
記住我

Obstructive sleep apnea (OSA) is associated with cardiovascular morbidity including hypertension [1–3]. There is a multitude of pathophysiological pathways by which OSA can contribute to hypertension including hypoxia-induced sympathetic activity, endothelial dysfunction because of reduced nitric oxide levels, insulin resistance, inflammation, oxidative stress, fragmented sleep and activation of the renin–angiotensin–aldosterone system. Consequently, treatment of obstructive sleep apnea by continuous positive airway pressure (CPAP) was supposed to be a powerful nonpharmacologic antihypertensive measure. Metaanalyses, however, show only a mild effect on BP with a mean reduction of 2–3 mmHg [4].
The effect of CPAP on BP increases with baseline BP, young age, and the severity of oxygen desaturations [5,6]. Thus, CPAP has indeed an antihypertensive effect. Its magnitude, however, is substantially lower than initially expected. Initial reports – 30 years ago – described BP reductions of 10 mmHg [7]. In analogy, the expectations in an overall reduction of cardiovascular risk were hampered by the randomized controlled SAVE trial in 2016, which failed to detect a CPAP-induced prevention of cardiovascular events in patients with moderate-to-severe obstructive sleep apnea and established cardiovascular disease [8]. Noteworthy, however, the mean duration of adherence to CPAP therapy was only 3.3 h per night. These findings indicate that CPAP cannot be used to reduce BP or cardiovascular risk in a ‘one size fits all strategy’. Thus, there is an urgent clinical need to define subgroups of patients, who might have a particular cardiovascular benefit – for example, regarding a reduction of BP – by CPAP (personalized approach).
We hypothesize that the magnitude of CPAP-induced BP reduction does not only depend on baseline BP but also on baseline apnea –hypopnea index (AHI) and the extent of daytime sleepiness, assessed, for example, by the Epworth Sleepiness Scale (ESS). From a clinical point of view, it would be of high interest to define threshold values for AHI and ESS, which are associated with a high probability of a clinically relevant reduction of BP. The present study, therefore, examines, whether such cut-off values exist for the prognosis of a CPAP-induced SBP reduction at least 5 mmHg.
METHODS Study population and study designWe performed a retrospective study of polysomnographic recordings, BP, and clinical data of patients undergoing in-laboratory polysomnography in a German University Hospital. By means of an electronic data extraction approach, 2461 patients were identified that had been admitted for a first polysomnography from 2010 to 2019. The study comprised a baseline examination at first polysomnography leading to the diagnosis of sleep apnea and a follow-up examination 13.3 ± 85.9 months after initiation of CPAP therapy. Inclusion criteria for further enrollment were diagnosis of sleep apnea necessitating CPAP therapy in baseline examination and age at least 18 years. Exclusion criterion was lack of indication for CPAP therapy, preestablished CPAP therapy, central sleep apnea, ventilation modes other than CPAP and missing BP measurements at baseline and/or follow-up.
Daytime sleepiness was assessed using the Epworth Sleepiness Scale (ESS) questionnaire. Polysomnographic monitoring comprised simultaneous noninvasive recordings of electroencephalogram, electrooculogram, submental and bilateral leg electromyogram, nasal or oral airflow, oxygen saturation (pulse oximetry), snoring microphone, chest and abdominal respiratory movement, body position and electrocardiogram. Polysomnography results were scored according to standard criteria according to American Academy of Sleep Medicine guidelines by an experienced observer [9,10]. Results were interpreted by physicians with long-lasting experience in sleep medicine. The study was approved by the ethical committee of Ruhr-University Bochum (reference number 18-6725).
Clinical data were taken at baseline polysomnography and at first control polysomnography 13.3 ± 85.9 months after initiation of CPAP therapy (follow-up).
