
記住我
Dear Editor,
X-ray is an indispensable diagnostic imaging tool with multiple indications. Being an ionising radiation, X-rays are carcinogenic. We report a case of squamous cell carcinoma (SCC) of the right thumb in a radiographic technician who exposed his hands to the X-ray and developer solution for a prolonged period.
A 45-year-old male, X-ray technician by occupation, presented with a non-healing ulcer on his right thumb of 5 years’ duration. He was treated elsewhere with multiple courses of antibiotics and antiseptic wound dressing without appreciable improvement. On enquiring, he revealed dipping of his right hand into the X-ray developer solution several times daily for 20 years. He also exposed his right hand frequently to the X-ray beam to hold the film while performing dental radiography. He has been performing about ten dental radiographic imaging daily for the past 20 years. He has no past or family history of cutaneous malignancies.
On examination, there was a single ulcero-proliferative lesion involving his dorsal right thumb extending from the hyponychium until 2 cm distal to the metacarpophalangeal joint. There was anonychia and an increased girth of the right thumb. Poikilodermatous changes involved his palms and fingers, while hyperpigmented keratotic lesions affected the palms. Poikiloderma and keratotic lesions were more prominent over the right hand. X-ray of the right hand showed resorption of the terminal thumb phalanx [Figure 1]. A single enlarged lymph node was palpable in the right axillary region (central group) which was mobile, firm, and non-tender.

Export to PPT
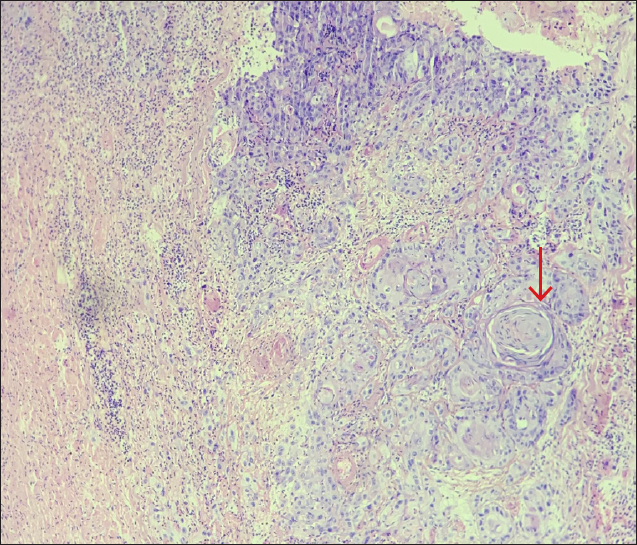
A biopsy from the ulcer margin confirmed the clinical diagnosis of SCC. Biopsy of the palmar keratotic lesion revealed hyperkeratosis, and parakeratosis without any neoplasia. Fine Needle Aspiration Cytology (FNAC) from the enlarged right axillary lymph node revealed reactive lymphoid hyperplasia. A thorough systemic workup ruled out systemic metastasis. Under general anaesthesia, amputation of the right thumb was performed at the level of metacarpophalangeal joint and complemented the defect with flap coverage. Dissection of the level 1 and level 2 axillary lymph nodes (except Rotter’s lymph nodes) and the adjoining fibro-fatty tissue was performed in the same sitting [Figure 2]. Histologic examination of the amputated specimen revealed moderately differentiated SCC with surrounding dense desmoplastic reaction and lympho-vascular invasion. [Figure 3] Tumour deposits were observed in 2 of the 39 dissected axillary lymph nodes. Adjuvant chemotherapy is being planned for the patient.

Export to PPT
Export to PPT
X-ray, being an ionising radiation, can induce double-stranded breaks in the cellular DNA which can progress to carcinoma in the absence of repair or apoptosis.1 The reported patient has been holding periapical film with his hands (right > left) for more than 20 years while performing dental radiography, and exposing his hands to 300 mA X-ray beam. As per guidelines of the International Commission on Radiological Protection (ICRP), cumulative X-ray exposure should be less than 50 mSv per year and less than 100 mSv in 5 consecutive years.2 The X-ray exposure in the present case during each exposure was 0.2 mSv. Thus, the cumulative exposure amounted to 600 mSv per year and 3000 mSv in five consecutive years which greatly exceeds the recommended safety limit.
The patient also immersed his bare right hand into the developer solution frequently for 20 years. The X-ray developer solution contains hydroquinone and its carcinogenic potential is evident through previous reports of SCC on the face following its usage as a bleaching agent.3 Apart from the present case, there is a single report, describing SCC involving the right thumb in a radiographic technician due to occupational exposure.4
The radiation emitted by the dedicated dental X-ray machine being used widely is 0.005 mSv per exposure which is much less than the radiation emitted by the 300-mA machine used by our patient.5 The usage of intra-oral film holders will also prevent X-ray exposure to the radiographer’s hands.
We report this case of occupational SCC caused by prolonged exposure of hands to X-ray. Hydroquinone in the developer fluid may be an additional contributor for carcinogenicity. Our case emphasises the importance of strict adherence to the radiation protection guidelines while performing the radiographic procedures.
留言 (0)