Demographic comparison
Descriptive statistics of demographic variables were computed for the three groups (i.e., health vegetarians, moral vegetarians, and omnivores) and summarized in Table 1.
The Kruskal–Wallis test revealed a significant difference in age among the three groups, χ2(2) = 14.09, p < .001. Multiple pair-wise nonparametric comparisons with a Bonferroni-type adjustment showed that health vegetarians were significantly older than moral vegetarians and omnivores; moral vegetarians and omnivores did not significantly differ in age. The Kruskal–Wallis test indicated no significant group difference in household income, urbanicity, and physical health.
A chi-square test of independence showed that the proportion of females significantly differed between groups, χ2(2) = 17.03, p < .001. Post-hoc analysis with Bonferroni correction revealed that the proportion of females was significantly higher in moral vegetarians (73.1%) than in health vegetarians (55.6%) and omnivores (47.6%); the proportion of females did not significantly differ between health vegetarians and omnivores.
Bivariate correlations in vegetarians
Bivariate correlation analyses were performed for health food choice motive (FCM), moral FCM, and other focal variables (including mediators and measures of psychological health) in vegetarians. The results were summarized in Table 2.
Table 2 Correlations between focal variablesMediation analyses in vegetarians
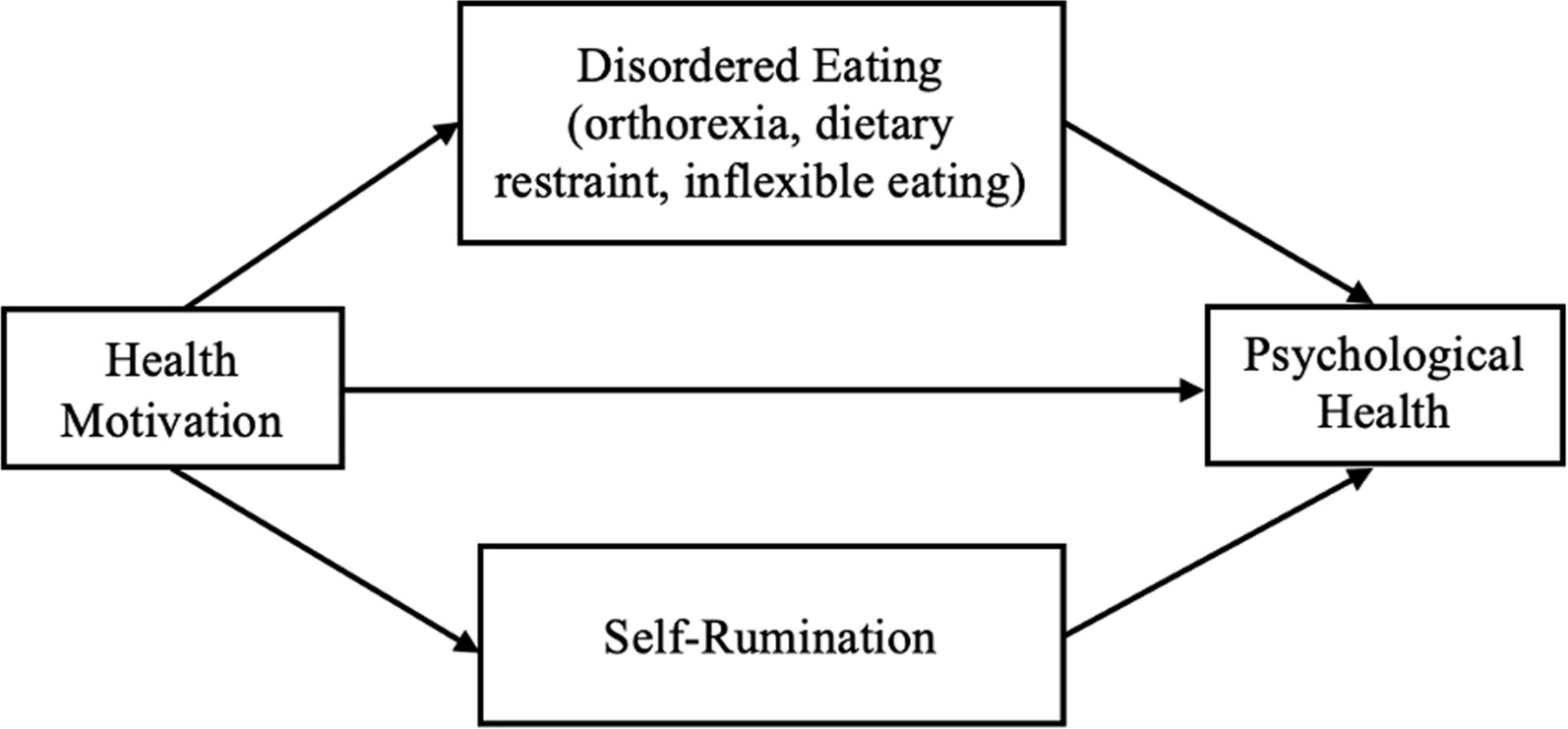
SPSS PROCESS [28] Model 4 was used to test the proposed mediation models (see Figs. 1, 2). Bootstrapping was performed with 5000 samples to test the significance of indirect effects. Mediation analyses were conducted including all vegetarians.