Blood pressure measurementOffice BP was assessed auscultatorily according to Riva-Rocci at admission by trained observers in a seated position in a quiet room of the laboratory after a resting time of at least 5 min. Measurements were performed at daytime during a physical examination prior to the polysomnography. The cuff size was chosen in dependence of the upper arm circumference using a standard bladder cuff 13 × 24 cm for a circumference of 24–32 cm, 15 × 30 cm for a circumference of 33–41 cm, and 12 × 22 cm for a circumference of less than 22 cm. The cuff was deflated by a maximum of 3 mmHg per second.
Statistical analysisData were checked for normal distribution by the Kolmogorov–Smirnov Test. Normally distributed data were presented as mean ± standard deviation and were compared from baseline to follow-up by a paired two-tailed t test. Categorical data and nonnormally distributed numeric data are presented as median and interquartile range (IQR). Baseline and follow-up ordinal data were analyzed by Wilcoxon signed rank test. Correlation analyses between AHI, ESS and change of BP were performed according to Pearson. Receiver-operating characteristic (ROC) curve analyses were performed in an attempt to predict a SBP reduction at least 5 mmHg and at least 10 mmHg by baseline AHI and ESS. P less than 0.05 was regarded statistically significant. All statistical analysis was done using SPSS Statistics 29 (SPSS Inc, Chicago, Illinois, USA) and GraphPad Prism 8 (GraphPad Software Inc., Boston, Massachusetts, USA).
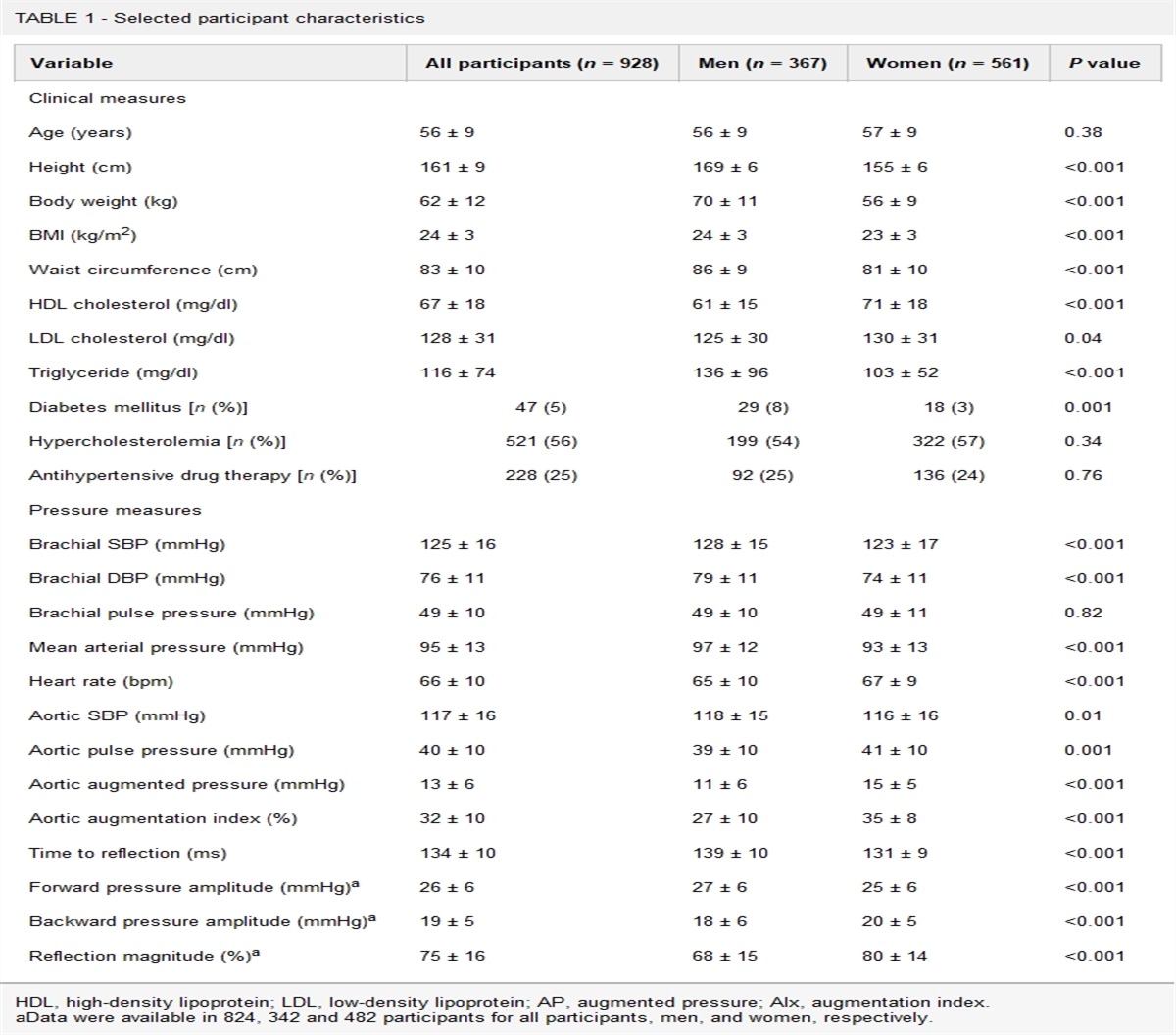
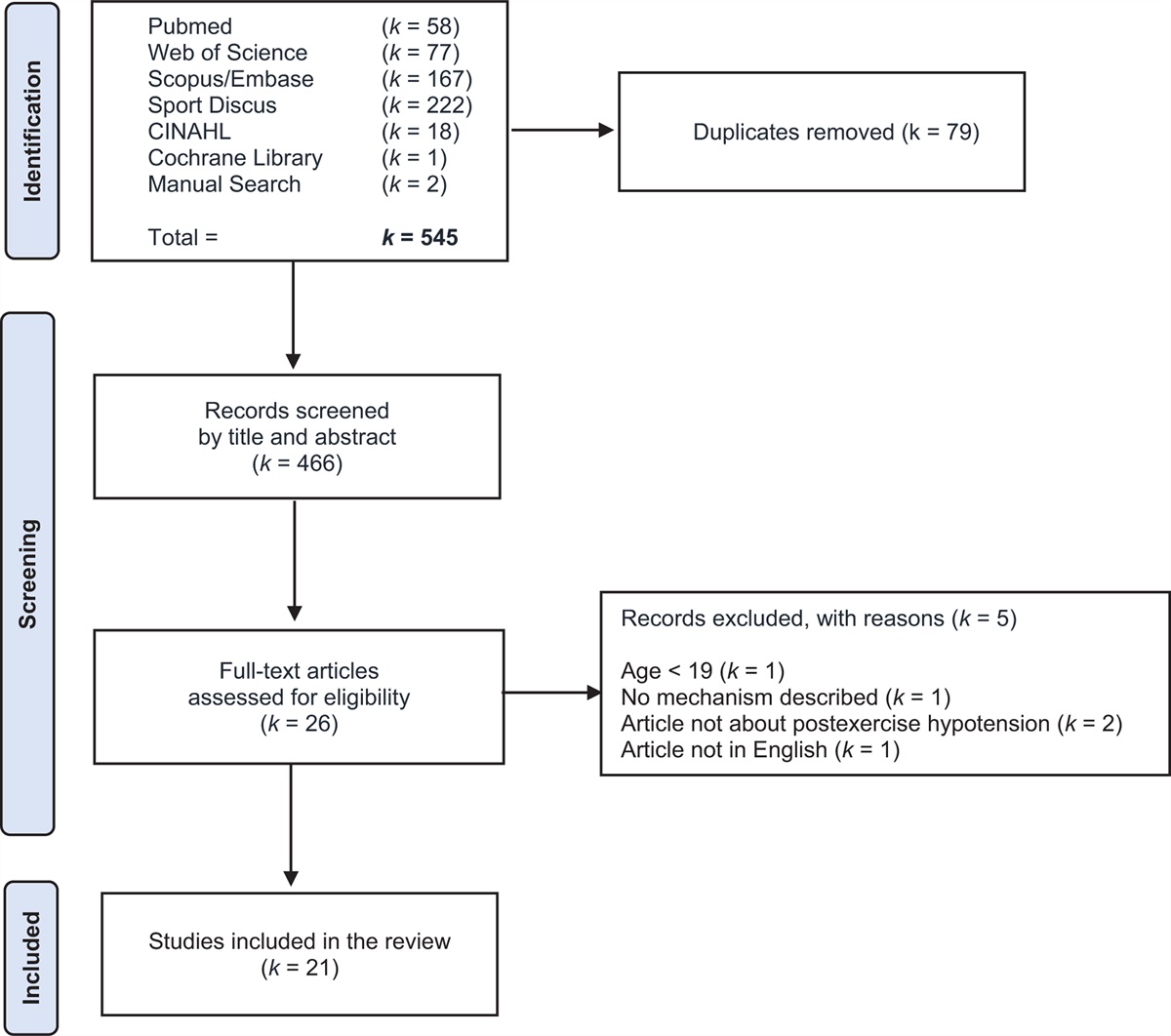
RESULTSDigital data extraction yielded data sets of 2461 patients, who were examined in our in-hospital laboratory and screened for enrolment in this retrospective analysis. A total of 555 patients were in line with all inclusion and exclusion criteria and were enrolled in the study. A detailed characterization of the study population is presented in Table 1.
TABLE 1 - Epidemiological and clinical characteristics of the study population at baseline Age (n = 555) 58.1 ± 12.7 BMI (n = 555) 30.0 (27.0–34.3) Creatinine (n = 546) 0.9 (0.8–1.1) eGFR (n = 546) 81.9 (68.0–94.0) Hypertension 398 (71.8%) Diabetes 102 (18.4%) Hyperlipidemia 96 (17.6%) Nicotine 124 (22.7%) LDL cholesterol (n = 197) 130.0 (102.5–151.0) HDL cholesterol (n = 197) 48.0 (39.0–58.0) CRP (n = 393) 0.2 (0.1–0.5) Uric acid (n = 257) 5.7 (4.9–6.6) Monthly hours of usage (n = 555) 143.7 (85.4–204.1) Numbers of antihypertensive drugs 1 (0–2) Days between