
記住我




Lower urinary tract symptoms (LUTS) impact over 50% of the global adult population [82]. These symptoms emcompass storage, voiding, and post-micturition symptoms. Notably, overactive bladder (OAB) syndrome is classified as a specific subset within the domain of storage symptoms [2]. According to the International Continence Society (ICS), OAB describes the symptom complex of urinary urgency, often accompanied by increased frequency and nocturia, with or without urgency urinary incontinence, occurring in the absence of urinary tract infection or other obvious pathological coditions [54]. OAB is reconginized as a highly prevalent, troublesome and distressing condition. Its incidence tends to rise with age and it exerts a remarkable impact on quality of life (QOL). OAB affects both male and female equally, resulting in a large economic burden on individuals and society, in terms of the direct health care costs and lost productivity.
Presently, clinical strategies for pharmacotherapy of OAB are still limited to antimuscarinics and β3 agonists. Due to associated risks and adverse effects of conventional medicines, the use of alternative therapies to treat diseases nowadays has witnessed a rapid increase. Compared to synthetic chemicals, phytochemical compounds from medicinal plants are usually less expensive, less toxic and present less side effects. Ethnopharmacology has been applying traditional medicine and natural products for disease management. For instance, some currently used drugs, like aspirin, artemisinin, and digoxin, are deprived from plant extracts. Some regimens and single-herb medications of Traditional Chinese Medicine (TCM) have exhibited efficacy in managing symptoms associated with OAB. Natural phytochemicals enable the maintenance of a biological balance and avoid drug accumulation in the body [12]. Additionally, a remarkable increase in the use of medicinal plants and natural products to treat OAB has been observed. [12, 34, 96]. Herein, we review and summarize the body of evidence, obtained through traditional application and modern scientific methodology, which supports the use of medicinal plants, natural products and herbal formulations for the treatment of OAB. The summary and consolidation of the existing scientific data would greatly facilitate improvement of future research and offer OAB patients a wider range of potentially improved alternative therapies.
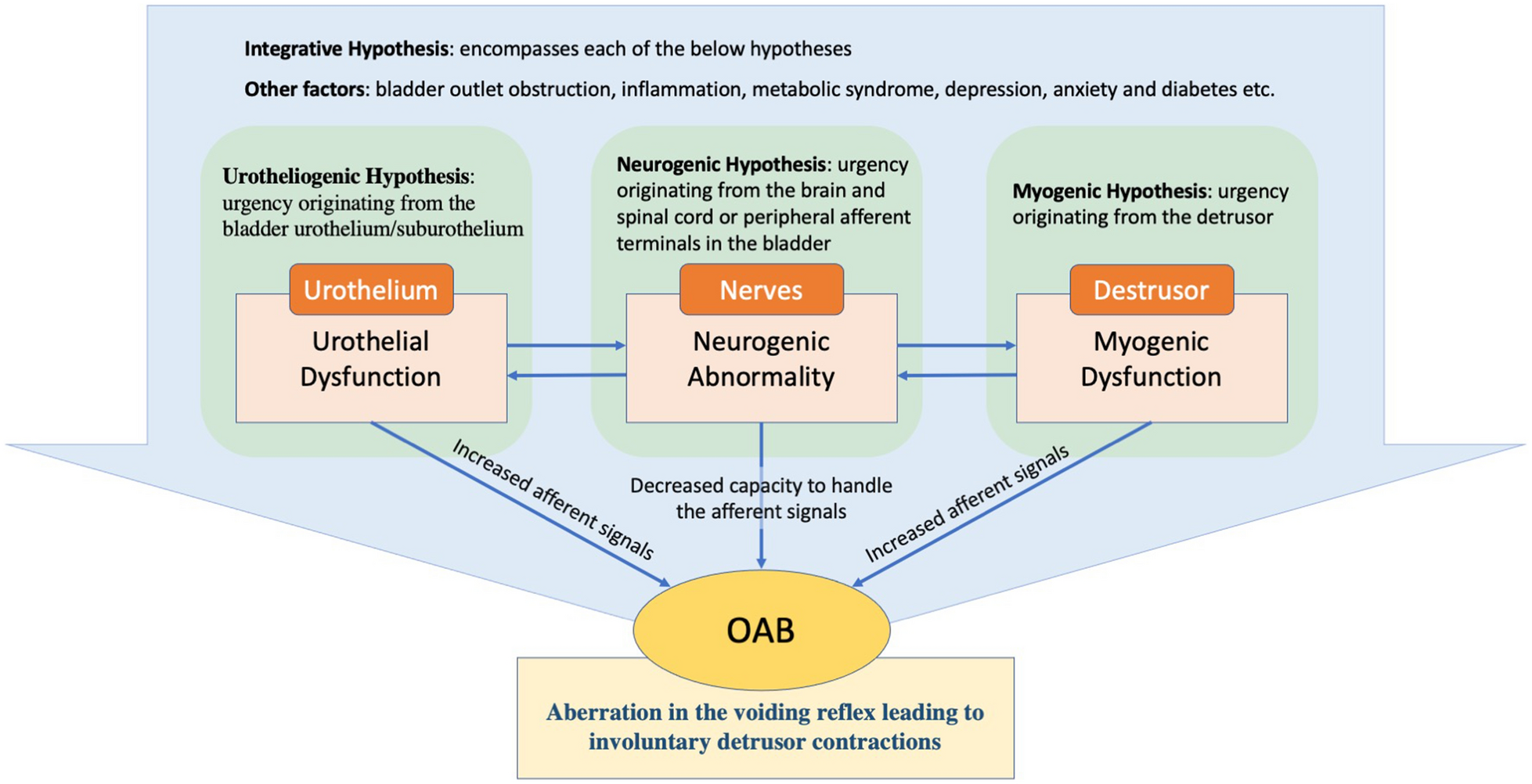
