
記住我

Arterial hypertension is associated with an increased risk of cardiovascular disease and event rates [1]. As a global major modifiable risk factor for morbidity and mortality, lowering of blood pressure (BP) has the potential to reduce the risks associated with arterial hypertension [2]. For the diagnosis of arterial hypertension, a correct BP measurement (BPM) is crucial, and to date, a standard cuff-based 24-hour (24h) BPM using a validated device is acknowledged as the standard to diagnose arterial hypertension [3–7]. Due to the limitations of standard cuff-based 24h BPM devices, an increasing number of cuffless BPM devices are available on the market with different technologies to measure or estimate BP. As those intended for standard cuff-based BPM devices are not applicable, specific generally accepted validation protocols are needed, to assess device accuracy, which had not been available until the 2023 published recommendations by the European Society of Hypertension [4,8–10]. Most cuffless BP devices require an initial calibration BPM (CalibBP), using a standard upper-arm cuff-based BPM device [8,10,11]. To track BP changes in relation to the CalibBP, an algorithm is used to translate the measured value, for example pulse transit time (PTT), into a BP value. Consequently, these devices may be more ‘tracking’ than ‘measuring’ devices. Whether larger physiological BP fluctuations can be tracked accurately by these devices or not is an important question, especially as traditional validation protocols for BP devices focus on static conditions over a limited period of time [8,10,11].
In a previous study, we found a significant difference between a cuffless 24h BPM device using PTT (TestBP) and a standard cuff-based 24h BPM device (RefBP) when comparing the results of simultaneously executed 24h BPM. The TestBP device resulted in higher BP values than the RefBP device, so the values of the different devices were not interchangeable [12,13]. It remains unclear, if this is due to a systematic overestimation by the TestB or due to specific limitations of the cuffless PTT-based device technology.
Therefore, aim of the present analysis is to analyse the ability of the TestBP device to follow changes of the BP levels over 24h after the initial CalibBP and in comparison to a standard RefBP device. In addition, we examined the effect of the difference between the CalibBP and the BP level over time (24 h, awake, asleep) on the difference between the two devices.
MATERIALS AND METHODS Ethical approval and study registrationFor this analysis, we pooled the data of the ‘Somnotouch-NIBP Compared to Standard Ambulatory 24 Hours Blood Pressure Measurement’ VAST study (ClinicalTrials.gov Identifier: NCT03054688) and the subsequent ‘Somnotouch-NIBP Compared to Standard Ambulatory 24 Hours Blood Pressure Measurement’ VAST prospective registry (ClinicalTrials.gov Identifier: NCT03975582). Trial protocols were approved by the local ethics committee (Ethikkomission Nordwest- und Zentralschweiz, Ethics Commission Northwest and Central Switzerland, EKNZ 2017–00323 und EKNZ 2019–00460) and registered in the U.S. trial registry clinicaltrials.gov. Informed consent was obtained from all participants, prior to study inclusion and the study was performed in accordance with the Declaration of Helsinki and its amendments, International Conference on Harmonization, Good Clinical Practice guidelines and applicable national laws and regulations. Anonymized data supporting the findings of this study are available from the corresponding author upon reasonable request.