baseline and follow-up (n = 555) 354 ± 361 Days under CPAP therapy (n = 555) 211 (177–268) AHI (n = 555) 21 (11–37) ESS (n = 492) 8.3 ± 4.8AHI, apnea–hypopnea index; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Age and low-density lipoprotein (LDL)-cholesterol were normally distributed (P > 0.10). Mean age was 58.1 ± 12.7 years. Median AHI was 21 (11–37) at baseline. Mean duration of adherence to CPAP therapy was 143.7 (85.4–204.1) hours per month (4.8 h per night). The follow-up examination took place after a mean of 354 ± 361 days. 71.8% of the study population had hypertension, 18.4% suffered from diabetes, 17.6% from hyperlipidemia and 22.7% reported tobacco consumption.
At baseline the median number of antihypertensive drugs were 1 (0–2). Comparing the first visit under therapy to baseline, 58 patients (10.5%) had in increase in either dosage or number of antihypertensive drugs, whereas 32 (5.8%) reported a reduction. Baseline mean SBP for the general population was 129.9 ± 15.5 mmHg, DBP was 81.7 ± 10.4 mmHg. Both, SBP and DBP decreased significantly from baseline to first follow-up with CPAP therapy (123.2 ± 15.2 mmHg, P = 0.0208 and 79.7 ± 10.7 mmHg, P = 0.0002, respectively). The change of SBP and DBP is summarized in Table 2 and Fig. 1.
