Our study in a large real-world cohort of US adults of diverse backgrounds shows that across all ASCVD risk groups, sexes, and ethnic groups, there remains significant underutilization of SGLT2-is and GLP-1 RAs. While use of these therapies was higher in those with DM who had multiple risk factors or ASCVD compared to those without multiple risk factors, even in those with both DM and ASCVD, only 8.6% were on an SGLT2-i and 11.9% on a GLP-1 RA. Although the use of SGLT2-i or GLP-1 RA was slightly greater in Hispanic or Latino people than in non-Hispanic White persons, barely one-tenth of all ethnic groups with DM are on these newer therapies. Those without health insurance or with lower levels of educational attainment were also least likely to be on these therapies.
A recent study focusing on persons with health insurance found similar results to our study with low use of SGLT2-i and GLP1-RA among patients with DM [19]. Similarly, among those with DM in the National Health and Nutrition Examination Survey 2017–2018, only 4.5% were on SGLT2-i and 1.5% were on GLP-1 RA [20]. Specifically, in those with ASCVD and type 2 DM, others found < 12% to be on these newer DM medications [21]. The results from our study as well as others are concerning as CVD outcomes are higher among those on sulfonylureas or insulin compared to those on GLP-1 RAs, SGLT2-is, and DPP-4 inhibitors [22].
Data from the Diabetes Collaborative Registry (2013–2016) showed that metformin, sulfonylureas, and insulin were used more by patients with type 2 diabetes compared to SGLT2-is and GLP-1 RAs, which were used by only 4.2% and 5.5% respectively by DM patients in the registry [23]. Among these patients without heart failure, only 4.2% and 5.5% were on SGLT2-i and GLP-1 RA, respectively [23]. Furthermore, only 2.7% and 4.3% were on SGLT2-i and GLP-1 RA, respectively among patients with both type 2 DM and heart failure [23], showing clear underutilization of these newer therapies. While there are some slight increases in the proportion of type 2 DM patients with CVD taking SGLT2-i and GLP-1 RA since the publications of EMPA-REG OUTCOME and LEADER, use of these medications is still quite limited [24]. From 2015 to 2018, patients with type 2 DM and CVD from the Optum Claims Database show an increase from 4.1 to 7.2% on SGLT2-i and 4.2 to 8.2% on GLP-1 RA [24].
Clinical inertia remains an important reason for the underutilization of these therapies. This includes cardiologists’ skepticism about prescribing diabetes medications; some feel these are out of their scope of practice [18]. Furthermore, without proper knowledge on these therapies, there is hesitancy about prescribing them [18]. Finally, there is a lack of implementation of automated systems approaches, such as electronic medical record reminders and best practice advisories that can be helpful to ensure their appropriate utilization.
Our data underscore the need to better disseminate and implement recent guidelines that focus on the use of these therapies for those with DM at highest risk of CVD [2]. While the highest use of therapies was in those with DM and ASCVD, use was still seriously inadequate with < 15% of such persons on these therapies. There is often a lag of more than 5 years between recommendation of newer medications and even modest adoption of their use [25]. The guidelines to use the newer medications are only a few years old, so our results are not surprising. The value of SGLT2-i therapies in reducing CVD outcomes has been reported with empagliflozin and canagliflozin among those with both DM at high CVD risk [26, 27], and dapagliflozin in mostly primary prevention DM for reducing cardiovascular death or hospitalization due to heart failure [9]. Similarly, the value of GLP-1 RA therapies in reducing adverse outcomes has been shown with liraglutide in those with DM with and without CVD [28], as well as subcutaneously administered semaglutide [12], but not oral semaglutide [29]. However, not all SGLT2-is and GLP-1 RAs have research and trial data to back their use in reducing occurrence of ASCVD.
While SGLT2-i use was somewhat higher in our participants with HF who were males, Hispanic or Latino persons, use was still suboptimal with use at only 6–10% for most groups. Those with CKD had even less usage of SGLT2-is, with no significant difference in usage across all different categories. This could be explained by in part by older persons being less likely to initiate SGLT2-i or GLP-1 RA treatment, despite the high prevalence of CKD in this population [30]. Older patients are more likely to have other health contraindications for starting these therapies and could be skeptical of newer treatments. Since the greatest concentration of those with CKD and diabetes are in this population, the under use of SGLT2-i in our data could be related to this discrepancy.
