
記住我



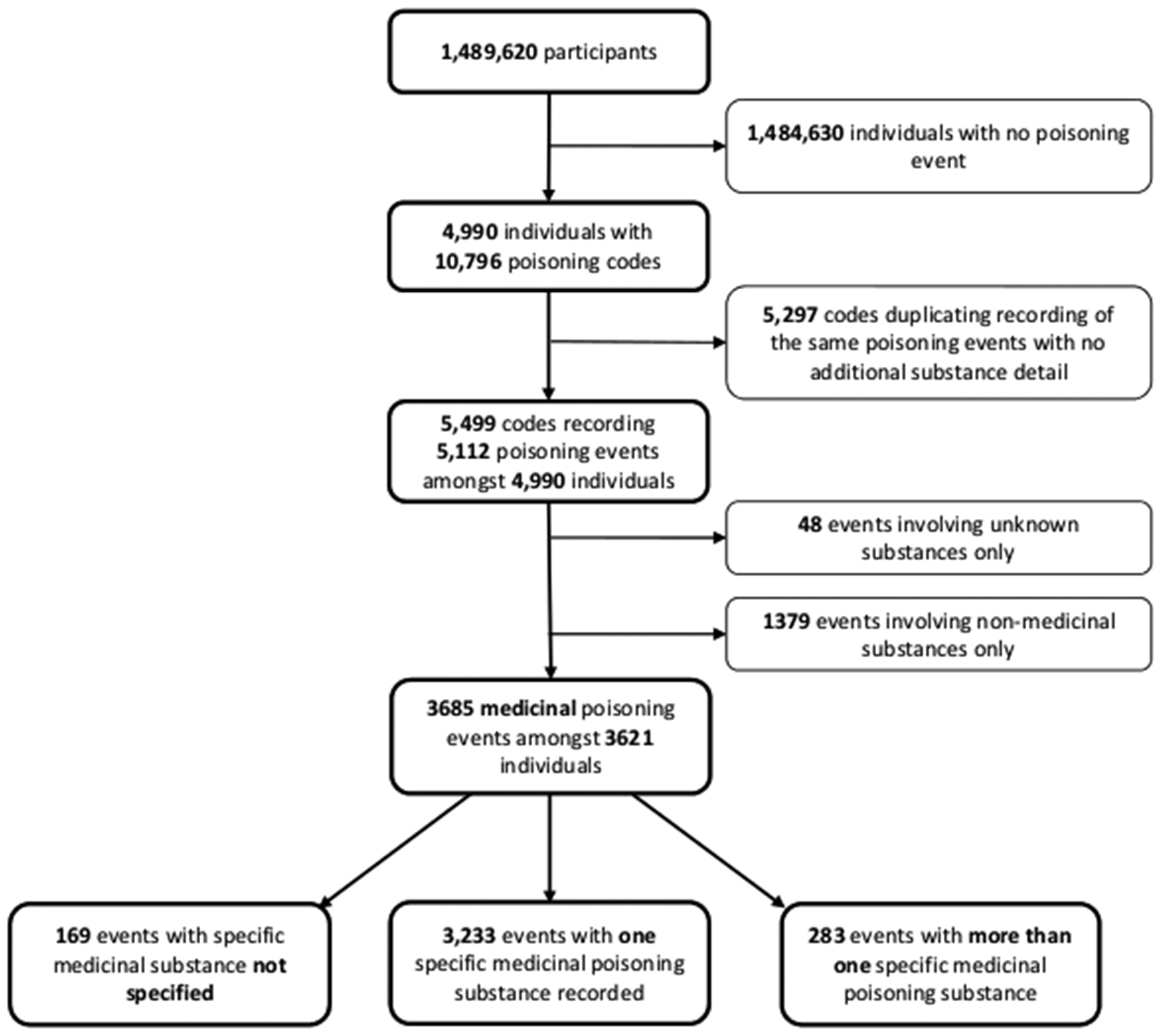
Sixteen patients with RA were interviewed, nine women and seven men, and all agreed to a follow-up CV screening. The duration of the interviews was not predetermined before the interviews took place. The duration of each interview varied, ranging from 15 to 59 minutes with a median duration in 28 minutes. Due to the COVID-19 pandemic the participants were provided with the flexibility to choose among face-to-face interviews, online, or telephone interviews. Notably, a majority of participants—specifically, nine in total—opted for telephone interviews. Importantly, it is worth highlighting that conducting interviews over the phone did not seem to compromise the quality or depth of information gathered, a perspective supported by Novick [20]. Additionally, one participant chose an online interview, while six participants opted for face-to-face interviews conducted at the hospital. The participants’ sociodemographic characteristics are presented in Table 1.