Pathophysiology of OABAt present, the etiology of OAB is largely considered idiopathic, and its underlying pathophysiology remains poorly comprehended, necessitating ongoing research endeavors. Two possible origins of OAB symptoms were proposed by the ICS: (1) reduced ability to process the afferent signals in the brain (the neurogenic hypothesis); and (2) abnormally enhanced afferent signals from the bladder and/or urethra: elevated afferent activity is considered to be associated either with aberration in the urothelium receptor function and neurotransmitter release (the urethrogenic hypothesis) or with aberration in myocyte excitability (the myogenic hypothesis) [123] (Fig. 1).
Fig. 1
Pathophysiology and underlying mechanisms of OAB
1.The urotheliogenic hypothesis
The urotheliogenic hypothesis refers to dysfunctions in signal molecules and ion channels within the urothelium. The urothelium not only acts as a protective barrier but also functions as a sensor to thermal, mechanical, and chemical stimuli. In the absence of a healthy urothelium, there may occur an elevation in spontaneous detrusor activity [107]. Through different receptors and transient receptor potential (TRP) channels, the urothelial cells respond to mechanical and chemical stimuli such as bradykinin, purines, norepinephrine, and acetylcholine (Ach), stimulating nearby afferent nerves. Abnormalities in the function of urothelium receptor and the release of neurotransmitter as well as in the sensitivity and coupling of the suburothelial interstitial result in involuntary contractions and manifestation of OAB symptoms [123, 166].
2.The myogenic hypothesis
The myogenic hypothesis posits that impaired function of the myocytes in the detrusor muscle may cause elevated excitability, hence leading to the occurrence of uncontrolled contractions [123]. Studies have demonstrated that myocytes obtained from the bladders of patients with detrusor overactivity (DO) display enhanced excitability and an amplified response to stimuli [23]. According to Drake et al. [37], it is hypothesized that DO could arise from histological alterations in the detrusor, resulting in abnormal electrical coupling of smooth muscle cells. Consequently, physiological micromotions get synchronised and transform into active involuntary contraction in the detrusor [59]. Bladder smooth muscle cells are interconnected through gap junction channels, predominantly composed of connexins, enabling their coupling. Although the involvement of connexins (Cxs) in the pathophysiology of OAB requires further study, Cx45 and Cx43 appear to be the most prominent Cxs expressed in human detrusor smooth muscle (DSM) cells [37, 111], and an increased Cx43 expression has been detected in individuals with neurogenic DO and urinary symptoms [8, 119].