Given that health FCM and moral FCM were significantly correlated (r(264) = .26, p < .001), moral FCM was statistically controlled for when examining correlations with health FCM and vice versa. Age, gender (male = 0, female = 1), ethnicity (minority race = 0), urbanicity, household income, physical health, and diet type (0 = non-strict vegetarian) were also entered as covariates.
The total effects of health FCM and moral FCM on measures of psychological health were summarized in Table 3. Contrary to Hypothesis 5a, Health FCM did not have a significant total effect on any measure of psychological health. Contrary to Hypothesis 8a, moral FCM did not have a significant total effect on any measure of psychological health.
Table 3 Linear regression analysis predicting psychological health—total effects modelDisordered eating measures as mediators
To recall, three disordered eating indicators were measured: orthorexia, dietary restraint, and inflexible eating. They were entered as parallel mediators. The results were summarized in Table 4.
Table 4 Mediation analysis testing the indirect effects of health motivation on psychological health indicators via disordered eating variablesHealth FCM did not have significant indirect effects via orthorexia on depression (bindirect = .02, SEboot = .05, 95% CIboot [− .06, .09]), anxiety (bindirect = .02, SEboot = .03, 95% CIboot [− .04, .07]), and stress (bindirect = .01, SEboot = .03, 95% CIboot [− .05, .07]). Its indirect effects via inflexible eating on depression (bindirect = .05, SEboot = .04, 95% CIboot [− .02, .12]), anxiety (bindirect = .03, SEboot = .03, 95% CIboot [− .02, .08]), and stress (bindirect = .04, SEboot = .03, 95% CIboot [− .01, .10]) also did not reach significance. On the other hand, health FCM had significant positive indirect effects via dietary restraint on anxiety (bindirect = .07, SEboot = .03, 95% CIboot [.02, .12]) and stress (bindirect = .07, SEboot = .03, 95% CIboot [.02, .14]), but its indirect effect on depression was not significant (bindirect = .06, SEboot = .03, 95% CIboot [− .002, .12]).
Results showed that the indirect effects of health FCM on measures of emotional well-being via orthorexia (bindirect = − .01, SEboot = .04, 95% CIboot [− .08, .07]) and dietary restraint (bindirect = − .05, SEboot = .04, 95% CIboot [− .13, .04]) were not significant. In contrast, health FCM was found to have significant, negative indirect effects on emotional well-being via inflexible eating (bindirect = − .09, SEboot = .04, 95% CIboot [− .18, − .004]).
The indirect effects of health FCM on social well-being were not significant via orthorexia (bindirect = .01, SEboot = .05, 95% CIboot [− .08, .11), via dietary restraint (bindirect = − .07, SEboot = .05, 95% CIboot [− .17, .03]), and via inflexible eating (bindirect = − .06, SEboot = .05, 95% CIboot [− .16, .05]). The indirect effects of health FCM on psychological well-being via orthorexia (bindirect = − .01, SEboot = .04, 95% CIboot [− .09, .07]), via dietary restraint (bindirect = − .06, SEboot = .04, 95% CIboot [− .13, .02]), and via inflexible eating (bindirect = − .07, SEboot = .04, 95% CIboot [− .16, .01]) were not significant, either.
Inconsistent with Hypothesis 1a, orthorexia did not significantly mediate the relationship between health motivation and any indicator of psychological health. Consistent with Hypothesis 2a, the results suggested that health motivation was positively associated with dietary restraint, which in turn was positively associated with anxiety and stress, which are indicators of negative psychological health. Consistent with Hypothesis 3a, health motivation was positively correlated with inflexible eating, which in turn was negatively correlated with emotional well-being, an indicator of positive psychological health.
We reran the same mediation analyses excluding vegetarians whose primary motivation is neither health nor morality. The results were consistent, except that health FCM was found to have a significant indirect effect on depression via dietary restraint, bindirect = .07, SEboot = .03, 95% CIboot [.001, .13], after excluding vegetarians whose primary motivation is neither health nor morality.
Self-rumination as a mediator
The results were summarized in Table 5.