Table 1 Sociodemographic characteristics of the included participantsThe analysis derived two main themes: Accepting an offer and Living with a chronic disease and embracing changes. Accepting an offer was described by two sub-themes: Engagement in the screening consultation and Risk awareness. Living with a chronic disease and embracing changes was described by the sub-themes Motivation for lifestyle changes and Strategies to achieve lifestyle changes (Fig. 2).
Fig. 2
Aims of the study, and the themes and sub-themes derived from the analysis
In the following, the main themes and sub-themes are described in detail and illustrated by selected quotes.
First main theme: accepting an offerThe participants described different reasons for taking part in the screening. Furthermore, some participants described the awareness and understanding of the CV risk as the reasons for accepting both the initial invitation but also adhere to the follow-up.
Sub-theme: engagement in the screening consultationThe decision to participate in CV screening was based on factors such as having the time for it, that the screening will do no harm, or simply that it was an offer presented by the hospital.
It's a screening that is done every 3 years. And it was 3 years ago since I last had it done, and it's just part of the package at the Danish Hospital for Rheumatic Diseases. (Male, high-risk)
For others, their engagement in the screening was motivated by the desire to positively contribute to the benefit of others with the same diagnosis.
If one can contribute to something positive for others and perhaps gain something from it oneself, isn't that the hope? That's what I'm expecting to come out of it, at least. (Male, high-risk)
Furthermore, for some of the participants, the screening served as a means of conducting a status check to ensure everything was in order and determine if any modifications were required. The consultations served as a means for participants to engage in periodic monitoring, acting as a proactive measure to address potential issues before they could escalate into significant problems.
Well, it's not a pleasant thought to have, but then I think that if I get checked occasionally to see if it has settled anywhere, then I'm aware of it and will react if something is wrong. (Female, low-risk)
The participants regarded their consultation with the nurse as a good experience and expressed a sense of appreciation towards the nurses. They found the nurses to be pleasant and kind during the interaction, which contributed to their overall satisfaction with the consultation. Some participants felt that the screening did not provide any new insights, as they were already well informed. Some were even concerned that discussions on lifestyle and the measures taken might make individuals feel judged and that it could be intimidating.
The only thing one could think during this conversation was: "Oh no, now you'll have to be weighed and found too heavy," and that might discourage some people. (Female, low-risk)
A feeling of being disappointed that they were not invited for yet another follow-up screening was also described. Before inclusion in this study, a few participants had declined further follow-up. They explained that it was because the screening was the same every time.
Oh, once a year I think... Yeah. But I don't do it anymore. It's over... It was the same we talked about every time. It doesn't matter, I'm doing fine. (Female, low-risk)
Sub theme: risk awarenessOne of the reasons for accepting an invitation for screening was the awareness of the increased risk of CVD in patients with RA, a family history of CVD, and the desire to gain knowledge about the associated risk factors and preventive measures. This understanding of the risks and the opportunity to learn about prevention served as a primary reason for their participation and willingness to engage in follow-up consultations.
Yes. I had a certain fear that it had gotten worse. I mean, it wasn't good to begin with, and then I thought, "Hey, maybe I should just check if it had gotten worse, you know." I don't really feel like ending up like a vegetable because of a heart issue, heart failure, you know. So that was the reason why I wanted to see if it had gotten worse. (Male, high-risk)
The participants recalled their risk for CVD being presented via the SCORE risk chart, which was described as an effective and easily comprehensible method for illustrating their risk by the participants.
