
記住我
Ultraviolet (UV) light has been an integral part of the dermatological examination, primarily in the form of the Wood’s lamp, which uses ‘black light’ having a peak output wavelength of 365 nm and aids in the diagnosis of conditions like pigmentary disorders (vitiligo, melasma, naevus depigmentosus) and superficial (fungal and corynebacterial) infections. Some other indications for which the Wood’s lamp can be used include – evaluation of Cutibacterium acnes, which can produce an orange-red colour in pilosebaceous follicles, pseudomonas infections which can produce a green fluorescence, and also porphyrias.1 The Wood’s lamp can also be used in the evaluation of premature canities and compliance regarding the use of sunscreens.2,3
UV dermoscopyUV reflectance dermoscopy (UVRD) is a relatively new innovation, combining dermoscopy with UV light evaluation. Like the Wood’s lamp, UV dermoscopy can be useful in pigmentary disorders such as vitiligo and melasma. Lesional margins, perifollicular pigmentation, and depigmentation can be better appreciated under UV dermoscopy as compared to normal dermoscopy.2 Dermoscopy with near-UV light can highlight demarcation of the distribution of melanin in cutaneous melanoma.4
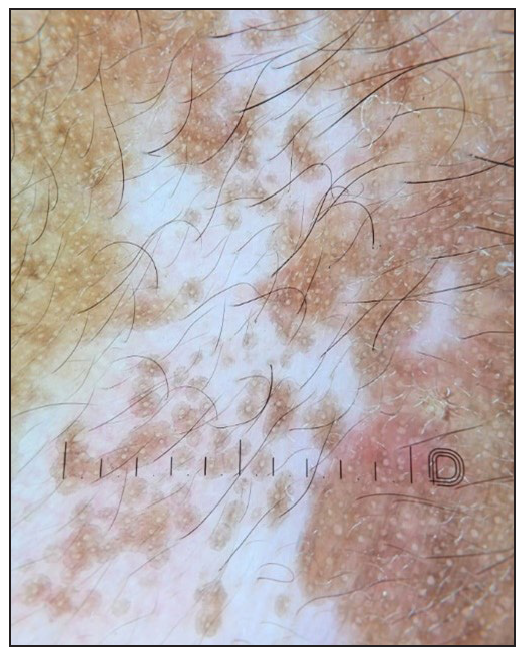
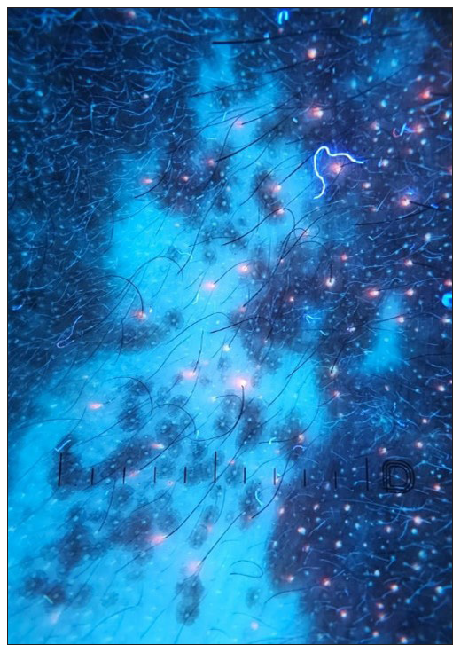
Sebaceous gland openings can show fluorescence under UVRD – ranging from bright blue/green to yellow, orange, or red. This could possibly be useful in the diagnosis and follow-up of acne vulgaris [Figure 1]. The same principle has been used to differentiate Fordyce’s spots from its mimickers. On normal polarised dermoscopy, Fordyce’s spots present as whitish-yellow clods, clustered together. Under UVRD, the fluorescence at the tip of the sebaceous opening can be seen over the less prominent, ill-defined yellow-green clods.5
Export to PPT
UVRD has been shown to be useful in the diagnosis of scabies too. UVRD of scabietic burrows highlights the blue fluorescence of the burrow and can also visualise a bright green fluorescence from the female mite’s body.6