3.The neurogenic hypothesis
The neurogenic hypothesis considers the abnormal management of afferent signals. In this case, urgency originates from the brain and spinal cord or peripheral afferent terminals in the bladder. Suprapontine lesions including cerebrovascular and neurodegenerative diseases like stroke and Parkinson’s disease, could cause aberrant central nervous system (CNS) activation and then lead to inappropriate excitation of the detrusor. Urinary retention occurs as a result of a spinal cord lesion, which eliminates voluntary and supraspinal control over the process of micturition [117, 123]. On the other hand, several specific neurotransmitters and related receptors participate in afferent signal transduction, such as muscarinic receptors and β3 adrenergic receptors. Among muscarinic receptors, M2 and M3 are the major subtypes expressed in the bladder [20]. Patients with idiopathic DO and painful bladder syndromes exhibit an elevated expression of M2 and M3 receptors in the bladder, and there is a notable correlation between the density of suburothelial M2 and M3 receptors and clinical urgency scores [109]. β3 adrenergic receptors is the dominant β-receptor subtype in the bladder [163], and expression of β3 adrenergic receptors in the bladder was strongly correlated with OAB-related symptoms [164].
4.The integrative hypothesis
The integrative hypothesis includes each of the above hypotheses since each of the components is likely to contribute to the pathophysiology of OAB considering the sophistication of mechanisms involved in micturition. Various potential triggers could induce local contractions (micromotions) in detrusor which are then transmitted to the bladder wall [35], resulting in occurrence of the sense of urgency. On the other hand, different other pathological and physiological conditions such as bladder outlet obstruction (BOO), inflammatory reactions, metabolic syndrome (such as diabetes), depression and anxiety also take part in the pathophysiology of OAB [106, 137]. Therefore, when patients present OAB symptoms, it is of utmost importance to conduct a comprehensive evaluation aimed at identifying and ruling out potential underlying causes.
Current treatments for OABVarious treatment options exist for OAB considering it involves multiple mechanisms. It is governed mainly by the severity of symptoms and the the extent to which it negatively affects patient’s quality of life (Table 1). General lifestyle changes have been suggested as a first-line therapy in all OAB patients; while pharmacotherapy or medications, including anticholinergics/antimuscarinics and β3 adrenergic agonists, are the mainstream treatment for OAB, based on their pharmacological efficacy both in theory and clinical application. They are regarded as second-line therapy for OAB. Third-line OAB therapy refers to neuromodulation of the nerves that control bladder function.
1.Lifestyle intervention, behavioral treatments and bladder training
Table 1 Therapy options for OAB [1, 94]The lifestyle intervention includes smoking termination, body weight reduction, timed voiding, modifying fluid intake, eliminating bladder irritants such as carbonated drinks and caffeine, adjusting bowel movements to avoid constipation and sprains during bowel movements and sleep [61, 101]. As for behavioral treatment, patients are trained to improve their ability to control and thereby disrupt or inhibit detrusor contraction. Pelvic floor muscle training (PFMT) could help inhibit pelvic floor contraction on the detrusor, therefore, ameliorating urgency and urge-related incontinence [99]. Bladder training is appled for cognitively and physically capable adults to further improve detrusor overactivity and regain continence by training them to gradually increase time interval between urinations [105, 121]. These practices mentioned must be accomplished daily with motivation and patience. If they fail to improve or control the symptoms, then pharmacotherapy or medications are added.
