
記住我
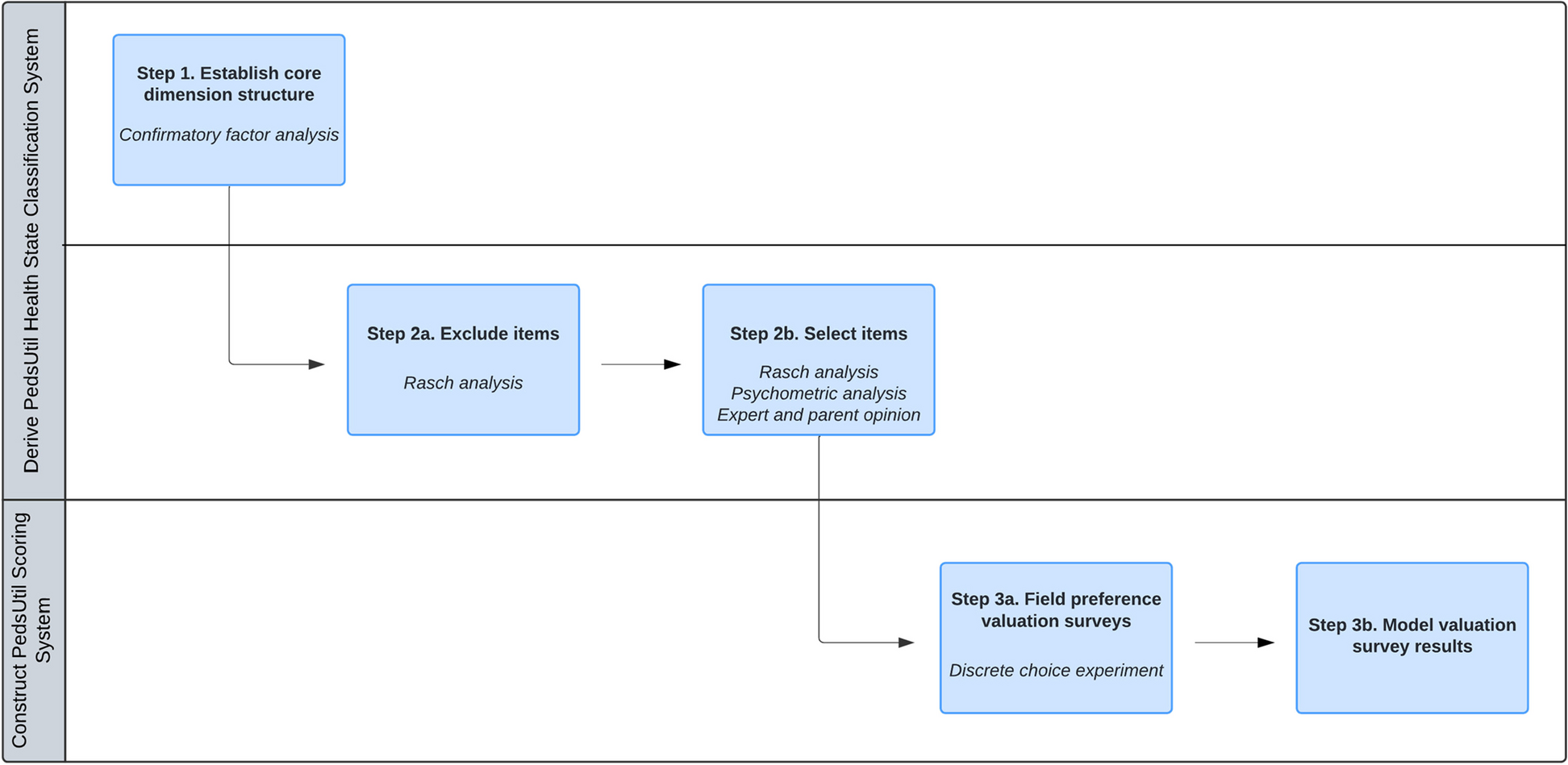
This study was conducted in three steps: 1) literature search on validated instruments using open-ended questions in cancer patients, 2) translations of WISP following the EORTC Quality of Life Group (QLG) Translation Procedure [12] and 3) pre-testing the translated WISP alongside the EORTC questionnaires and expanding the qualitative part with structured patient interviews to identify potential comprehension problems, following the EORTC QLG Module Development Guidelines (Phase 3.a) [13]. These steps are described in further detail below.
Literature searchWe performed a literature search on validated instruments with open-ended questions for cancer populations since 1990. The following keywords were searched in PubMed and CINAHL in March–April 2020: (("Patient-reported outcomes" OR "Patient-reported outcome measurements" [MeSH] OR "EORTC-QLQ" OR "systematic assessment") AND (open-ended)) AND ("Terminally ill" [MeSH] OR "advanced cancer" OR "Neoplasms" [MeSH])). When instruments were identified, we contacted the corresponding authors to ask about their experience collecting data with open-ended questions and which coding system they used.