The risk is clearly shown on the chart with the green fields, where everything was fine, and then a red one appeared. So, it was proven on paper, you could say. I thought that was very good. (Male, high-risk)
When directly questioned about their recollection of the risk SCORE calculated by the nurse, most participants could remember their risk assessment. While some participants faced challenges in recalling the exact numerical value, they were able to recall whether their risk fell into the green, yellow, or red category, or if it was classified as low, moderate, or high. The scheme's emphasis on risk visualization was enhanced by the use of colors, notably observed when the risk level transitioned from green to red upon a participant's disclosure of being a smoker, highlighting the impact of smoking on their risk.
Yes, everything was green until they mentioned that I smoke. Then a red one appeared. (Female, high-risk)
The familiarity of these colors, commonly associated with "danger" for red and "good" for green, facilitated the participants' recognition and interpretation, as they are frequently employed in various contexts outside of the screening, making them easily understandable for the patients.
I don't necessarily need it in color, but, you know, we're familiar with the system from traffic lights with red, yellow, and green. You can say, "Now I'm in the green, that's where I should be." There's a light green and a dark green, where it shifts from 0 to 1, but that's related to age, and people can easily understand that. The darker it gets, the worse it is. (Male, low-risk)
For some, the scheme was a helpful repetition and provided a comprehensive explanation of the numbers.
Well, I think that's good because then you can also see the result from last time, and you can still track whether you are on the right track, so to speak. (Female, low-risk)
For others, the illustration of their risk made them intentionally avoid looking at the scheme. A few participants stated that there was no discussion regarding the risk SCORE during their screening. Other participants admitted that they had not given much thought to the conversation with the nurse. The risk of CVD was perceived as a highly serious matter, but also that risk is just a part of life. However, some participants felt no need for any changes, despite their risk.
Um, somewhere between quite high and high (laughs). Yeah, well, they claim, persistently, that I was, or am, overweight. And that's it. But, as I said, those cardiovascular diseases haven't really made me lose weight. (Male, high-risk)
The need for further attention and support for those who were at high risk and to ensure they received appropriate interventions and resources to decrease their CV risk were stated by some of the participants. One participant emphasised that simply receiving good advice and information on CV risk are insufficient to drive lasting changes and felt that knowing that you are accountable to someone or receiving regular check-ins makes it easier to stay on track.
Attending other offers were also a part of the discussion with the nurse and some had been referred to other health professionals i.e., a dietician. Many of the participants were either already visiting their GP or were recommended or informed by the nurse of the opportunity and importance of attending yearly visits with their GP due to their CV risk. Some participants discussed the necessity of attending both the screening and the yearly GP visit, where a yearly check-up with the GP was preferred by some. Others described a feeling of not getting the same type of information on CV risk when attending the screening and at the GP.
Actually, it has been nice to be able to talk with her [the screening nurse] about it. Especially because you don't have the same conversations with your own GP. You just don't, and not even with the doctor here [rheumatologist at the hospital]. There were two years when I wasn't here at all, and the last two years I've had different doctors. So, it's not easy either. You don't really establish a relationship with them. (Female, low-risk)
In addition to the screening, some participants had expected and wanted a more extensive check of the heart to be incorporated. Some were left with a fear of not knowing if everything was all right in terms of their heart.
You don't have the sensation of: "Wow, this [the CV screening] is wonderful. Currently, there's nothing wrong," even though you know the risk is there. I don't know if there's anything wrong. Not even after that conversation. (Female, low-risk)
Second main theme: living with a chronic disease and embracing changesMotivation for lifestyle changes was described in terms of a desire for change, and the need to prioritise making changes in everyday life. The importance of awareness of their CV risk and a social network were mentioned as strategies to achieve lifestyle changes in terms of physical activity and potential adherence to lifestyle changes.