TABLE 2 - Change (Δ) of blood pressure from baseline to follow-up in dependence of apnea–hypopnea index and daytime sleepiness as measured by Epworth Sleepiness Scale Blood pressure baseline Blood pressure follow-up ΔBlood pressure P Overall population (n = 555) Systolic 129.9 ± 15.5 128.3 ± 15.2 −1.5 ± 19.2 0.02 Diastolic 81.7 ± 10.4 79.7 ± 10.7 −2.1 ± 13.6 0.0002 AHI ≥21 (n = 286) Systolic 130.5 ± 15.3 128.6 ± 14.6 −1.8 ± 18.9 0.06 Diastolic 82.5 ± 10.7 80.4 ± 9.8 −2.1 ± 14.0 0.01 AHI <21 (n = 269) Systolic 129.4 ± 15.8 127.9 ± 15.8 −1.3 ± 19.0 0.18 Diastolic 81.0 ± 10.1 78.9 ± 11.4 −2.0 ± 13.0 0.01 ESS ≥8 (n = 248) Systolic 128.3 ± 14.8 127.3 ± 14.2 −0.9 ± 17.6 0.22 Diastolic 81.2 ± 10.5 79.5 ± 10.1 −1.5 ± 12.9 0.05 ESS <8 (n = 244) Systolic 129.7 ± 15.1 128.8 ± 15.0 −0.8 ± 19.5 0.42 Diastolic 82.6 ± 10.3 80.3 ± 10.2 −2.4 ± 13.2 0.01P less than 0.05 was considered significant. AHI, apnea–hypopnea index; ESS, Epworth Sleepiness Scale.
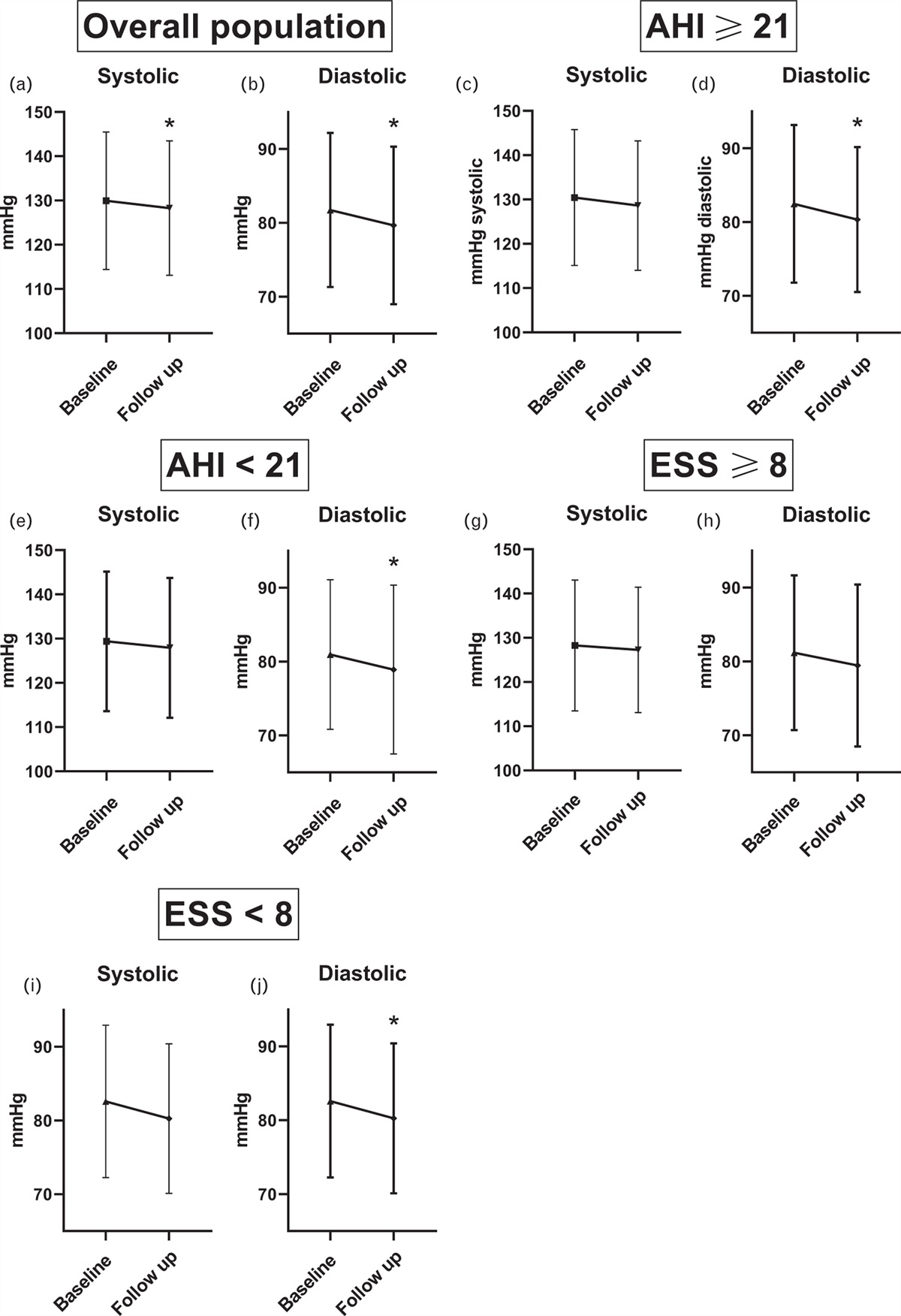
 FIGURE 1:
FIGURE 1: SBP and DBP before and 354 ± 361 days after initiation of continuous positive airway pressure therapy in n = 555 patients with sleep apnea. Plots provide mean and standard deviation) in (a and b) the overall study population, (c–f) stratified by apnea–hypopnea index (AHI) higher or lower than median, and (g–j) stratified by Epworth Sleepiness Scale (ESS) higher or lower than median. Data are provided as mean and standard deviation. P < 0.05 was considered significant.