2.Anticholinergic or antimuscarinics drug
Drugs that inhibit acetylcholine-induced involuntary detrusor contractions are currently the mainstay treatment options for OAB. Anticholinergics were the first OAB pharmacotherapy on the market and present the largest available dataset [142]. It is widely recognised that normal bladder contraction in human is modulated primarily by stimulation or activation of muscarinic receptors within the detrusor muscle [17, 165]. The predominant cholinoceptors present in urinary bladder are M2 receptors, while its contraction is mainly mediated by the minor population of M3 receptors [165]. Therefore, M3-selective antimuscarinic agents (such as darifenacin and solifenacin) offer the first-line treatment for OAB, acting through competitively antagonizing acetylcholine at the M3 receptors in the DSM to inhibit DO [10]. However, regrettably, these M3-selective anti-muscarinic agents clinically result in various significant adverse reactiosns in many patients, including paralysis of accommodation, tachycardia, constipation, and dry mouth [11].
3.β3-adrenergic agonistic drug
During the urine storage stage in the bladder, norepinephrine (noradrenaline) is released by the sympathetic nerves and binds to the β3-adrenergic receptors on the DSM, exhibiting inhibitory action, which results in the bladder relaxation [43, 57]. Mirabegron is the only approved drug that acts as a effective and selective β3-adrenoceptor agonist. It is thought to relax the DSM by directly activating the β3 adrenergic receptors, which subsequently results in elevated cAMP and adenylyl cyclase levels in the tissue. In OAB rat models, mirabegron increases the average voiding volume in each urination, decreases the frequency of non-voiding contraction and enhances the bladder capacity without deranging discharge. Mirabegron could contribute to reduced annulled incidence; therefore, it can be applied in patients who discontinue previous anticholinergic/antimuscarinic therapy [14, 39, 124, 125, 141]. Common adverse effects of mirabegron include urinary tract infections, tachycardia, headache, and diarrhoea [150].
4.Neuromodulation and onabotulinum toxin A (Botox®) therapy
When patients fail first- and second-line OAB therapy, their conditions are regarded as refractory. Particularly, these patients show inadequate response to behavioral therapy. They also demonstrate either lack of response to medications (at least two types) or intolerance of medications (due to contraindications or adverse effects). Neuromodulation or onabotulinum toxin A (Botox®) therapy may be used for the carefully selected refractory patients. There are three different types of neuromodulation therapy, namely: peripheral tibial nerve stimulation (PTNS), sacral neuromodulation (SNS), and temporary chemodenervation of the bladder detrusor muscle. However, the treatment benefits are often counteracted by frequent and moderately severe adverse events such as lead migration, pain at the stimulator and lead sites, infection/irritation, electric shock, the requirement for additional surgeries, urinary tract infections (UTIs), dysuria, and hematuria etc. Onabotulinum toxin A (Botox®) therapy refers to injecting a chemodenervation agent, Botox® (Allergan, Inc., Irvine, CA, USA), into the bladder, which was approved by FDA for idiopathic OAB in 2013. Onabotulinum toxin A is originated from a bacterium Clostridium botulinum and it binds to peripheral cholinergic terminals at the presynaptic membrane of the neuromuscular junction to inhibit acetylcholine release. This action causes muscle fibers paralysis until new fibers grow, thus temporarily affecting the myocytes in the bladder wall [94, 130, 153].
The current treatments for OAB present various limitations or side effects in clinical use. Hence, there is a strong rationale for the exploration and development of novel treatment strategies that aim to optimize therapeutic efficacy against OAB while simultaneously minimizing adverse reactions and side effects associated with effective dosages. Medicinal plants play an important role in this aspect since they have a long tradition in LUTS treatment. The screening and mechanistic elucidation of herbal drugs will greatly value OAB therapy.