We also contacted all EORTC QLG members asking whether they had knowledge of instruments including open-ended questions used in cancer patients and/or experience performing data analysis for these instruments.
Study populationFor the pre-testing of WISP, we planned to recruit cancer patients from at least 6 countries (at least one English-speaking country and one non-European language country) to assess the WISP instrument in a cross-cultural context [13]. In each included country, we planned to recruit 20 patients receiving diverse cancer treatments; 10 patients should be from an oncology setting (5 patients receiving chemotherapy/radiotherapy and 5 receiving immune/targeted treatment in hospital departments), and 10 patients from a palliative care setting (i.e., receiving palliative care/treatment in a palliative care service, hospice or hospital department).
Inclusion criteria were: 1) having knowledge of the cancer diagnosis, 2) being at least 18 years old, 3) undergoing active antineoplastic treatment or palliative care/treatment, 4) being a native speaker of the country's language, 5) being mentally and physically able to participate, and 6) providing informed consent.
TranslationThe EORTC QLG Translation Unit made forward/backward translations of the original WISP in Danish into English (Fig. 1) and seven additional languages for cultural adaptation. These translated versions of WISP were pilot-tested in each country by asking five cancer patients in active or palliative treatment to review the wording of the instrument and discuss whether the translated version was difficult to answer, confusing or upsetting [12].
Fig. 1
English version of the WISP instrument
Procedure for the pre-testing of WISP and patient interviewsFrom November 2022 to June 2023, we pre-tested WISP together with the selected EORTC questionnaires. Patients in active treatment completed the QLQ-C30 + a relevant module according to the patient’s diagnosis if available + WISP, whereas patients in palliative care/treatment completed the QLQ-C15-PAL + WISP.
After patients completed the questionnaires and reported at least 1 symptom/problem using WISP, they were invited to participate in semi-structured interviews to collect information on their understanding and acceptability of WISP, as well as the usefulness of WISP for their reporting of ‘additional symptoms/problems not included in the questionnaire they just completed’ [13]. The interviews were conducted in person by local researchers in the patients' native language, were summarized by the local researcher and not audiotaped, and lasted approximately 15–20 min.
QuestionnairesThe QLQ-C30 comprises 30 items distributed in five functional scales (physical, emotional, role, cognitive and social functioning); three symptom scales (fatigue, pain, nausea/vomiting); two global scales (global health and quality of life) and six single items (insomnia, dyspnea, constipation, lack of appetite, financial difficulties and diarrhea) [4]. The QLQ-C15-PAL consists of half of the items of the QLQ-C30 containing only those items that are most relevant for patients in palliative care [5]. In both EORTC questionnaires (+ module), items are rated on 4-point Likert scales that range from 1 (not at all), 2 (a little), 3 (quite a bit) to 4 (very much), except for global health/quality of life scales rated from 1 (very poor) to 7 (excellent) [4, 5].
WISP consists of a single item asking patients to report up to three symptoms/problems not mentioned in the questionnaire preceding it (i.e., QLQ-C15-PAL or QLQ-C30 + module). Responses on WISP use the same 4-point rating scale as the EORTC questionnaires [11]. This study only reports data collected on WISP.
Statistical analysesPatient characteristics were expressed as proportions and compared between patients in active and palliative care/treatment using Chi-square tests (significance level of 0.05).
Qualitative responses from patient interviews were categorized and summarized according to patient treatments. We calculated the proportion of patients adding information about their symptoms/problems and the proportion of patients rating WISP as difficult, annoying, confusing or upsetting to answer.
WISP responses that were rated at least as 2 (a little) were coded using a coding system of 61 symptom/problem categories developed in Denmark to analyze WISP data reported by patients in specialized palliative care [11, 14, 15]. This coding system was developed by grouping the WISP qualitative responses into categories; for example, ‘back pain’ was coded as ‘pain’. If a symptom/problem was not covered by the QLQ-C15-PAL, new codes were established using a list of 48 physical and psychological symptoms developed by Homsi et al., which investigated symptoms reported by palliative patients using open-ended questions versus those systematically assessed [16]. We created extra codes if a symptom/problem did not match any existing category [11]. The prevalence of symptoms/problems reported on WISP was calculated for all cancer patients and for patients receiving different types of treatment (active treatment vs. palliative care/treatment). We calculated the severity as the proportion of symptoms/problems rated as ‘a little’ (mild), ‘quite a bit’ (moderate) and ‘very much’ (severe). Statistical analyses were conducted using the IBM SPSS Statistics 28.
留言 (0)