
記住我




Sixteen neonates diagnosed with PAIS were included, 9 males and 7 females. Thirteen were born from singleton pregnancies. Of the three twin pregnancies, only one was spontaneous, the other two pregnancies following oocyte donation, or in vitro fertilization (IVF). Gestational age ranged between 31 + 2 gestational weeks (GW) and 41 + 5 GW, with 2 early preterm births, 5 preterm births, and 9 full-term deliveries. The majority of neonates (12/16) developed neurological symptoms between days 1 and 3 of life; the remaining 4 newborns were diagnosed following brain ultrasound routinely performed in the setting of prematurity.
The clinical characteristics of the PAIS cases and of the controls can be found in supplemental Table S1.
Placenta histopathological findings, neonates with PAISThe histopathological features of the 16 placentas are summarized in Table 1. Slightly more than half the placentas (9/16, 56%) showed features belonging to more than one category. Representative examples from the 3 categories of lesions are illustrated in Fig. 1.
Table 1 Main histological findings, placentas from neonates diagnosed with PAISFig. 1
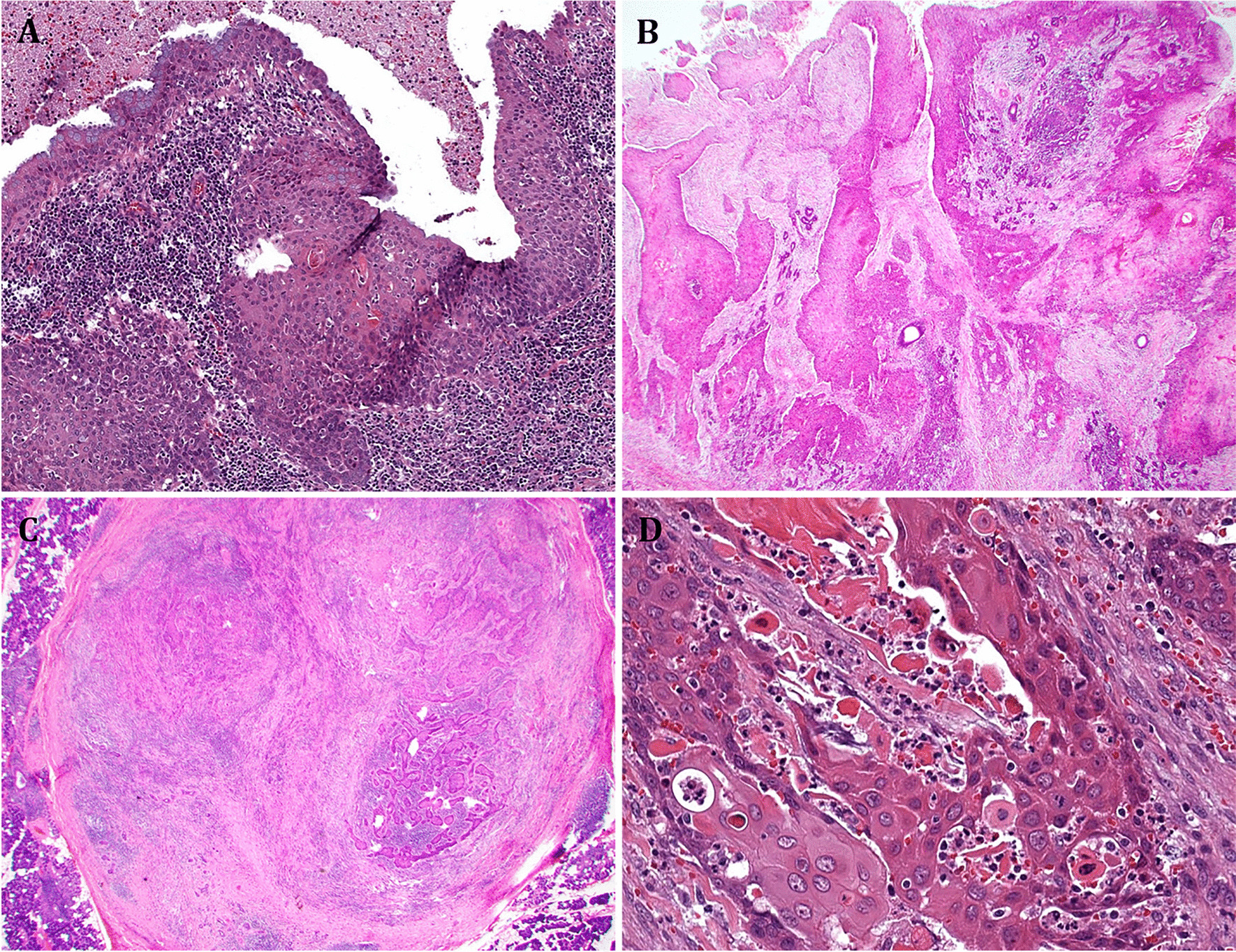
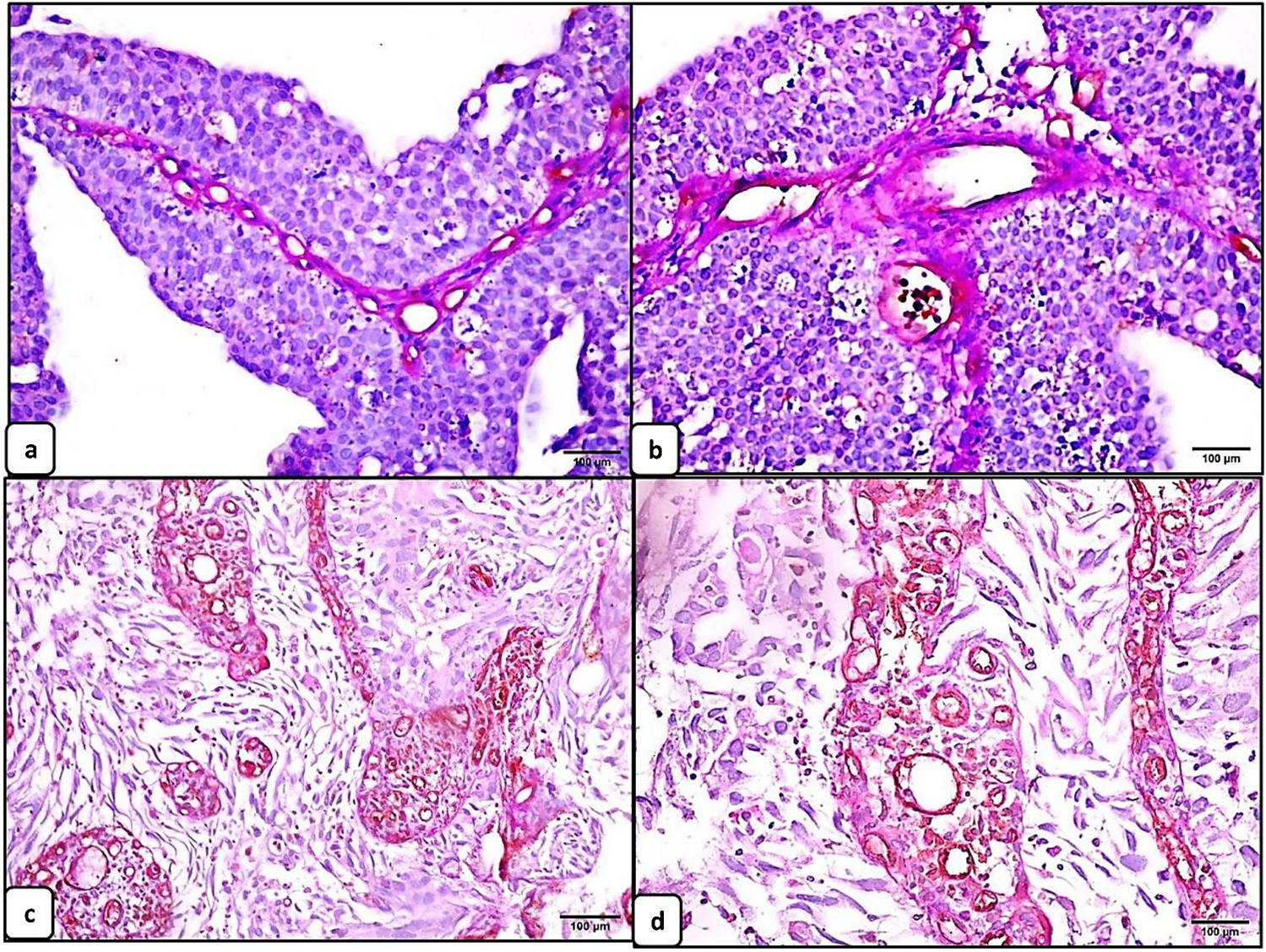
Illustrative gross and microscopic placenta pathological findings of the main categories of lesions. Associated brain MRI findings are shown. Case P2: inflammation. Ascending intrauterine infection, premature delivery at 33 + 6 GW. A, B Umbilical cord phlebitis (V, umbilical vein) and arteritis (A, umbilical arteries) identify a stage 2, grade 