New drug targets for OAB treatmentIncreasing research suggests that the etiology of OAB is multifactorial, necessitating the continued exploration of new drug candidates. Several new drug targets and cellular pathways in the urinary bladder to treat OAB have been proposed recently, as follow: (1) Modulators of cyclic nucleotide (cyclic adenosine monophosphate and cyclic guanosine monophosphate) that mediate adenosine triphosphate (ATP) release from bladder wall tissues, such as P2X3 receptor antagonists and nitric oxide (NO)-sensitive soluble guanylyl cyclase (sGC) activator; (2) new targets for β3 agonists, including the bladder muscularis mucosa and bladder wall blood vessels; (3) Various TRP channels (TRPV1, TRPV4, TRPM8, TRPA1, and TRPM4) and the effects of their mediators (antagonists) on detrusor overactivity; (4) Large and small conductance Ca2+‐activated K+ channels (BK and SK channels, respectively) and their impacts on spontaneous contractions; (5) Antioxidants that function to inhibit oxidative stress pathways; (6) Antifibrosis agents that directly or indirectly modulate the TGF‐β pathway, namely the canonical fibrosis pathway [9, 47, 158].
Recent research shows that medicinal plants and herbs could provide more efficacious treatment options with less side-effects. And they have been found to act on different targets or pathways compared to synthetic drugs. Current scientific evidence has demonstrated that a fair number of medicinal plants and natural products with efficacy of treating OAB act via one or a few of the targets mentioned above. Effects and mechanisms of various medicinal plants on OAB treatment from existing studies are summarized in Tables 2 and 3.
Table 2 Single-herb medications for overactive bladder treatmentTable 3 Herbal formulations for overactive bladder treatmentMedicinal plants and natural products for OAB treatmentLiterature reviews show a significant amount of research addressing the potential application of medicinal plants and natural products in OAB treatment [12, 34, 96]. A wide variety of medicinal plants have been employed to treat OAB in various regions and countries throughout different historical periods. Clinical evidence as well as preclinical in vitro and in vivo investigation have demonstrated that medicinal plants and/or their active ingreidents are efficacious for alleviating OAB. Additionally, herbs or medicinal plants are usually combined into therapeutic formulas in accordance with the theories of traditional medicine. TCM practitioners believe in “synergistic” or “emergence” effect when using herbal formulations, which are considered more effective and comprehensive in the treatment of diseases than single herbs alone. In this section, single-herb medications and herbal formulations for OAB treatments are reviewed and summarized in Tables 2 and 3 respectively. And the illustration of their possible interverntion mechanisms in the unrinary bladder is shown in Fig. 2.
Fig. 2
Illustration of possible intervention mechanisms of medicinal plants and natural products on OAB in the urinary bladder. a Promotion of the NO synthesis and release. b Reduction of the ATP synthesis and release. c Inhibition of the expression of the M receptors. d Up-regulation of the expression of the adrenergic receptors. e Down-regulation of the expression of P2X receptors. f Inhibition of transmembrane Ca2+ influx and stimulation of Ca2+ release from intracellular stores. g Activation of K+ channels. h Inhibition of TRP channels. i Improvement in the barrier function of urothelium. j Regulation of excess blood flow. k Increase in intracellular cAMP in the bladder smooth muscles. l Inhibition of the release of inflammatory mediators, such as Substance P, CGRP etc.
Single-herb medications for OAB treatment Alpinia oxyphyllaAlpinia oxyphylla is known as “yì zhì (益智)” in Chinese. For centuries, the capsular fruit of this plant has been widely utilized in TCM to address specific symptoms of urinary incontinence, including frequency, urgency, and nocturia. Izalpinin, a flavonoid isolated from the fruit of Alpinia oxyphylla, was found to antagonized Carbachol-induced contractions concentration-dependently on rat bladder detrusor strips, which is due to its muscarinic receptor antagonistic action [168].
Artemisia monosperma (Wormwood)This plant thrives extensively in the Arabian desert and has been deemed as an antispasmodic and anthelmintic in traditional medicine. It is also applied to treat hypertension. An isolated flavanone from Artemisia monosperma, 7-O-Methyleriodictyol, inhibited the amplitude of the phasic contractions in a dose-dependent fashion, and lowered the tone of ileum, uterus, and urinary bladder in rats. It also relaxed the phenylephrine-precontracted pulmonary artery and the acetylcholine-precontracted trachea [3].
