
記住我
Dear Editor,
Auricular skin cancers represent 6–10% of cutaneous head and neck malignancies, basal cell carcinomas (BCC) and squamous cell carcinomas (SCC) being the most common.1 Other tumours such as lentigo maligna (LM), malignant melanoma (MM), Merkel cell carcinoma (MCC), or pleomorphic dermal sarcoma (PDS) can also develop in this area2 [Figure 1].

Export to PPT
The auricles, having a unique, three-dimensional structure and essential aesthetic role, are part of the facial “high-risk” H-zone.3 Their anatomy, with a thin skin layer overlying cartilage, little subcutis, and proximity to lymphatic channels, increases the risk of tumour invasion and progression.3
We retrospectively reviewed charts of 529 patients with auricular skin cancer referred to our department between 2000–2022. We assessed patients’ gender, age, tumour type, anatomical location, and documented recurrence. The data cleaning, tables, figures, and statistical tests were performed using R Studio version 2022.07.2.
All procedures were performed as per the ethical standards of the 2013 Declaration of Helsinki, and Ulm University Medical Ethics Committee approved this retrospective chart review (No.437/22).
Of 529 patients, 439 (82.99%) were male (M) and 90 (17.01%) female (F), with an M: F ratio of 4.8:1, data consistent with previously reported male sex predominance.4 The mean age distribution was 74.7 years for M and 72.3 years for F at diagnosis, suggesting cumulative sun damage as the main carcinogenesis factor. The patients’ characteristics are illustrated in Table 1.
Table 1: Patients’ characteristics according to gender, age, tumour type and tumour side (i.e., left/right)
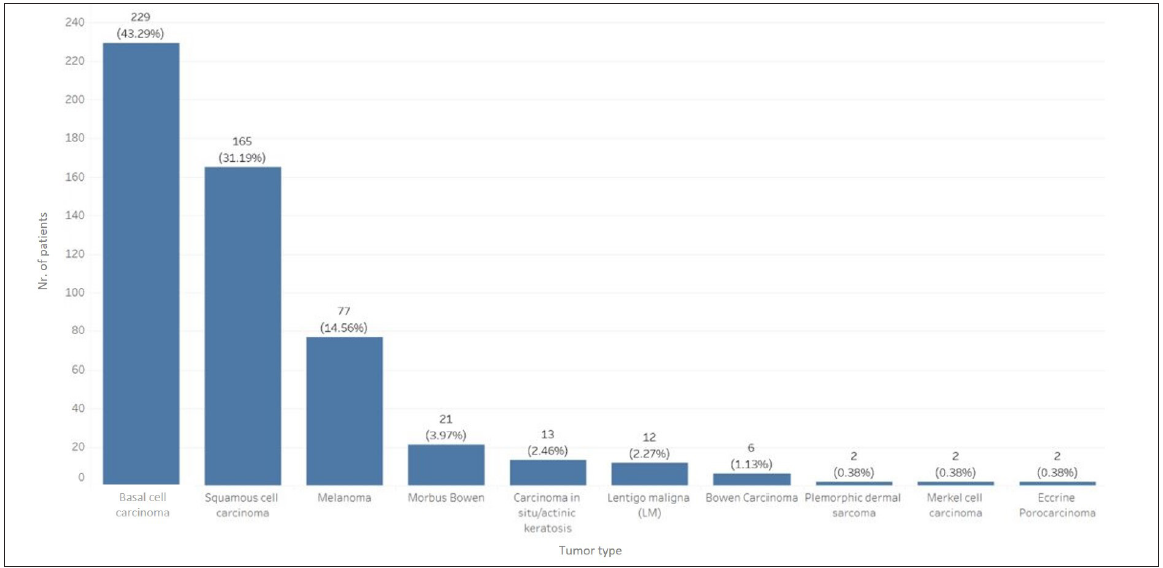
M (N = 439) F (N = 90) Overall (N = 529) Age (years) Mean (SD) 74.7 (10.3) 72.3 (14.6) 74.3 (11.2) Median [Min, Max] 76.0 [28.0, 95.0] 76.0 [25.0, 92.0] 76.0 [25.0, 95.0] Histology BCC 180 (41.0%) 49 (54.4%) 229 (43.3%) Lentigo maligna 11 (2.5%) 1 (1.1%) 12 (2.3%) Melanoma 39 (8.9%) 14 (15.6%) 53 (10.0%) Other 58 (13.2%) 12 (13.3%) 70 (13.2%) Squamous cell carcinoma 151 (34.4%) 14 (15.6%) 165 (31.2%) Tumour side Left 233 (53.1%) 47 (52.2%) 280 (52.9%) Right 206 (46.9%) 43 (47.8%) 249 (47.1%)BCC was the most common auricular tumour (43.2%), followed by SCC (31.9%), MM (14.5%), LM (2.27%), Bowen carcinoma (1.13%), and PDS (0.38%). The BCC/SCC ratio was 1.19:1 for M and 3.5:1 for F, showing an apparent BCC predilection in female patients [Figure 2].