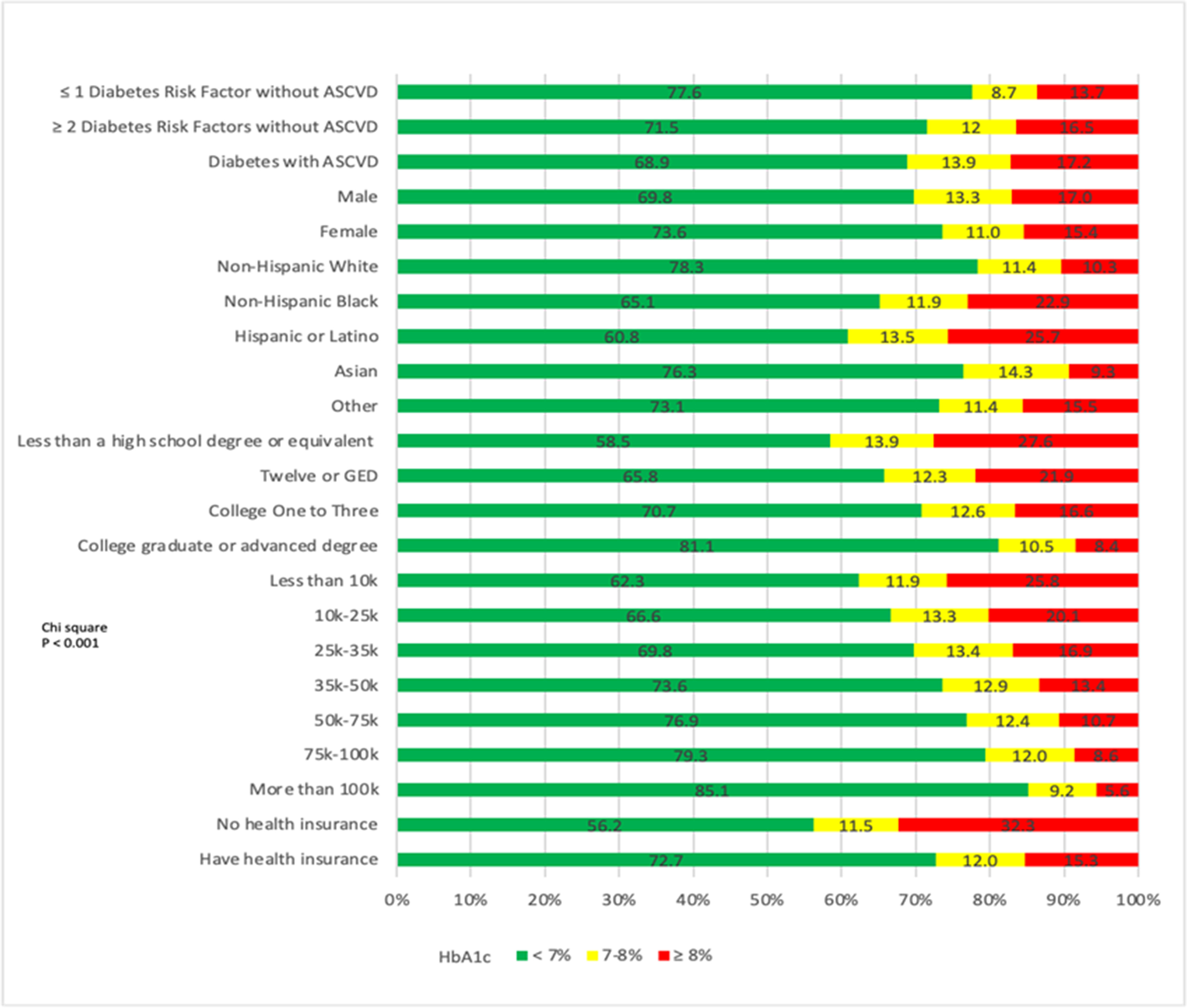
We identified HbA1c control remains suboptimal, especially among those with DM and CVD who are a highest risk. Since around 70% of our participants were controlled according to HbA1c, it was not surprising that the use of SGLT2-i and GLP-1 RA was low. Hispanic or Latino persons as well as Asian persons had the highest proportions not in glycemic control. Previous research has shown that both Hispanic or Latino persons and Asian persons have higher HbA1c levels compared to White persons [31], and there are multiple explanations for the continued elevated HbA1c levels among these ethnic groups. One explanation is that there is a lack of culturally tailored diabetes prevention program for specific ethnic groups, which needs to address ethnic-specific dietary and physical habits, as well as risk factors that are most predominant among specific groups [32]. Similarly, a systemic lack of diabetes support resources, guidance, and mental health well-being plays a role in the poor glycemic control in the Hispanic or Latino population [33]. Not surprisingly, we noted those of higher income to be more likely on GLP-1 RAs, consistent with the notion that those who can afford newer therapies will be on them [34]. Furthermore, given the extreme expense of these medications, our results are not too surprising [35]. These agents are often held in reserve for later use when traditional medications are ineffective. We also show that the highest risk group of diabetes with ASCVD are also more likely to be on both therapies, following the trend expected after the recent guidelines on medications for at high-risk groups [2]. Finally, our observations showing a lack of greater uptake of these therapies nor improved glycemic control over time underscores the continued disparities in diabetes treatment among our cohort with a high representation of underserved, lower education, and lower income participants.