UVRD showing prominent yellowish-green fluorescence has been reported in trichomycosis axillaris.7 Pink glow on UV dermoscopy has been identified as a helpful sign for the diagnosis of subungual glomus tumour.8
Other applications of UVRDSome other indications in which we found UVRD useful include:
–
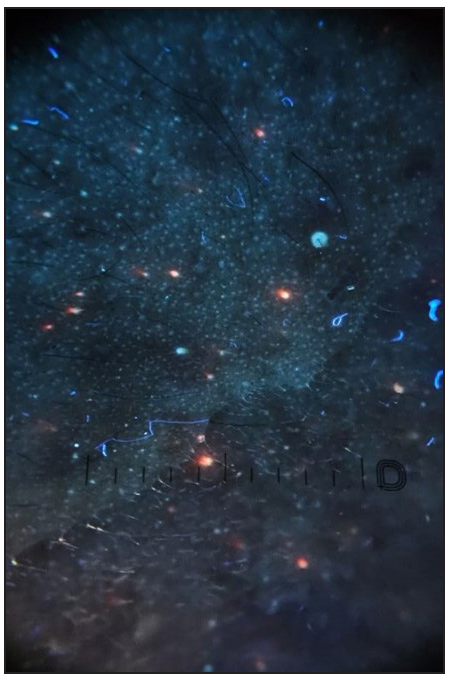
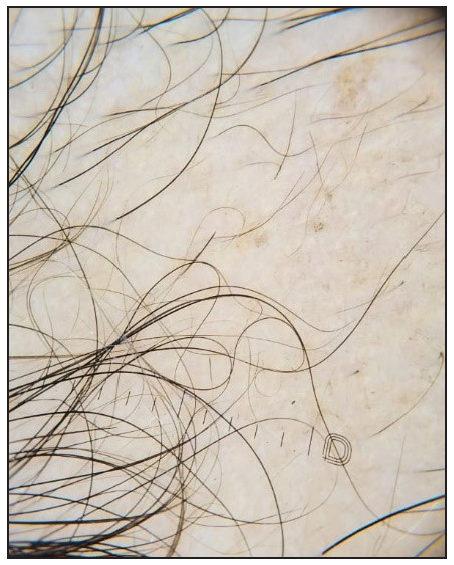
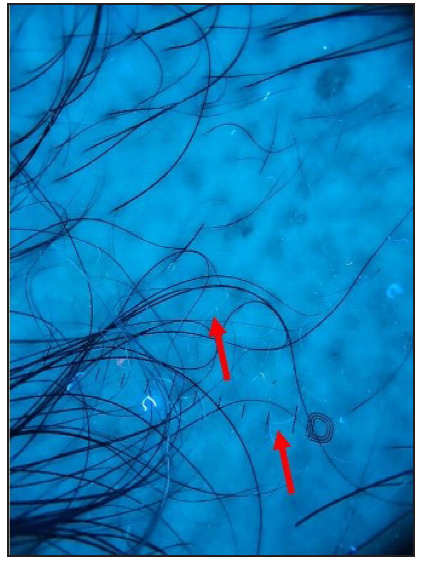
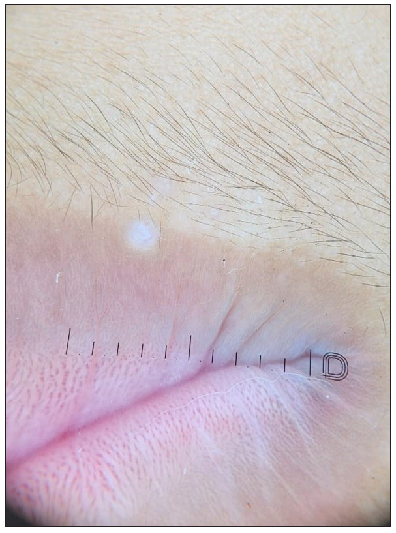
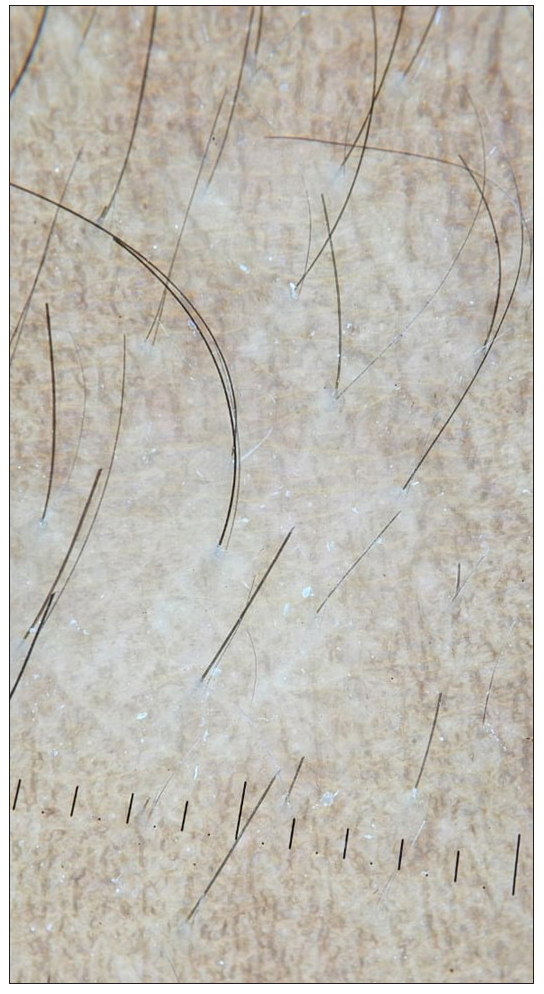
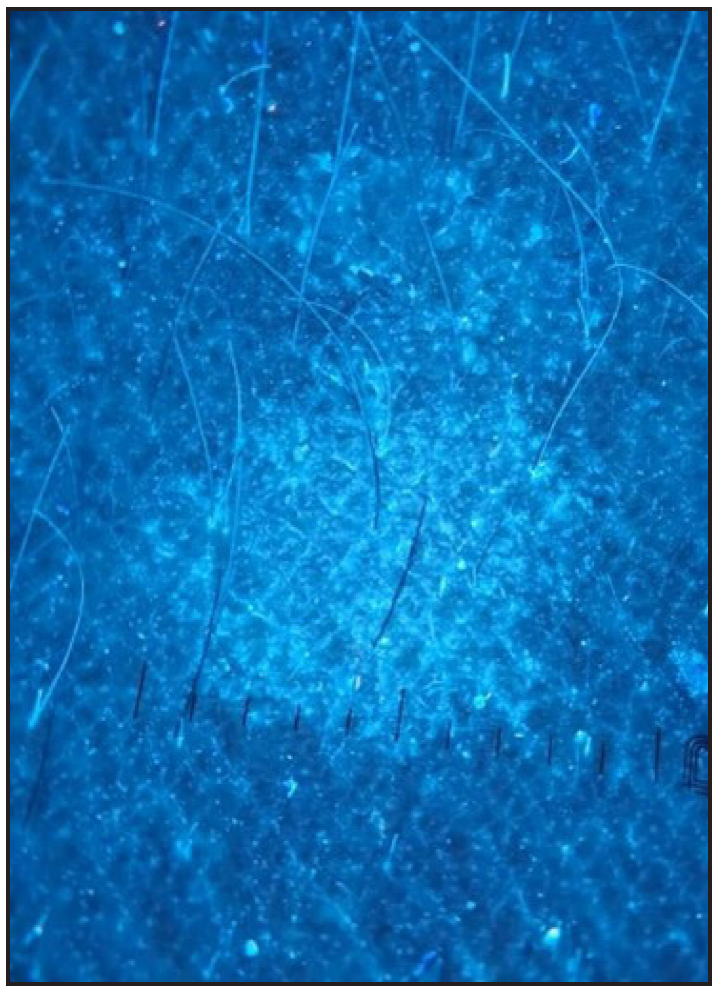
Evaluation of premature canities - like the Wood’s lamp examination, UVRD can highlight the grey hairs better. Similarly, it can help in the evaluation of fine regrowing hairs in alopecia areata (AA). Fine, regrowing hairs in AA can be devoid of pigment. UVRD picks up these hairs better as compared to standard dermoscopy [Figures 2a and 2b].