Export to PPT
52.9% of lesions developed on the left auricle, while 47.1% on the right, with no significant gender-related difference. It was suggested that the left auricle is more prone to extensive sun exposure and carcinogenesis due to seating position while driving.5 Regarding tumour type and location (left vs. right), the Chi-square test could not find any statistically significant association (p = 0.77).
For the association between tumour type and gender, Fisher’s test showed that female patients are more likely to develop auricular BCCs and MMs, while male patients instead develop SCCs (p = 0.002) [Table 1].
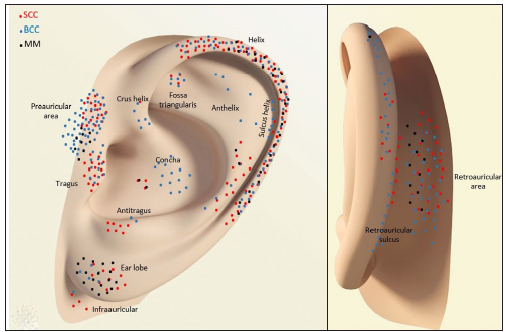
The helix was the predilection site for BCC (26,6%), followed by preauricular (23.6%), retroauricular (19.7%) and concha area (6.1%). For SCC, the predilection site was the helix (40.6%), followed by retroauricular (15.8%), preauricular area (10.9%), and antihelix (6.7%), while for MM, the commonly involved auricular subunits were helix (30.2%), earlobe (26.4%) and retroauricular area (24.5%) [Figure 3a].
Export to PPT
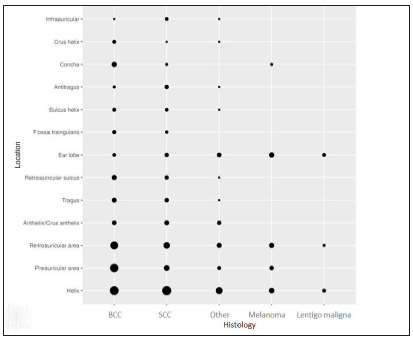
The distribution of auricular tumours according to the anatomic subunit is illustrated in Figure 3b.
Export to PPT
No hypothesis tests for relapse and tumour type variables for NMSC were conducted due to missing values and patients lost to follow-up. However, from 229 BCCs, 2 cases of sclerodermiform BCC relapse (0.8%), known for their high recurrence risk was documented. Five out of 165 SCCs (3%) relapsed with locoregional metastases, out of which 2 were in immunosuppressed patients, a known factor for increased metastatic risk.6
From 53 MM subjects, 2/13 patients with retroauricular MM (15.3%) had stage IV disease with lung metastasis at diagnosis, whereas 3/16 patients with helix MM (18.7%) progressed to stage IV within a few years. Four out of 8 patients with preauricular MM (50%) and 1/14 earlobe MM (7.14%) showed locoregional progress with cervical/ parotid metastases during follow-up. In our cohort, there was no particular difference in lymphatic spread depending on the anatomic subregion, probably because 2/3rd of subjects were American Joint Committee on Cancer (AJCC) stages IA-IIB with an uneventful follow-up.
The helix was our cohort’s most common subunit for skin cancers, followed by retroauricular, preauricular area, and earlobe. The most common tumours were BCC, SCC, and MM, and the rare ones were MCC or PDS. Our data showed that the retroauricular area is a predilection site for MM, demonstrating a role of other factors for MM development besides UV exposure. Furthermore, in 2 cases of retroauricular MM, patients were diagnosed in stage IV, suggesting the late identification of the primary tumour hidden by the auricular framework and hair.
We found a significant predominance of auricular skin cancer in men in the 7th decade; for SCC specifically. This fact is known, as previous studies found an M:F ratio of 22:1, probably because women benefit from their longer hair, i.e., a factor of sunlight reduction7
Our analysis also revealed a new aspect of gender-related tumour distribution: the women in our cohort were more prone to develop BCCs and MM in the auricular area compared with men who develop SCCs. This new information is of interest when managing suspicious auricular lesions: a thorough examination of the auricular subunits during screening is essential, as tumours can be overseen in the retroauricular region or hidden anatomic subunits of the auricular framework, leading to delayed diagnosis and therapy.
留言 (0)