Artemisia vulgarisArtemisia vulgaris is widely distributed across natural habitats gloablly, spanning Asia, Europe, North and South America, as well as Africa [38]. It has been employed as a culinary spice in the food industry in different regions worldwide. For many centuries, A. Vulgaris has been utilized in traditional Chinese, Hindu, and European medicine to regulate the gastrointestinal system function and address a range of gynecological diseases [38]. In traditional system of medicine, this herb is considered a beneficial therapeutic agent in alleviating smooth muscle spasms [68]. In a recent research, it was found that A. Vulgaris extract inhibited carbachol-induced urinary bladder contractions via dual, anticholinergic and Ca2+ antagonist mechanisms, by blocking muscarinic receptors and influx of extracellular calcium [78]. This indicates its potential for treatment of bladder overactivity.
Aspalathus linaerisAspalathus linearis, commonly know as Rooibos (meaning “red bush”) is a leguminous shrub indigenous to the Cape Floristic Region of South Africa [7]. The species complex composes of several different growth forms, and among them the Red type has been cultivated for producing rooibos herbal tea. In the last decades, A. linaeris has become very popular for its antioxidant and medicinal attributes [122]. In traditional medicines, A. linaeris is generally accepted as a helpful therapeutic in relieving smooth muscle spasms [68]. In a study with rabbit urinary bladder strips, A. linaeris extract relaxed the bladder and inhibited carbachol-induced urinary bladder contractions via a dominant opening of ATP-sensitive potassium-channels and a weak blockade of calcium channels [78]. This reveals its medicinal usefulness in hyperactive bladder disorders.
Astragalus membranaceus (Huangqi)Astragalus membranaceus, also called huáng qí (黄芪), it is an herb widely used in TCM and diet, and it has been widely studied in western medicine for various disease treatment. Astragalus polysaccharide (APS) is a type of water-soluble heteropolysaccharide deprived from the stems or dried roots of Huangqi [174]. Astragaloside IV (AS-IV), a small molecular saponin, is another major component from the aqueous extract of Astragalus membranaceus [170]. An in vivo study reported that both APS and AS-IV ameliorated urinary frequency on a CYP-induced OAB female mice model via modulation of urothelial wound healing, possibly via the increased expression of tight junction protein ZO-2 [32].
Bletilla striataBletilla striata is distributed widely in eastern Asian countries, including China, Japan, North Korea, and Myanmar. As widely used in TCM for thousands of years, its functions of hemostasis, detumescence, and improving one’s health have been recorded in Chinese Pharmacopeia (2015) [69]. Besides having been employed to treat hemoptysis, traumatic bleeding, chapped skin, swelling, and ulcer bleeding [157], it has also been used in TCM empirically to treat interstitial cystitis (IC). Study on zymosan‐induced cystitis in female rats [97] showed that treatment of B. striata extract solution decreased abdominal withdrawal reflex (AWR) scores and amplitude of bladder detrusor electromyogram (EMG). Furthermore, it demonstrated notable improvements in OAB by effectively prolonging the micturition interval and enhancing urine storage capacity. These results implied the possible efficacy of B. striata on treating OAB. However, more research on OAB models and patients is required for further validation.
Bridelia ferrugineaThis tropical plant is native to Africa and has been utilized in African traditional medicine to treat intestinal and bladder ailments. Ethanolic extract of B. ferruginea leaves inhibited KCl-induced contractile response in rat urinary bladder smooth muscle. This effect might be ascribed to the blockade of purinergic neurotransmission [116]. It can be speculated that B. ferruginea leaf exact could be useful in bladder overactivity although further research is required to better evaluate its potential therapeutic application.
Bryophyllum pinnatumBryophyllum pinnatum is a succulent perennial plant originating in Madagascar, whose leaf press juice was shown to reduce the electrical- or carbachol-induced contractile response in porcine DSM [129]. The flavonoid fraction of this plant lowered the porcine detrusor contractility in dose- and time-dependent fashion [
留言 (0)