–
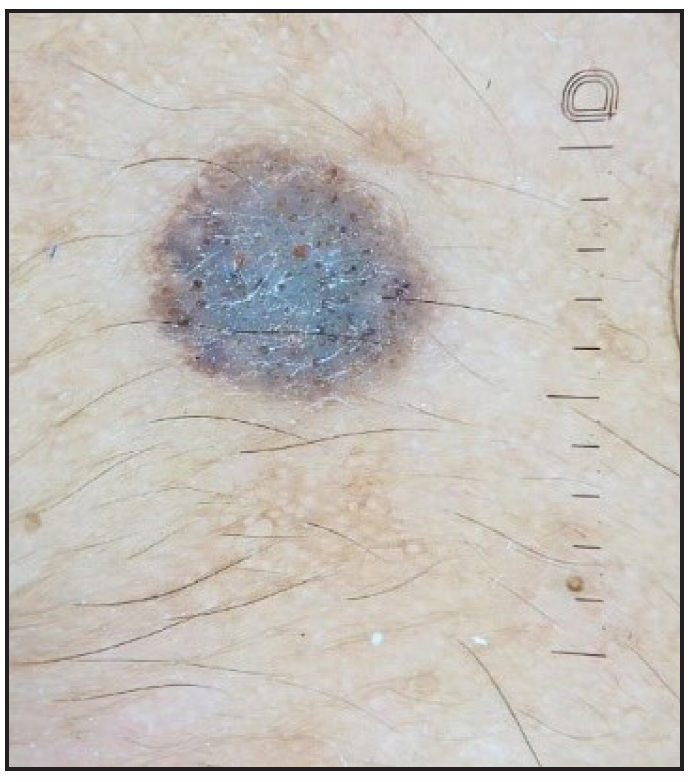
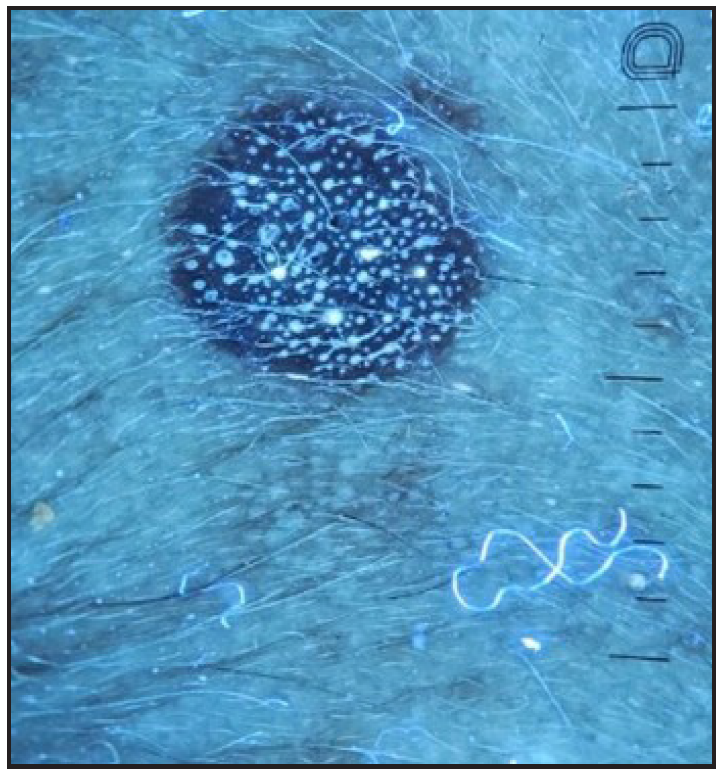
Molluscum contagiosum – central umbilicated area shows bright white fluorescence [Figures 3a and 3b].
–
Scaling tends to be generally more prominently seen under UV dermoscopy. For example, in pityriasis versicolor – the fines scales are visible more clearly using UVRD and can be enhanced by grattage test [Figures 4a and 4b].
–
The UV blink sign - The dermoscopic ‘blink sign’ describes the blinking appearance of certain dermoscopic patterns when the device is toggled between polarised and non-polarised modes. For example, the comedo-like openings in seborrheic keratosis are visualised more clearly on non-polarised dermoscopy, as compared to polarised dermoscopy, and hence these structures appear to blink when the dermoscope is toggled between polarised and non-polarised modes.9 The comedo-like openings and milia-like cysts seen in seborrheic keratosis tend to be clearer under UV and these structures show a blinking effect when the dermoscope is toggled between UV and non-UV modes. We would like to label this as the ‘dermoscopic UV blink sign’ (personal observation) [Figures 5a and 5b].
–
The pigmentary patterns in conditions like vitiligo tend to be generally clearer under UV dermoscopy [Figures 6a and 6b].
Export to PPT
Export to PPT
Export to PPT

Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
ConclusionThe combination of dermoscopy with UV light is a relatively recent introduction and can be useful in diagnostic dermatology. Most dermoscopes that incorporate UV light use a non-polarised form of UV light and hence it is basically like an examination under magnification using UV light. However, using a contact fluid along with the UV light mode will convert this into true UV dermoscopy
留言 (0)