2 fetal inflammatory response (hematoxylin & eosin, H&E, A × 10, B × 60). C Left posterior MCA old infarct seen on axial T1 MRI at day 15. Case P6: hypoxia and high BW/PW. PW < P10, BWP50–P75, and term delivery. D, E On cut section, 20% of the placenta approximately showed large firm whitish areas (D), corresponding histologically to maternal vascular malperfusion (MVM) and large areas of infarction (E, H&E whole-mount view). Areas of villous stromal hemorrhage were consistent with acute hypoxia (F, H&E × 400). G Imaging findings at day 1 demonstrate on DWI massive acute left hemispheric stroke and right MCA stroke. Case P14: hypoxia. Diamniotic-dichorionic twin pregnancy, early premature delivery at 31 + 2 GW. H FVM was seen in the affected twin only. Villous stromal-vascular karyorrhexis, with iron deposition (arrow), and stem vessel obliteration (arrowhead) are shown. I, J Imaging findings (coronal T2 and axial T1) at term demonstrate bilateral porencephalic cavities in the MCA territories, more extensive on the left side
Category 1: inflammationEvidence of ascending intrauterine infection was seen in 5 singleton placentas (5/16, 31%), one preterm, the other full term, that also displayed histological signs of hypoxia (Category 2 lesions). Two cases showed a S2, G2 fetal inflammatory response, i.e., severe acute umbilical phlebitis and arteritis were seen. The other three placentas showed acute non-severe S1, G1 umbilical phlebitis. One case also displayed high-grade, diffuse VUE.
VUE was seen in two twin placentas.