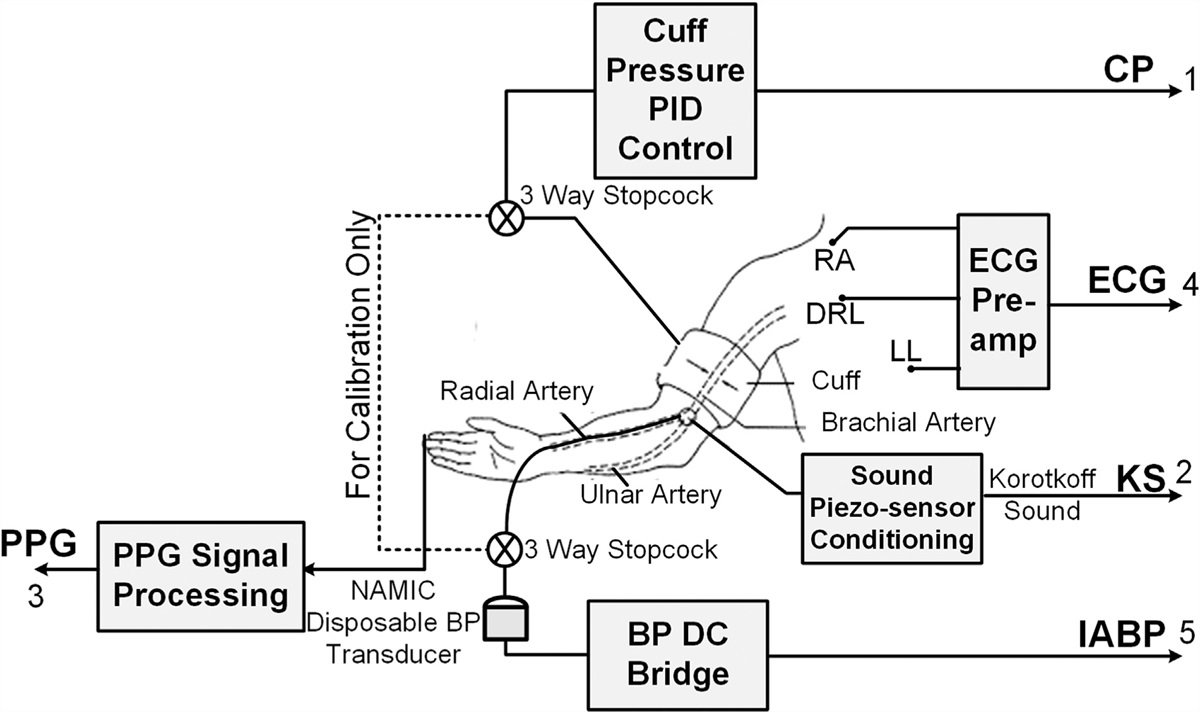
Device detailsAs test device, we used a cuffless, noninvasive 24h-BPM device, the Somnotouch-NIBP (Somnomedics GmbH, Randersacker, Germany), which allows continuous beat-to-beat BP monitoring. The device contains a finger photoplethysmograph and three ECG leads connected to a watch-like gadget with integrated actigraph. By using the PTT technique, the device measures the interval between the R-wave on the ECG and the signal of the corresponding pulse wave from the finger photoplethysmography (PPG) [14,15]. The system is first calibrated by an initial single cuff-based CalibBP on the contralateral upper arm [14,15]. Systolic (s) and diastolic (d) BP values are calculated using a nonlinear model integrating changes of the PTT and its relation to the CalibBP in a beat-to-beat fashion [15]. Summing up, an increasing pulse wave propagation resulting in shorter PTT correlates with a higher BP. Vice versa, a decreasing pulse wave propagation resulting in longer PTT correlates with a lower BP. Calculated BP can be affected by arterial wall stiffness and tension, which influence both pulse wave propagation and PTT [16,17]. The device is commercialized as validated according to the European Society of Hypertension International Protocol Revision 2010 [14]. The cuff-based reference devices used in the study were the Spacelabs 90217A (Spacelabs Healthcare Inc., USA), the Mobil-O-Graph (IEM GmbH, Aachen, Germany) and the Mobil-O-Graph PWA (IEM GmbH, Aachen, Germany) 24h BP monitor [18–20].
Study centre and familiarizationThe TestBP device was implemented in April 2015 at the Medical Outpatient and Hypertension Clinic at the University Hospital Basel. The whole study team was familiar with using the TestBP device correctly in clinical practice and trials. Cuffless BPM (TestBP) and standard cuff-based BPM (RefBP) were analysed and interpreted by experienced cardiologists and hypertensiologists (TB, ASV).