Sub theme: motivation for lifestyle changesQuitting smoking, adopting healthier eating habits, and increasing physical exercise were mentioned as areas for improvement where the participants wished to make changes. During the screening sessions, the nurse provided participants with lifestyle recommendations and suggested areas for potential changes. The recommendations emphasised the importance of a healthy diet, with specific instructions on dietary changes and a better understanding of nutrition to manage cholesterol levels effectively.
They talked about what cholesterol levels and nutrition can do for cardiovascular diseases. (Male, low-risk)
A key recommendation was to engage in activities that elevate their heart rate and incorporate more exercise into their daily routines. Following the conversation, many participants reported an enhanced focus on physical activity or disclosed that they had already prioritised it, attributing this change to improved emotional well-being and its positive impact on their everyday lives and disease management. The participants recognised the value of physical activity in enhancing their overall well-being, including its potential to improve symptoms related to their diagnosis.
It's probably the physical activity because I feel that it benefits me. (Female, low-risk)
They also recalled talking to the nurse regarding alcohol consumption. Several participants stated that they did not have any issues with alcohol and only drank alcohol on special occasions or sporadically. Many of the participants mentioned limited alcohol consumption due to medication and the potential risk of liver damage. Despite being aware of the recommendations, external factors or specific situations could potentially influence their decision-making, causing them to deviate from the recommendations.
Yes, of course, we did. Alcohol in relation to what I'm dealing with, in connection with the medication I'm taking, it's not a good combination. But every now and then, you forget about that when the party is good. (Male, high-risk)
The participants acknowledged that changing a lifestyle habit is a difficult task, with one individual going so far as to describe quitting smoking as the most challenging experience he had ever faced. According to the participants, the motivation must originate from within the individual. They expressed that true changes are possible when an individual is genuinely motivated and driven to make changes.
Yes, the only thing that really needs to happen is for me to pull myself together and get it done. I think it was called character strength in my childhood. (Male, high-risk)
Making small changes posed no difficulty for some of the participants. Others firmly believed that their current lifestyle did not require any modifications. They felt they were already physically active or felt content with their present lifestyle. Some felt that making changes would make no difference anyway due to old age and medication. In addition, some found it challenging to initiate any changes as they were satisfied with their current lifestyle.
I think changing lifestyle will be difficult for me. I might as well say it, because I feel good now, and why the hell should I change that? (Male, high-risk)
Sub theme: strategies to achieve lifestyle changesSome participants shared that their awareness of the risks and consequences associated with their unhealthy lifestyle habits, such as smoking or eating too much, served as a motivator to make changes. For some, the fear of relapsing and being on the edge served as a pivotal point to quit smoking. The strategies to quit smoking included adopting new routines and using distraction techniques. The participants acknowledged that they possessed knowledge regarding which lifestyle changes they considered beneficial or detrimental, particularly in relation to CV risk, but it did not always lead the lifestyle changes.
They've mentioned it, but apparently it hasn't fully sunk in. (Male, high-risk)
Quitting smoking was described as a difficult challenge. One participant shared the experience of using a bet with another person as motivation to quit smoking.
We had a bet. I had to work on New Year's Eve, and so did the other person. Ten minutes to twelve, I smoked my last cigarette. (Female, low-risk)
The participants described that in order to become more active, one must actively engage in activities and make a conscious effort. Embracing an active lifestyle, prioritising exercise, and simply being more physically active were common descriptions among the participants.
I might consider, every now and then, that even though I'm quite active now, I could incorporate a bit more exercise than I currently do… (Female, low-risk)
Furthermore, the participants emphasized the significance of being active with others and having a source of motivation when it came to physical activity. The presence of a supportive social network had a profound impact on the participants, with the majority expressing a preference for engaging in physical activity with others. They viewed physical activity as a social endeavor, where companionship played a crucial role. One participant mentioned that living with someone who was highly active had a positive influence on their own activity levels. Participating in physical activity with others was perceived as a commitment, fostering a sense of accountability.
At least having someone to do it with. It adds a sense of commitment when you have someone… We take turns driving. There are two of us. When you're alone, you might not go [exercising]. (Female, low-risk)
留言 (0)