Category 2: placental and fetal hypoxic lesionsFeatures consistent with placental and fetal hypoxia were the most frequent findings, (15/16, 94%), consisting mainly of FVM and MVM.
FVM, identified in 7 placentas (7/16, 44%), was high grade in 4 cases, low grade in 2 placentas, and ungradable in the last (Case P8) due to freezing artifacts. The intensity of the lesions was therefore variable, ranging from recent intramural fibrin deposition in stem vessels, to high grade FVM with multiple chorionic plate and stem vessel thromboses, villous stromal-vascular karyorrhexis, and large areas of avascular villi. In one placenta (P12), focal vessel wall calcification was seen, together with umbilical vein, chorionic plate vessel, and stem vessel thrombi. High grade FVM was associated in two cases with signs of an acute hypoxic event to the placenta [16] (villous stromal hemorrhage) and with meconium-laden macrophages in the membranes or increased NRBCs and EVT in one case each. Meconium-laden macrophages in the membrane chorion have been associated with an increased likelihood of oropharyngeal meconium and increased risk of meconium aspiration [17]. Of note, FVM may have been overlooked in the sole placenta without histological evidence for hypoxia (P9), since evaluation was limited by freezing artifacts, the placenta having been sent with delay to the pathology ward. In 4 of the 7 cases with FVM, features of MVM were associated.
MVM without FVM was seen in 6 further cases. Two cases showed associated signs of acute or prolonged chronic hypoxia. Meconium staining of the membranes was also seen.
