
記住我
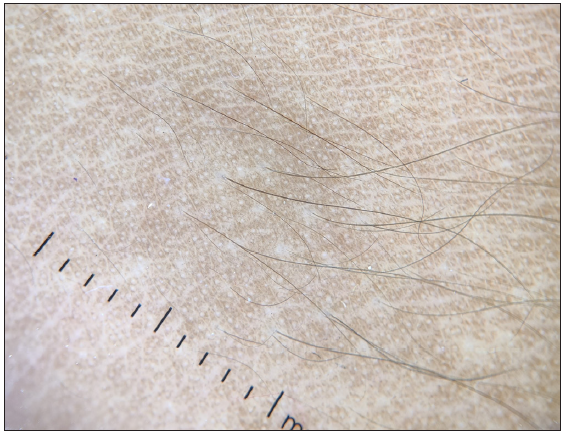
A thirteen-year-old girl, with a known case of ventricular septal defect, presented with a two-year duration of multiple skin-coloured to hyperpigmented nodules over her face, trunk and extremities. The lesions were asymptomatic, without any surface erosion or ulceration. On examination, multiple (eleven) firm-to-hard tender nodules of size ranging from 0.5 to 1.5 cm were present over the sites mentioned above. In addition, the skin-overlying nodules were pigmented and associated with hypertrichosis [Figures 1a and 1b]. The nodules on the face and thigh were bony hard, suggestive of calcification, which was later confirmed on X-ray evaluation of the skull and thigh [Figure 2]. Examination of the oral cavity showed a solitary, small, whitish, non-tender nodule on the left lateral aspect of the tongue [Figure 3]. There was no lymphadenopathy, and the rest of the mucocutaneous examination revealed no abnormality. Dermoscopy of the cutaneous nodules showed an increased pigment network with areas of perifollicular sparing [Figure 4]. An incisional biopsy was done from the nodule present over the left thigh for histopathological examination.

Export to PPT

Export to PPT

Export to PPT

Export to PPT
Export to PPT
Export to PPT
Export to PPT
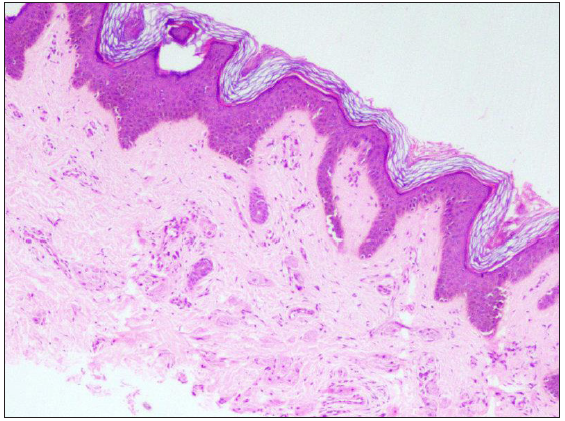
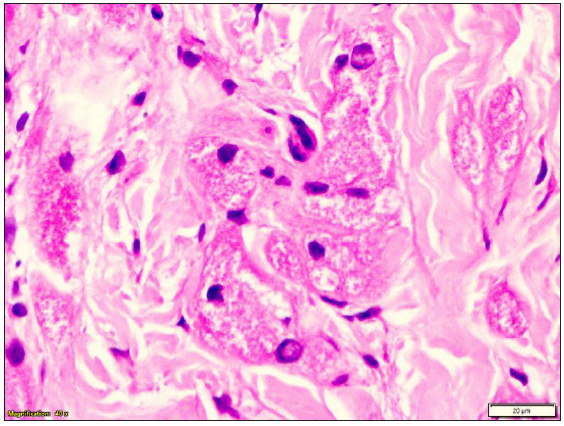
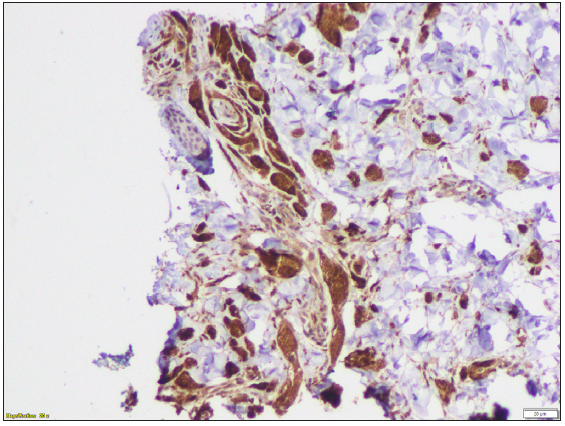
Histopathological ExaminationThe epidermis was unremarkable. In the dermis, scattered, large, round to polygonal cells with eosinophilic granular cytoplasm and central nuclei were present [Figures 4a and 4b]. The infiltrate was limited to the upper dermis without any subcutaneous tissue involvement. Immunohistochemistry was positive for CD68 [Figure 5] and S100 and negative for CD1a [Figure 4].
Export to PPT
QuestionWhat is your diagnosis?
AnswerDiagnosis: Hairy granular cell tumour
DiscussionGranular cell tumour (GCT) is a rare benign neoplasm originating from Schwann cells. There is a female preponderance and it commonly affects middle-aged individuals.1 The most accepted pathogenesis is the altered metabolism of Schwann cells, but origin from histiocytes, fibroblasts, or myoepithelial cells has also been postulated.2 It manifests as a solitary subcutaneous or submucosal nodule commonly involving the tongue or internal organs. Around one-fifth of the cases present with multiple lesions.2 Pointers towards diagnosing GCT in our case include multiple lesions, overlying hypertrichosis and mucosal lesions. The other differentials to be considered in lesions with overlying hypertrichosis include plexiform neurofibroma, leiomyoma, melanocytic nevus, smooth muscle hamartoma and eccrine angiomatous hamartoma. The nodules of leiomyoma and neurofibroma are firm in consistency and spare mucosa, while melanocytic nevus and smooth muscle hamartoma lack isolated nodules as in our case. Eccrine angiomatous hamartoma can have hyperhidrosis in addition to hypertrichosis and shows hyperplastic eccrine glands on histopathology. Moreover, hypertrichosis on cutaneous lesions of GCTs is extremely rare, with only one case reported.3 Increased stimulation of hair follicles and prolongation of the anagen growth cycle can be the possible mechanism. However, the exact mechanism needs to be established. Another interesting finding in our case was the calcification of the lesions over the face and thighs. Previous literature reported calcification in colonic tumours as well as seller Granular cell tumour (GCT).4,5 However, there are no reports of calcified cutaneous granular cell tumours to date.
This case highlights the importance of keeping GCT as a differential when one comes across hairy nodules on the skin, especially if mucosa is involved. Previous literature mentioned the association of GCT with Noonan syndrome, neurofibromatosis type 1 and LEOPARD syndrome.6 Our patient also had a ventricular septal defect without any other features of LEOPARD syndrome. The common origin of cardiac septum and schwann cells from neural crest cells might explain the association but needs further validation.7 Nevertheless, it is prudent to know about associated syndromes so that proper evaluation can be done, which can prevent major cardiac events in future. The GCTs are mostly benign and rarely show malignant behaviour.2 The prognosis was explained to the girl’s parents, and she is under regular follow-up.
留言 (0)