We show that those on health insurance are more likely to be on both SGLT2-i and GLP-1 RA. Research has shown that patients with commercial health insurance plans are more likely to be on these newer diabetes therapy, specifically SGLT2-is [36]. Similarly, those with private health insurance plans are more likely initiate treatment on GLP-1 RA [37]. However, the mere presence of health insurance may be insufficient; Medicare Advantage health insurance plans may only partly cover the costs of these medications, resulting in significant out-of-pocket costs [38]. Furthermore, patients without health insurance are least likely to have access to these therapies. Financial barriers to obtaining many beneficial medications remain an important cause of adverse health outcomes globally.
Interestingly, in adjusted analyses, we found that Asian, Black, and Hispanic/Latino participants have greater odds of being on SGLT2-is and Black and Hispanic/Latino participants have greater odds of being on GLP1-RAs than White participants, although use in all groups remained low. Further studies on ethnic/racial medication preferences as well as responses to new therapies are needed. Similarly, we noted that males were more likely to be on SGLT2-i, but not on GLP-1 RA. Females were not prescribed SGLT2-is as often as males, suggesting that gender inequality influences therapeutic plans, which ultimately results in detrimental outcomes and is reflected in our results [34]. Additionally, the mechanism of action of SGLT2-is involves increases in renal glucosuria, which creates a favorable environment for pathogens to proliferate, leading to genital infections. There has been a higher incidence of genital infections after initiating SGLT2-is in female patients [39], which could explain the sex differences in SGLT2-i use in our study.
Inequalities in use of these medications also have to do with underserved populations not having adequate access to these therapies. Special programs are needed by payers and manufacturers of these drugs to make these more available to underserved populations with low utilization. Since a major challenge is getting these newer therapies to underserved populations, some of the ways this can be accomplished is through studying the social determinants of health in individual communities, incorporating virtual care, and shifting budgets to outpatient/primary-care settings [40]. Furthermore, focusing on value-based care and evidence-based medicine, along with a single-payer model and a public choice model, can be utilized to reach universal coverage [41].
Our study has several strengths and limitations. Our study is unique in that the participants reflect the diversity of the USA, including significant representation of people who have not taken part in or have been left out of health research before, including persons representative of the diversity of the USA from all backgrounds and regions. The detailed linkage to medical records allows assessment of SGLT2-i and GLP-1 RA use and glycemic control across groups stratified by ASCVD risk as well as social determinants of health. A limitation is the cross-sectional nature of our study without multiple measures to assess adherence, nor follow-up to examine cardiovascular or mortality outcomes. Furthermore, since our sample size is large, small differences reach the threshold of statistical significance.
In summary, our study has shown in a diverse cohort of US adults that despite recent guidelines for SGLT2-is or GLP-1 RAs use in higher risk people with DM, few are actually taking them, and use is lower among the underserved. Several large clinical trials over the last decade have demonstrated greater benefit in using new glucose lowering therapies than those previously recommended for standard care. We would expect these results to lead to increased uptake over time of said newer treatments, but data relating to use of these agents in a real-world setting are limited. Our study emphasizes the need to further examine barriers towards implementation of these newer therapies, especially among those lacking sufficient health insurance who are often at highest risk of CVD and other DM-related outcomes. Automated systems aimed to improve use of these and other evidence-based therapies in appropriate patient populations are crucial to optimize quality of healthcare.


留言 (0)