
記住我

Between 13 April and 25 July 2023, 699 participants provided consent. Of these, 502 eligible respondents completed the demographics and AGT-Eye questionnaire, and 477 respondents completed all survey instruments (Supplementary Fig. 1). After excluding participants residing in Australia (n = 6), data from 496 participants were included in the primary analysis set (Participant characteristics shown in Table 1 and Supplementary Table 3).
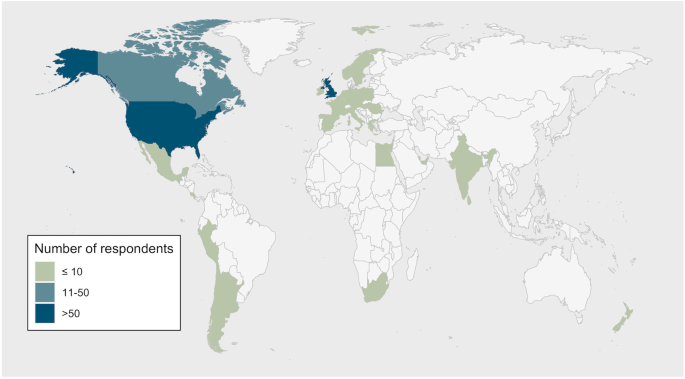
Table 1 Participant characteristics of the multinational survey cohort (n = 496).Data included participants from 35 countries (Fig. 1). Most responses were from high income countries (96%), with respondents from the United States of America (USA; 69%) and United Kingdom (UK; 11%) constituting 80% of the study sample. English was the primary language reported by 87% of participants.
Fig. 1: Country of residence of participants who participated in the multinational survey (n = 496).
Respondents from Australia (n = 6) were excluded from the analysis.
Most responses were from adults with IRDs (89%; n = 439; mean age 55.6 [14.4] years); 7% of respondents were parents/guardians/carers of people with IRDs <18 years of age (n = 36; mean age 44.8 (8.6) years), and 4% were parents/guardians/carers of people with IRDs >18 years of age (n = 36; mean age 46.2 (14.5) years).
Adult respondents predominantly reported having retinitis pigmentosa (62%), Stargardt disease (13%), or other macular dystrophies (6%); 2% of adult respondents had Leber Congenital Amaurosis (Fig. 2). The main presenting symptoms reported at disease onset were difficulty seeing at night/dusk (66%) and difficulty adjusting from light/dark (49%; Supplementary Table 3). In contrast, parents/guardians/carer responders were largely of dependents with retinitis pigmentosa (35%), Leber Congenital Amaurosis (26%), and Stargardt disease (18%).
Fig. 2: Self-reported diagnoses of survey respondents (n = 496).
Responses shown from adults with IRDs (n = 439) or as reported of their dependent by parent/caregivers (n = 57).
Figure 3 shows participants’ attitudes towards gene therapy and medical research. Only 27% of participants have previously participated in medical research, but 70% have supplied DNA to an IRD database. Most respondents (61%) indicated that they had never previously received any treatments for their (or their dependent’s) IRD (Fig. 3B). Those who had mostly had vitamin A treatments (28% of all respondents), and less commonly herbal remedies (8%), acupuncture (5%), and electrical stimulation (4%). Two adult participants with IRDs (0.4% of all responses) had previously received stem cell treatment.
Fig. 3: Participants’ attitudes towards gene therapy and medical research (n = 496).
A Likelihood of taking up gene therapy if offered for their condition. B Previous treatment for inherited retinal disease. C Perceived barriers to receiving gene therapy for inherited retinal diseases. IRD inherited retinal disease.
Over 90% participants said that they were very likely (73%) or likely (18%) to take up gene therapy if this was available to them (Fig. 3A). Only 6 participants (1.2%) said that they were unlikely or very unlikely to take up ocular gene therapy. Approximately one-third of respondents (32%) reported no barriers to getting gene therapy (Fig. 3C). The main barriers among both adults with IRDs and parents/guardians were cost of treatment (38% of all respondents), fear of side effects (27%), early phase roll-out of treatment (22%), and fear that treatment may not work (18%). Other barriers include lack of awareness about available treatments for their IRD or inadequate discussion of options (9%), causative gene has not been identified from genetic testing (1%), limited ability to travel for treatment access, fear of further vision loss, and apprehension about ineligibility for future treatments (each <1% of respondents).
