Problem
Margin-controlled, micrographic surgery is commonly indicated for the removal of several tumours including large basal cell carcinomas, squamous cell carcinomas and fibrohistiocytic tumours such as dermatofibrosarcoma protuberans. In these procedures, debulking is recommended to achieve flattening and an adequate evaluation of margins, commonly obtained with a 90° cutting angle. Thus, this practice requires several large incisions that may be technically challenging if homogeneous cuts are to be obtained for paraffin-embedded processing.
Solution
The use of a double scalpel with a 4-mm separation between the blades allows retrieval of 90° homogeneous surgical pieces, with an adequate thickness for processing and collection in pathology cassettes. This scalpel follows the same principle as the double scalpel with a 2-mm separation, already commercialised and routinely used in dentistry and in excision of lentigo maligna or extramammary Paget’s disease. The 4-mm double-blade scalpel can be customised by a surgical instrument manufacturer, based on this model. The risks associated with this scalpel do not differ from a conventional scalpel and its main limitation lies in the lack of experience with this instrument, its limited marketing, and the possible learning curve toward familiarisation with its use. This device is especially useful for the excision of lesions in which margins greater than 2 mm are the choice during paraffin-embedded margin-controlled micrographic surgery, such as large or high-risk basal cell carcinomas, and/or squamous cell carcinomas, Merkel cell carcinomas and/or dermatofibrosarcoma protuberans [Figures 1a–1g and 2a–2d, Video 1]1,2.

![]() Figure 1a:
Figure 1a:
A double scalpel with 4-mm separation.
Export to PPT

![]() Figure 1b:
Figure 1b:
Left submammary papulonodular lesion compatible with dermatofibrosarcoma protuberans.
Export to PPT

![]() Figure 1c:
Figure 1c:
Marking of the lesion.
Export to PPT

![]() Figure 1d:
Figure 1d:
Excision of the lateral margins with the 4-mm double-bladed scalpel.
Export to PPT
![]() Figure 1e:
Figure 1e:
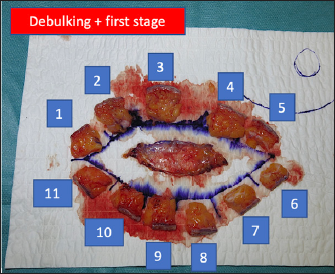
Histological representation of the first stage of Mohs surgery obtained with a double scalpel in a dermatofibrosarcoma protuberans of the trunk. Note that the debulking has been performed and that there are 12 histological pieces, one corresponding to the deep margin (thoracic deep fascia) and 11 to the lateral margins arranged in an orderly clockwise fashion. The pieces have an ideal size for their introduction into histological cassettes.
Export to PPT
![]() Figure 1f:
Figure 1f:
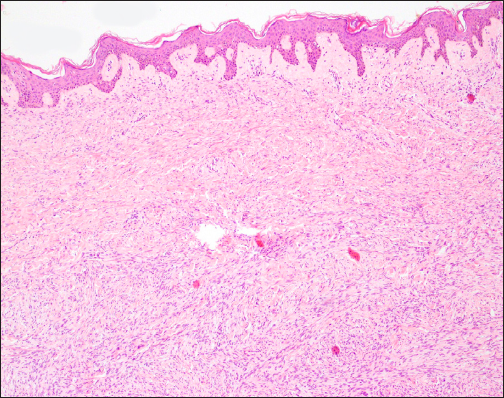
Histological sections of a dermatofibrosarcoma protuberans obtained by Mohs surgery with the double scalpel with 4-mm separation. The neoplasm was in the dermis and was composed of a dense proliferation of spindle cells, monomorphic, with a large and elongated nucleus, constituting irregularly intertwined fascicules, following a storiform pattern. The stroma is scant, with the presence of intercellular collagen deposits and small capillaries also stain (Haematoxylin and Eosin; 20x).
Export to PPT
![]() Figure 1g:
Figure 1g:
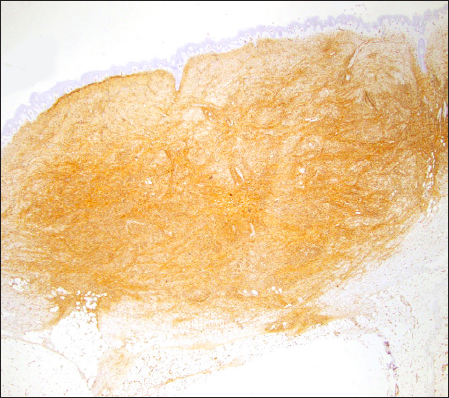
Histological sections of a dermatofibrosarcoma protuberans obtained by Mohs surgery with the double scalpel with 4-mm separation. The neoplasm was in the dermis and was composed of a dense proliferation of spindle cells, with large and elongated nuclei, arranged in irregularly intertwined fascicules, following a storiform pattern. The stroma is scant, with the presence of intercellular collagen deposits and small capillaries. CD34 staining is intensely positive (Haematoxylin and Eosin; 10x).
Export to PPT
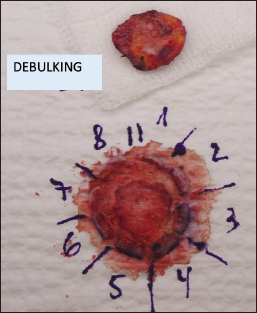
![]() Figure 2a:
Figure 2a:
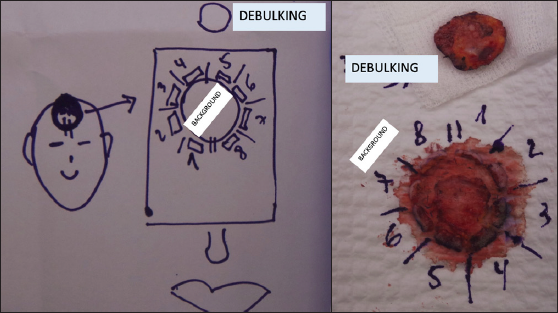
Excision specimen of high-risk basal cell carcinoma on the frontal scalp (debulking + fundus + lateral margins).
Export to PPT
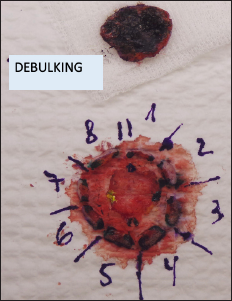
![]() Figure 2b:
Figure 2b:
Labelling of the excised margins.
Export to PPT
![]() Figure 2c:
Figure 2c:
Marking the margins with Indian ink for easier recognition.
Export to PPT
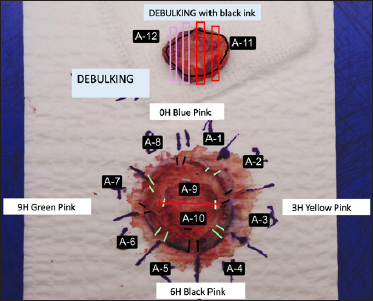
![]() Figure 2d:
Figure 2d:
Histopathological detail from the pathologist for analysis of all margins: marking according to their color code.
Export to PPT
Video 1: Demonstration of the use of a wide double scalpel on a patient with dermatofibrosarcoma protuberans on the anterior trunk.

留言 (0)