To test the hypothesis that the number of apnea events and the intensity of sleepiness predicts the BP response to CPAP therapy, we compared subjects with AHI less than median to those with an AHI greater than median. Accordingly, the BP response of patients with an ESS less than median was compared with those with an ESS greater than median. As presented in Table 2, patients with AHI at least 21 indeed showed a numerically higher systolic and a significantly higher diastolic reduction in BP from baseline to first follow-up. The corresponding changes of BP were systolic −1.8 ± 18.9 (P = 0.06) and diastolic −2.1 ± 14.0 (P = 0.009) for AHI at least median vs. systolic −1.3 ± 19.0 (P = 0.18) and diastolic −2.0 ± 13.0 (P = 0.007) for AHI less than median. CPAP effectively reduced daytime sleepiness. ESS decreased from 8.3 ± 4.8 at baseline to 6.6 ± 4.5 at follow-up (P < 0.0001). However, patients with greater than median ESS (≥8) did not show a significantly more pronounced reduction in SBP or DBP (128.3 ± 14.8 mmHg systolic and 81.2 ± 10.5 mmHg diastolic at baseline vs. 127.3 ± 14.2 mmHg systolic and 79.5 ± 10.1 mmHg diastolic at follow-up; P = 0.22 and 0,05, respectively).
In an attempt to define an AHI and ESS cut-off value for the prediction of a SBP decrease of at least 5 or 10 mmHg, ROC analyses were performed. Areas under the curve (AUC), however, were close to 0.5 for both AHI and ESS. Thus, AUCs for a decrease of SBP at least 10 mmHg were 0.52 (AHI) and 0.50 (ESS). Accordingly, AUCs for a decrease of SBP at least 5 mmHg were 0.51 and 0.52. ROC curves and AUCs are presented in Fig. 2. Pearson's correlation analysis showed no significant association between BP response and AHI (r = 0.006; P = 0.84), nor for BP response and ESS (r = −0.01; P = 0.48).