Attitudes to gene therapy (AGT-Eye) item scoresSources of informationResponses to all AGT-Eye items are shown in Supplementary Table 4. Figure 4 shows the sources where participants obtained information about gene therapy, which were primarily research registries (e.g., the Foundation Fighting Blindness registry; 60% participants) and internet (61% of all participants). Among all respondents, less than a third agreed that they received information about gene therapy from each of their ophthalmologist (30%), other medical or health professionals (28%), research groups (30%), or patient support groups (19%). Other sources of information, including social media (21%) and family/friends (17%), were less common.
Fig. 4: Reported sources of information about gene therapy.
Sources reported from adults with IRD (n = 439), compared to parent/guardian/carers of a dependent with an IRD (n = 57).
Both parent/guardians (compared to affected adults) and participants who were more likely to take up gene therapy had higher sources of information subscale scores, indicating that they were more likely to have obtained information about gene therapy from different sources (Fig. 4). There were no differences between sources of information subscale score between age groups, gender, education levels, and self-reported vision status (Supplementary Table 5).
Knowledge of gene therapy methodsDespite most participants understanding the difference between an experimental treatment provided in a clinical trial and a treatment that has already been approved by the government (93%), less than half thought they had a good knowledge of gene therapy (45% agreed/strongly agreed).
In the “knowledge of methods” subdomain (Fig. 5), 71% of all respondents knew that gene therapy and stem cell therapy are not the same treatment. However, only 47% knew that gene therapy for the eye is not injected into the blood stream through the arm, while a similar number of respondents (47%) neither agreed nor disagreed, indicating that they are uncertain of the details of the treatment delivery method. Less than a third of all respondents were aware that gene therapy for the eye may not be suitable for all stage of disease (29%), while 31% agreed/strongly agreed with the statement that generally, gene therapy for inherited retinal disease is delivered to both eyes.
Fig. 5: Participant responses to the attitudes to gene therapy for the eye questionnaire (n = 496).
Response frequencies shown for the knowledge of methods, awareness of potential outcomes, and perceived value of treatment subdomains.
Adult participants with IRDs (compared to parent/guardians) and participants with higher levels of education scored relatively higher in the “knowledge of methods” subscale. There was no difference in subscale scores between age groups, gender, central/widespread IRD, self-reported eyesight levels, or by participants’ likelihood of taking up gene therapy (Supplementary Table 5).
Awareness of potential gene therapy outcomesMost participants agreed that the main goal of ocular gene therapy is to slow down the disease (63%). However, in the next question, over half (53%) also indicated that the main goal of ocular gene therapy is to restore vision back to normal (Fig. 5). Half (51%) agreed that treatment complications, such as permanent blindness, are possible with an approved gene therapy, and 35% knew that ocular gene therapy treatments can have side effects elsewhere in the body.
Most (77%) participants agreed that having gene therapy for their eye condition does not stop them passing on the gene to their children, and agreed that gene therapy for IRDs will require many years of follow-up with their eyecare practitioner (70%). However, approximately half of all respondents were not sure if: (i) receiving gene therapy for their IRD means they wouldn’t be eligible for future genetic treatments (52%); (ii) if they undergo gene therapy, it would affect their eligibility or terms of conditions in life, disability or health/medical insurance in the future (50%); and (iii) they might not be eligible for financial or other government benefits if gene therapy for their eye condition is successful (48%).
Younger participants and those who were more likely to accept gene therapy scored higher in the AGT-Eye’s “awareness of outcomes” subscale. There were no other differences in the “awareness” subscale scores between respondent type, gender, central/widespread IRD, self-reported eyesight levels (Supplementary Table 5).
Perceived value of treatmentOver 75% of participants would consider travelling to another country to access gene therapy for their condition, if it was not available in their local area. While two-thirds (67%) of respondents agreed that government subsidy of ocular gene therapy would be an effective use of taxpayer money, only one-third (36%) indicated that the government, and half (51%) that private health/medical insurance, should pay for all associated costs of ocular gene therapy treatment. While 65% of respondents would consider a payment plan for their gene therapy, 12% disagreed.
Perceived value of treatment was related to participants’ age, education levels, and likelihood of taking up gene therapy, as younger participants, those with higher levels of education, and those more likely to take up gene therapy had higher subscale scores. There were no differences in the perceived value of treatment scores between adults with IRD/parent guardians, gender, central/widespread IRD, self-reported eyesight levels (Supplementary Table 5).
Relationship between AGT-Eye and other instrument scoresThere was a weak to moderate correlation between each of the AGT-Eye subscale scores (Supplementary Table 6), with the strongest correlation between knowledge of methods and each of information sources (ρ = 0.50 [95% CI: 0.43–0.56]), awareness of outcomes (ρ = 0.29 [95% CI: 0.20–0.37]), and perceived value of treatment (ρ = 0.19 [95% CI: 0.10–0.27]).