There is no consensus on the definition of high grade MVM. Provisional criteria consist of a placental weight < 3rd centile with at least one of the following: accelerated villous maturation, distal villous hyperplasia, and multiple infarcts [18]. One preterm singleton placenta (P5) met these criteria.
The one case of SARS-CoV-2-related MPFD showed extensive parenchymal damage, involving more than 80% of the placenta volume, expected to result in fetal hypoxia (P1, Fig. 2). There was no evidence of coexisting chronic histiocytic intervillositis.
Fig. 2
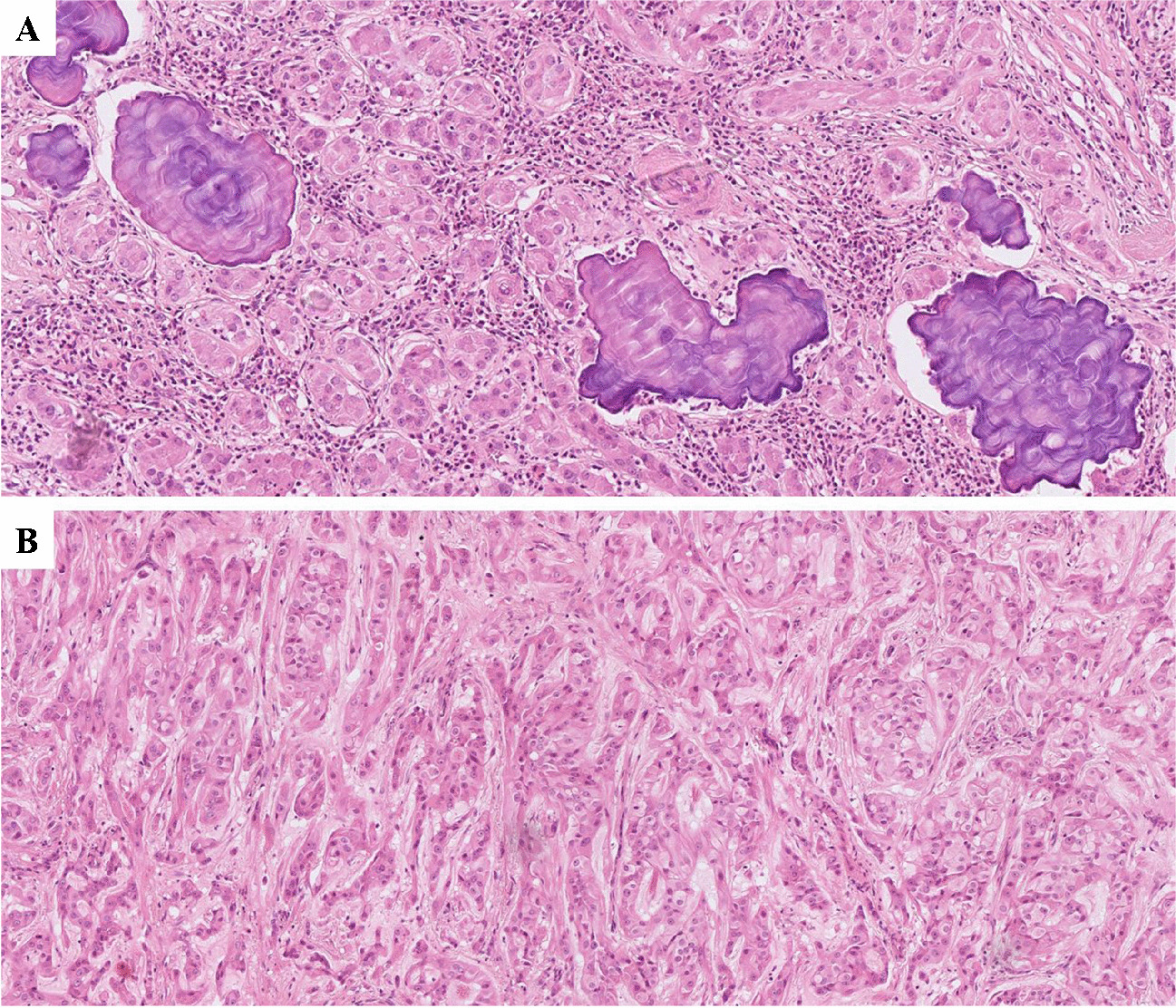
Case P1: SARS-CoV-2 infection. A Macroscopic placenta section, early preterm delivery (31 + 4 GW), showing extensive fibrin deposition, involving > 80% of the total placenta volume. B Histology showed partially necrotic chorionic villi encased in fibrin (hematoxylin & eosin, H&E, × 100). C Circumferential cytotrophoblastic and syncytiotrophoblastic reactivity to SARS-CoV-2 nucleocapsid antibody (× 100). D Imaging at day 3 shows acute left MCA infarct on DWI
Finally, excessive EVT and increased syncytial knots consistent with chronic hypoxia, and patchy villous edema were documented in a placenta from a polydrug user (P4, Fig. 3), with prenatal exposure of the neonate.
