hired community health workers to deliver the program. Health workers were required to have at least three years of work experience in family and community health, some work experience with entertainment-education, residence in El Alto, and understanding of the native language (Aymara). Most health workers also had formal training as doctors or nurses. Following recruitment, the program trained health workers on nutrition, according to Ministry of Health standards, and on management, application, and creation of program scripts and play techniques (puppets, clowns, songs, poems, communication skills, construction and acting of characters). Recruitment and training of health workers lasted about three months.
After the training period, health workers delivered the behavioral-change strategy to caregivers and family members in enrolled households. Home visits were organized along age-specific curricula called “educational paths,” which emphasized key nutrition messages caregivers should receive based on the child’s age at each stage of the intervention. During each visit, educational paths emphasized one message from the following areas: exclusive breastfeeding and complementary feeding, responsive feeding, and hygiene (with an emphasis on handwashing). The program staff delivered messages face-to-face with the use of interpersonal communication and participatory demonstrations. They enhanced the intervention by conveying information through interactive play and performing arts (puppet shows, theater, songs, or poems). These communication strategies engaged families and caregivers at a cognitive and emotional level. Home visits lasted between 60 and 90 min and occurred once or twice per month depending on the child’s age. Children graduated from the program at two years old, regardless of their age at start.
Data collectionHousehold surveys were collected at baseline, during the first follow-up (about 30 months after baseline), and during the second follow-up (about 42 months after baseline). The research team conducted interviews with the mother or primary caregiver of every target child (child < 12 months old at baseline). They recorded information on household sociodemographic and caregiver characteristics. In both follow-up surveys, caregivers were asked detailed questions about their feeding practices and the target child’s intake of individual food groups within the last 24 h, in accordance with WHO IYCF guidelines [28]. Caregivers were also asked questions to measure their knowledge of IYCF and nutrition practices promoted by the program. The team also collected administrative data including information on program implementation, enrollment, participation, and graduation.
Sample size and powerTwo thousand and one eligible households completed the baseline survey, 1582 households completed the first follow-up survey, and 1245 completed the second follow-up survey. One thousand two hundred and thirty-four households completed both follow-up surveys. Power calculations were performed as part of the study design. Ex ante, the study was powered (power of 0.80 and significance of 0.05) to detect a 5 percentage-point change in stunting or a 0.13 SD change in height-for-age z score [25]. Ex post power calculations on the first follow-up yielded a minimum detectable effect size of 0.14 SDs in height-for-age z scores for the intent-to-treat (ITT) sample [26].
Outcome definitionsThe primary outcomes of interest for this study are defined as follows:
Knowledge index a score between 0 and 1, representing the proportion of correct responses to 43 knowledge-based questions regarding IYCF practices. All 43 components included in the index are the same between rounds. A list of individual components is presented in Additional file 1: (S1 File).
Practice index a score between 0 and 1, representing the probability of following recommended IYCF practices. Components included in this index vary between data collection rounds due to age-specific practices. The individual components included in each round are presented in Additional file 1: (S2 File).
Each index averages the components of equally weighted questions as follows:\(_=\frac^_}\), where \(_\) is the index score for household \(i\) on question\(j\), \(_\) is a binary variable equal to 1 if the caregiver responded according to recommended practices and 0 otherwise, and \(J\) is the total number of items in the index. Standardized versions of the indices were constructed as follows: \(_}}}_=\frac}}_- }}_\right)}}}_}\), where \(}}_\) is the z score for \(}\) in household\(i\), \(}}_\) is the mean of \(index\) in the control group, and \(}}_\) is the standard deviation of \(}\) in the control group.
Statistical analysesDue to limited program funds, data for the second follow-up were collected by another program that, based on its design, was only interested in households with two parents. This posed an empirical challenge for our analyses since households with both parents may have had underlying differences in demographic, socioeconomic, and health characteristics compared to single-parent households. In order to minimize potential bias due to unobserved differences between households across rounds, we limited all analyses to the balanced panel of two-parent households that were reached for second follow-up (1225). We ran balance tests for this subsample of households to check whether demographic and socioeconomic characteristics at baseline were similar between treatment and control groups. We confirmed that the balance expected from randomization of treatment holds for this subsample. We also ran balance tests between treatment and control groups for households that attrited, by design or otherwise, to check for selection bias due to attrition. Additionally, we replicated all analyses with the full sample of households to see whether our results are robust to different sample specifications. Tables with these results can be found in Additional file 1.
To compare differences in average outcomes across treatment and control groups, we estimated ITT effects based on the initial random assignment using multivariate regression analysis, with and without controlling for covariates. ITT effects were estimated using the following model:
$$_= \alpha + \beta _+ \sum_^_+ _$$
where \(_\) is the outcome of interest for household \(i\), \(_\) is a binary variable equal to 1 if assigned to the treatment group and 0 if assigned to the control group, \(\beta\) is the average ITT effect, and \(_\) is a vector of \(j\) covariates included in the regressions.
We also ran the same regression models with inverse probability weights to account for potential selection bias due to sample attrition. Weights are calculated as follows: \(_=\frac(_)}\), where \(_\) is the imputed weight for household \(i\), \(_\) is a binary variable equal to 1 if household \(i\) was observed in all rounds (not attrited) and 0 otherwise (attrited), and \(\widehat(_)\) is the estimated probability of being observed after controlling for household and caregiver characteristics.
Additional regressions were performed with interaction terms to assess potential heterogeneous ITT effects. Caregiver age (years), number of children, baseline knowledge (probability), and education (years) were dichotomized at the median and used in the interactions. The baseline knowledge indicators include 106 observations for children who were not the target child (older siblings). A dummy variable controlling for the change in the target child was added to the adjusted regression models for these indices. All statistical analyses were conducted in Stata (V.15.0).
留言 (0)