Table 5 Mediation analysis testing the indirect effects of health motivation on psychological health indicators via self-ruminationHealth FCM did not have a significant indirect effect on any measures of psychological health via self-rumination: depression (bindirect = .01, SEboot = .02, 95% CIboot [− .03, .05]), anxiety (bindirect = .005, SEboot = .01, 95% CIboot [− .02, .03], and stress (bindirect = .01, SEboot = .02, 95% CIboot [− .03, .04]), emotional well-being (bindirect = − .01, SEboot = .02, 95% CIboot [− .06, .04]), social well-being (bindirect = − .01, SEboot = .03, 95% CIboot [− .07, .05]), and psychological well-being (bindirect = − .01, SEboot = .02, 95% CIboot [− .06, .04]).
Inconsistent with Hypothesis 4a, mediation analyses showed that self-rumination did not mediate the relationship between health motivation and psychological health.
If excluding vegetarians whose primary motivation is neither health nor morality, the results were consistent.
When the three disordered eating measures and self-rumination were entered in the model, the direct effect of health FCM was not significant on any measure of psychological health: depression (b = − .01, SEboot = .05, p = .91), anxiety (b = − .06, SEboot = .04, p = .16), stress (b = − .04, SEboot = .04, p = .28), emotional well-being (b = .06, SEboot = .07, p = .36), social well-being (b = .04, SEboot = .07, p = .56), and psychological well-being (b = .11, SEboot = .06, p = .10).
Subjective dietary adherence as a mediator
The results were summarized in Table 6.
Table 6 Mediation analysis testing the indirect effects of moral motivation on psychological health indicators via dietary adherenceThe indirect effects of moral FCM via dietary adherence on depression (bindirect = − .01, SEboot = .01, 95% CIboot [− .03, .005]), anxiety (bindirect = − .01, SEboot = .01, 95% CIboot [− .03, .002], and stress (bindirect = − .01, SEboot = .01, 95% CIboot [− .03, .003]) were not significant. The indirect effects of moral FCM on measures of positive psychological health were not significant, either (emotional well-being: bindirect = .01, SEboot = .01, 95% CIboot [− .01, .03]); social well-being: bindirect = .01, SEboot = .01, 95% CIboot [− .01. .04]; psychological well-being: bindirect = .01, SEboot = .01, 95% CIboot [− .004, .04]).
Inconsistent with Hypothesis 6a, the results showed that dietary adherence did not mediate the relationship between moral motivation and psychological health, possibly because moral motivation was not significantly correlated with dietary adherence after controlling for covariates.
Of note, diet type was significantly correlated with dietary adherence even after controlling for moral motivation and other covariates, such that consuming a strict vegetarian diet (vs. non-strict vegetarian diet) was associated with better dietary adherence, which in turn was associated with lower anxiety; the indirect effect of diet type on anxiety via dietary adherence was significant, bindirect = − .08, SEboot = .04, 95% CIboot [− .16, − .01].
If excluding vegetarians whose primary motivation is neither health nor morality, the results were consistent.
Prosocial motivation and prosocial behavior as mediators
Autonomous prosocial motivation and prosocial behavior were entered as parallel mediators. The results were summarized in Table 7.
Table 7 Mediation analysis testing the indirect effects of moral motivation on psychological health indicators via autonomous prosocial motivation and prosocial behaviorUnexpectedly, autonomous prosocial motivation did not mediate the relationship between moral motives and any measure of psychological health (depression: bindirect = .02, SEboot = .03, 95% CIboot [− .03, .07]; anxiety: bindirect = .02, SEboot = .02, 95% CIboot [− .01, .05]; stress: bindirect = .03, SEboot = .02, 95% CIboot [− .01, .07]; emotional well-being: bindirect = .003, SEboot = .03, 95% CIboot [− .05, .06]; social well-being: bindirect = .01, SEboot = .03, 95% CIboot [− .05, .07]; psychological well-being: bindirect = .03, SEboot = .03, 95% CIboot [− .02, .08]). For prosocial behavior, the indirect effects on depression (bindirect = − .004, SEboot = .01, 95% CIboot [− .03, .02]), anxiety (bindirect = .01, SEboot = .01, 95% CIboot [− .003, .04]), and stress (bindirect = .01, SEboot = .01, 95% CIboot [− .01, .03]) were not significant. On the other hand, moral motivation had significant indirect effects via prosocial behavior on emotional well-being (bindirect = .03, SEboot = .02, 95% CIboot [.002, .06]), social well-being (bindirect = .07, SEboot = .03, 95% CIboot [.02, .13]), and psychological well-being (bindirect = .04, SEboot = .02, 95% CIboot [.01, .07]).
Consistent with Hypothesis 7a, moral motivation was positively associated with prosocial behavior, which in turn was positively associated with emotional, social, and psychological well-being. Contrary to Hypothesis 7a, autonomous prosocial motivation was not a significant mediator of the relationship between moral motivation and psychological health.