 FIGURE 2:
FIGURE 2: Receiver-operating characteristics analysis for a continuous positive airway pressure-induced SBP difference at least 5 mmHg and at least 10 mmHg in dependence of apnea–hypopnea index (AHI) and Epworth sleepiness scale (ESS).
DISCUSSIONThe present study confirms that CPAP therapy has a mild BP-lowering effect. Patients with more severe sleep apnea have a slightly greater CPAP-induced BP reduction than those with less severe sleep apnea. Noteworthy, however, neither daytime sleepiness as measured by ESS nor the severity of sleep apnea as measured by AHI can be used to predict a strong BP reduction at least 5 mmHg. This finding is of practical clinical relevance: the idea of offering CPAP therapy to patients without relevant daytime sleepiness because of an AHI that might suggest a substantial decrease of BP has to be rejected.
The observed CPAP-induced BP reduction of 2 mmHg systolic and diastolic is in line with meta-analysis data (2.6 mmHg systolic, 2.0 mmHg diastolic) [4]. Most trials had a follow-up period of 2–3 months. We have a substantially longer follow-up period of approximately 1 year. Thus, the present analysis is able to observe long-term effects of CPAP therapy in sleep apnea. The relevance of a long-term follow-up has recently been demonstrated in a meta-analysis finding a significant BP reduction under CPAP therapy for a follow-up period more than 3 months, whereas such an effect could not be observed for shorter follow-up periods [11]. Although 72% of the study population had the diagnosis of hypertension, mean BP was normotensive at baseline (130 mmHg systolic). This is of relevance for the interpretation of our findings, as the effect of CPAP on BP increases with baseline BP [5].
It has previously been demonstrated that the severity of sleep apnea – as measured by the degree of nocturnal hypoxemia – is associated with the extent of BP decrease by CPAP treatment [12]. This finding led to the hypothesis that AHI may be used to predict the BP response to CPAP therapy. The AUC of the corresponding ROC analysis, however, is close to 0.5 indicating a very low prognostic value. In analogy, ROC analysis using ESS provided almost identical results indicating that daytime sleepiness cannot be used to predict a BP reduction of at least 5 mmHg either. The correlation analyses confirm these findings. There are several aspects that might explain these results. First, the follow-up period was long and collateral parameters like body weight, physical activity, dietary habits, and antihypertensive medication may have changed. In fact, however, only 22.8% of the study population had a change of antihypertensive medication: 12.1% of the study population had an increase, whereas 6.7% had a decrease in either dosage or number of antihypertensive drugs. Exclusion of these patients, however, did not change the study's findings. Second, as described in the introduction, the effect of CPAP on blood pressure in sleep apnea was overestimated for a long time. In the present study, only 55.5% of the patients developed a systolic decrease of at least 5 mmHg Finally, it may be scrutinized whether the quality of treatment or the patients’ adherence was too low to produce are more robust association. Indeed, adherence to CPAP therapy is negatively associated with morning BP [13]. The decrease of daytime sleepiness from baseline to follow-up and the mean CPAP use of 4.8 h per night; however, contradict these assumptions in the present population. Daily use of CPAP was thereby 1.5 h longer than in the SAVE trial.
Although the study is somewhat disappointing regarding the prediction of BP reductions at least 5 mmHg, it has to be kept in mind that the observed 2 mmHg decrease of BP is still of clinical relevance: according to metaanalysis data from randomized controlled trials, a systolic decrease of 2 mmHg corresponds to a 4% reduction of major cardiovascular events [14].
The study is limited by its retrospective character. Moreover, office BP measurements were performed ‘according to clinical practice’ and there are no 24 h ambulatory BP data. However, the vast majority of hypertension trials made use of office BP. Thus, the study's results can be well interpreted in the context of the literature. Strengths of the study are its large sample size with strictly defined inclusion and exclusion criteria, a long follow-up period and the mandatory criterion of a complete dataset for each patient. Current developments in cuffless BP monitoring may offer the opportunity to investigate the impact of CPAP on continuous BP in future studies [15].