Supplementary Tables 7–10 show the distribution of NEI-VFQ-25, PACT-22, and EQ-5D-5L scores and their correlations with AGT-Eye subscale scores. The median NEI-VFQ-25 composite score was 53 (IQR: 39–67), from a range of 0–100, and EQ-5D-5L scores were 0.78 (IQR 0.65–0.90, utility value score) and 80 (70–88, VAS; Supplementary Table 9). Weak or no correlation was found between AGT-Eye subscale and each of NEI-VFQ-25 or EQ-5D-5L scores (Supplementary Table 10). Between the quality of life instruments, there was a weak to moderate correlation between NEI-VFQ-25 and each of EQ-5D-5L utility (ρ = 0.62 [95% CI: 0.56–0.68]) and visual analogue scale (ρ = 0.25 [95% CI: 0.16–0.34]) scores.
Regarding participants’ attitudes towards clinical trial participation, responses showed strong positive sentiments across various PACT-22 domains: positive beliefs (median score 88 [IQR: 75–100]), safety (75 [69–88]), information needs (88 [75–100]), and patient involvement (75 [62–88]; Supplementary Table 7). Negative expectations were low (46 [38–58]). Comparing AGT-Eye scores with participants’ attitudes towards clinical trial participation scored using PACT-22, a weak correlation was evident between knowledge of methods and each of positive beliefs (ρ = 0.30 [95% CI: 0.21–0.38]) and safety (ρ = 0.26 [95% CI: 0.18–0.35]), and between value of treatment and each of positive beliefs (ρ = 0.26 [95% CI: 0.17–0.34]), safety (ρ = 0.27 [95% CI: 0.19–0.36]), and information needs (ρ = 0.20 [95% CI: 0.11–0.28]). There was weak or no correlation between AGT-Eye subscale scores and the other PACT-22 domains (Supplementary Table 8).
Comparison between current international survey and 2021 Australian survey dataOverall responses and instrument scoresData from this multinational survey were compared to data from an Australian national survey of people with IRDs (n = 639) or their parents/caregivers (n = 42) [10, 11] administered in 2021. A similar number of individuals in both surveys had participated in medical research, but more participants from the USA had previously supplied DNA to a research database (75% compared to 60% in Australia, and 59% in other countries). Adults with IRDs in the USA had relatively higher NEI-VFQ-25 composite scores (mean (SD): 54.5 (19.8)) than those from Australia (49.6 (15.3)) and other countries (50.6 (18.7)). For PACT-22 domains, USA respondents had lower scores in the positive beliefs, safety, information needs, and patient involvement domains, but also less negative expectations than respondents from Australia and other countries (Supplementary Table 11). Over 90% of USA-based respondents are likely/very likely to get gene therapy if this was available to them, similar to 92% of respondents in Australia, and 93% in other global regions.
Comparison of AGT-Eye responses between USA and AustraliaWe compared AGT-Eye individual item responses between respondents from Australia and the USA, as USA residents constituted the major cohort from the international survey (Supplementary Table 12). Participants in the USA scored higher in the sources of information (mean (SD): 2.6 (0.7) versus 2.4 (0.9); adjusted p = 0.001) and knowledge of treatment methods (3.5 (0.5) versus 3.3 (0.4); p < 0.001) subscales, while Australian participants scored higher in the perceived value of treatment subscale (3.7 (0.5) versus 3.6 (0.6); p < 0.001).
Compared to Australian residents, respondents from the USA had higher self-rated knowledge about gene therapy for IRDs (41% vs 28% Australian reporting good knowledge; p = 0.007), and correctly indicated that gene therapy for the eye is not injected into the blood stream through the arm (45% vs 25% Australian respondents; p < 0.001) and that gene therapy and stem cell therapy are not the same treatment (68% vs 47% Australian residents; p < 0.001). For sources of information, USA residents reported research registries as a main information source (59% agreed vs 27% agreed in Australians, p < 0.001), and more Australian residents reported receiving information from family and friends (22% vs 17% in USA).
Regarding the perceived value of treatment, more Australian than US respondents believed that the government should pay all costs of gene therapy (43% versus 26%; p < 0.001), and that government subsidy of their treatment would be an effective use of taxpayer money (79% versus 64%; p < 0.001). There were no differences in participants’ willingness to travel to access gene therapy, or to consider a payment plan for gene therapy treatment.
留言 (0)