If excluding vegetarians whose primary motivation is neither health nor morality, the results were consistent.
When dietary adherence, prosocial motivation, and prosocial behavior were included in the model, the direct effect of moral FCM was not significant on any measure of psychological health: depression (b = − .04, SEboot = .06, p = .42), anxiety (b = − .01, SEboot = .04, p = .81), stress (b = − .06, SEboot = .05, p = .21), emotional well-being (b = .02, SEboot = .07, p = .81), social well-being (b = − .02, SEboot = .08, p = .78), and psychological well-being (b = − .003, SEboot = .07, p = .97).
Group comparisons
Mean differences between health vegetarians, moral vegetarians, and omnivores in the studied variables were examined by performing ANCOVA, with gender, age, ethnicity, household income, urbanicity, and physical health controlled for (see Table 8).
Table 8 One-way analysis of covariance in focal variables while controlling for age, gender, ethnicity, household income, urbanicity, and physical healthAs expected, there was a significant group difference in orthorexia, F(2, 291) = 32.27, p < .001. Pairwise comparisons with Bonferroni correction revealed that health vegetarians (M = 2.79, SE = .07) had higher levels of orthorexia than moral vegetarians (M = 2.39, SE = .06) and omnivores (M = 2.05, SE = .06); moral vegetarians (M = 2. 39, SE = .06) scored higher on orthorexia than omnivores (M = 2.05, SE = .06). Dietary restraint also significantly differed between groups, F(2, 291) = 3.91, p < .05. Pairwise comparisons suggested that health vegetarians (M = 3.15, SE = .11) had higher levels of dietary restraint than omnivores (M = 2.74, SE = .10); moral vegetarians (M = 2.92, SE = .09) did not significantly differ from health vegetarians (M = 3.15, SE = .11) and omnivores (M = 2.74, SE = .10). Results also revealed a significant group difference in inflexible eating, F(2, 291) = 15.60, p < .001. Pairwise comparisons showed that health vegetarians (M = 3.44, SE = .11) displayed higher levels of inflexible eating than moral vegetarians (M = 3.00, SE = .09) and omnivores (M = 2.62, SE = .10); moral vegetarians had higher levels of inflexible eating (M = 3.00, SE = .09) than omnivores (M = 2.62, SE = .10).
There was no significant group difference in self-rumination, F(2, 291) = 1.12, p = .33.
Unexpectedly, there was no significant difference in dietary adherence between health and moral vegetarians, F(1, 197) = 1.24, p = .27. The results were consistent if controlling for diet type.
A comparison of autonomous prosocial motivation suggested a significant group difference, F(2, 291) = 3.38, p < .05. Moral vegetarians (M = 5.78, SE = .11) showed significantly higher autonomous prosocial motivation than omnivores (M = 5.34, SE = .12); health vegetarians (M = 5.59, SE = .14) did not significantly differ from moral vegetarians or omnivores. On the other hand, there was no significant group difference in prosocial behavior, F(2, 291) = .18, p = .83.
The results suggested no significant group difference in depression (F(2, 291) = 1.13, p = .33) and anxiety (F(2, 291) = 2.19, p = .11). However, levels of stress significantly differed among the three groups, F(2, 291) = 4.10, p < .05. Pairwise comparisons indicated lower stress levels in omnivores (M = 1.67, SE = .07) than in health vegetarians (M = 1.94, SE = .08); moral vegetarians (M = 1.90, SE = .07) did not significantly differ from health vegetarians (M = 1.94, SE = .08) and omnivores (M = 1.67, SE = .07) in stress. Of note, the difference between moral vegetarians and omnivores in stress was marginally significant, p = .05.
There was no significant group difference in terms of emotional well-being (F(2, 291) = .09, p = .91), social well-being (F(2, 291) = .26, p = .77), and psychological well-being (F(2, 291) = .02, p = .98).
In summary, Hypotheses 1b and 3b were supported.
Consistent with Hypothesis 1b, health vegetarians had higher levels of orthorexia than moral vegetarians. Contrary to 2b, moral and health vegetarians did not significantly differ in dietary restraint. Consistent with Hypothesis 3b, health vegetarians displayed higher levels of inflexible eating than moral vegetarians. Contrary to Hypothesis 4b, moral and health vegetarians did not significantly differ in self-rumination. Contrary to Hypothesis 6b, moral and health vegetarians did not significantly differ in dietary adherence. Contrary to Hypothesis 7b, moral and health vegetarians did not significantly differ in autonomous prosocial motivation or prosocial behavior. Contrary to Hypothesis 8b, moral and health vegetarian did not significantly differ in psychological health.








留言 (0)