In conclusion, this study confirms that CPAP therapy for sleep apnea has a mild BP-lowering effect. Although this effect is slightly higher in patients with above-average AHI, neither the severity of sleep apnea as measured by AHI nor the extent of daytime sleepiness as measured by ESS can be used to define threshold values predicting a BP decrease at least 5 mmHg. The decision to initiate or not to initiate CPAP therapy in patients with sleep apnea has, therefore, still to be based on the intention to reduce sleepiness and not to reduce BP.
ACKNOWLEDGEMENTS Conflicts of interestThere are no conflicts of interest.
REFERENCES 1. Pennestri MH, Montplaisir J, Fradette L, Lavigne G, Colombo R, Lanfranchi PA. Blood pressure changes associated with periodic leg movements during sleep in healthy subjects. Sleep Med 2013; 14:555–561. 2. Winkelman JW, Shahar E, Sharief I, Gottlieb DJ. Association of restless legs syndrome and cardiovascular disease in the Sleep Heart Health Study. Neurology 2008; 70:35–42. 3. Winkelman JW, Finn L, Young T. Prevalence and correlates of restless legs syndrome symptoms in the Wisconsin Sleep Cohort. Sleep Med 2006; 7:545–552. 4. Fava C, Dorigoni S, Dalle Vedove F, Danese E, Montagnana M, Guidi GC, et al. Effect of CPAP on blood pressure in patients with OSA/hypopnea a systematic review and meta-analysis. Chest 2014; 145:762–771. 5. Martinez-Garcia MA, Capote F, Campos-Rodriguez F, Lloberes P, Diaz de Atauri MJ, Somoza M, et al. Spanish Sleep Network. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension: the HIPARCO randomized clinical trial. JAMA 2013; 310:2407–2415. 6. Pengo MF, Soranna D, Giontella A, Perger E, Mattaliano P, Schwarz EI, et al. Obstructive sleep apnoea treatment and blood pressure: which phenotypes predict a response? A systematic review and meta-analysis. Eur Respir J 2020; 55:1901945. 7. Suzuki M, Otsuka K, Guilleminault C. Long-term nasal continuous positive airway pressure administration can normalize hypertension in obstructive sleep apnea patients. Sleep 1993; 16:545–549. 8. McEvoy RD, Antic NA, Heeley E, Luo Y, Ou Q, Zhang X, et al. SAVE Investigators and Coordinators. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med 2016; 375:919–931. 9. Hori T, Sugita Y, Koga E, Shirakawa S, Inoue K, Uchida S, et al. Sleep Computing Committee of the Japanese Society of Sleep Research Society. Proposed supplements and amendments to ’A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects’, the Rechtschaffen & Kales (1968) standard. Psychiatry Clin Neurosci 2001; 55 (3):305–310. 10. Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, et al. American Academy of Sleep Medicine. Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 2012; 8:597–619. 11. Shang W, Zhang Y, Liu L, Chen F, Wang G, Han D. Benefits of continuous positive airway pressure on blood pressure in patients with hypertension and obstructive sleep apnea: a meta-analysis. Hypertens Res 2022; 45:1802–1813. 12. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, Mullins R, Jenkinson C, Stradling JR, Davies RJ. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002; 359:204–210. 13. Hoshide S, Yoshida T, Mizuno H, Aoki H, Tomitani N, Kario K. Association of night-to-night adherence of continuous positive airway pressure with day-to-day morning home blood pressure and its seasonal variation in obstructive sleep apnea. J Am Heart Assoc 2022; 11:e024865. 14. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016; 387:957–967. 15. Hoshide S, Yoshihisa A, Tsuchida F, Mizuno H, Teragawa H, Kasai T, et al. Pulse transit time-estimated blood pressure: a comparison of beat-to-beat and intermittent measurement. Hypertens Res 2022; 45:1001–1007.
留言 (0)