Fig. 3
Case P4: in utero crack cocaine exposure. A Increased extravillous trophoblast with atypia is seen (arrowheads), together with focal villous edema (arrows). B DWI MRI at day 5 demonstrates acute superficial left posterior MCA stroke
Category 3: placentas with a high BW/PW ratioFive placentas, one twin and four singleton, were considered small relative to neonatal birthweight. Except for the one placenta with freezing artifact discussed above (P9), all showed features of hypoxia (Category 2), and three also displayed inflammation (Category 3).
Comparison with controlsTerm pathological placentas vs. normal term controls from the membrane donation programSimilar to the PAIS placentas, lesions of more than one category were seen in a majority of the control cases (13/20, 65%).
All 20 control placentas showed some degree of hypoxic lesions. MVM was seen in 13 cases (13/20, 65%), and FVM in 9 (9/20, 45%); there was no high grade MVM or FVM. Meconium staining of the membranes was frequent (9/20, 45%). Inflammation was observed in 11 placentas (55%). Ascending intrauterine infection was mild only (S1, G1 maternal/fetal response). Two cases showed high-grade, patchy VUE and five chronic deciduitis (of which only one also had VUE).
Finally, high BW/PW ratio (Category 3 lesions) was seen in 4 cases.
Severe/high grade lesions were seen in the PAIS placentas only, with the exception of high-grade VUE that was seen in both PAIS and control placentas. Statistical significance (p = 0.0398) was reached for severe ascending intrauterine infection, defined as S3 and/or G2 maternal and/or fetal inflammatory response.
Twin placentas: affected twin vs. co-twinIn all three twin pregnancies, one twin developed neonatal stroke, while the co-twin remained unaffected. Signs of hypoxia were seen in both disks/portions from the affected, and unaffected co-twin, but no co-twin portion showed histological features from more than one category. Differences between the two placental disks/portions are reported in detail below.
Placenta #14: early preterm dichorionic-diamniotic twin placentaThe disk from the affected twin showed extensive hypoxic lesions, with high grade FVM, and severe MVM with infarcts, affecting approximately half the placenta disk volume, together with signs of prolonged chronic hypoxia. There were mild differences in relative placental volume, the affected twin receiving 40% of the total volume. Finally, low-grade focal VUE was seen in the affected twin disk only.
Placenta #15: preterm monochorionic-diamniotic twin placentaThe placental portion from the affected twin showed features from all three categories. Volume distribution was highly heterogeneous, with only 20% of the volume attributed to the affected twin. High-grade, patchy VUE was seen in this portion only, as well as low grade FVM. The much larger placental volume devoted to the unaffected twin showed only minor hypoxic features, with peripheral infarcts representing < 2% of the volume (in a preterm placenta however).
Placenta #16: term fused dichorionic-diamniotic twin placentaThe two disks showed chorangiosis (adaptation mechanism) and signs of acute hypoxia. The disk from the affected twin showed additional hypoxic features, meconium staining of the membranes, and decidual arteriopathy.
A comparison of the prevalence of severe or high grade lesions between affected neonates and controls is provided in Table 2. The detailed histological features of the control placentas can be found in Supplemental Tables S2 and S3.
Table 2 Severe/high grade lesions: comparison between placentas from affected neonates and controls
留言 (0)