RecruitmentBetween May 2017 and February 2022, recruitment took place at the Medical Outpatient Department and Hypertension Clinic at the University Hospital Basel. The study team recruited healthy volunteers and patients with an indication for a 24h BPM. Inclusion criteria were age at least 18 years and the ability to give informed consent. Exclusion criteria were age less than 18 years, a SBP difference more than 10 mmHg between both upper extremities, atrial fibrillation at the time of enrolment and other medical reasons prohibiting BP measurement on the upper extremities. The inter-arm BP difference was measured sequentially after 5 min of rest with a single measurement on the left and right upper arm, in a sitting, upright position with legs uncrossed and back supported by the use of a validated, cuff-based, oscillometric Omron HBP-1300-E device [21].
In the VAST study, we included participants according to specific recruitment goals [at least 15 participants in low (<135 mmHg), intermediate (≥135 and <150 mmHg) and high (≥150 mmHg) mean awake SBP categories] to ensure distribution over a broad range of BP values and used exclusively Spacelabs devices as reference device [12,13]. The VAST prospective registry was the subsequent extension, opened to all patients with a clinical indication for 24h BPM. In addition, we used the Spacelabs and Mobil-O-Graph devices according to disposability in the prospective VAST registry. Recruitment for the VAST study was open until all recruitment goals were achieved. From the prospective VAST registry, we used data of participants recruited until February 2022. We used standardized questionnaires to evaluate personal and medical factors including intake of antihypertensive medication and biometrics.
Measurement procedureThe measurement procedure was previously reported in detail [12,13]. For calibration, participants were in a sitting, upright position with legs uncrossed and back supported when both devices were attached. An appropriately sized cuff connected to the RefBP device was placed on the right arm. According to the manufacturer's instructions, the TestBP device was placed on the left forearm. The device was connected to the finger photoplethysmograph on the left index finger and to the ECG electrodes (Fig. 1a). After 5 min of rest, the first manually triggered RefBP was used as CalibBP for the TestBP device. The study team programmed the RefBP device for BPM every 20 min from 08 : 00 to 22 : 00 and every 30 min from 22 : 00 to 8 : 00. The RefBP and TestBP devices were then worn simultaneously for 24 h, during which period the participants were instructed to follow their usual daily business. Individual participant diaries were used to define awake and asleep times. TestBP was monitored simultaneously beat-to-beat on the left arm.
 FIGURE 1:
FIGURE 1: Sample participant. (a) Arrangement of TestBP and RefBP devices. (b) Result of this sample participant in a plot comparing the difference between the RefBP and the TestBP (here -31 mmHg) with the difference between the CalibBP and the RefBP (here 27 mmHg), exemplarily systolic 24 h mean. (c) TestBP of a sample participant with the SBP in Red, DBP in purple. The CalibBP is framed in red, the awake BP in yellow, the asleep BP in blue, and the 24 h mean BP in brown. The systolic CalibBP is 161 mmHg, the systolic 24 h mean is 165 mmHg. (d) RefBP of the same sample participant. The CalibBP is framed in red, the awake BP in yellow, the asleep BP in blue, and the 24 h mean BP in brown. The systolic 24 h mean is 134 mmHg, thus resulting in a s24hRefBP - s24hTestBP of 134 mmHg - 165 mmHg = -31 mmHg, and a sCalibBP - s24hBP of 161 mmHg - 134 mmHg = 27 mmHg.
The RefBP were analysed by its own dedicated analysis software (Spacelabs Healthcare Inc, USA and Mobil-O-Graph, IEM GmBH) after the 24 h BPM. If the RefBP device measured a minimum of 27 BP values, the data set was valid, if not the data set was excluded [22]. Mean systolic and diastolic 24 h, awake and asleep BP values were calculated. For all TestBPs, we used two methods of heart beat detection and ECG interpretation for BP calculation. The TestBPs were first evaluated by the automatic heart beat detection algorithm included in the Domino Light software package (Domino Light V1.5; Somnomedics GmbH) after choosing the ECG lead with best signal quality. Then all TestBPs were evaluated by the optional Schiller Darwin 24 h ECG software package (Medilog Darwin V.2.5.2.52; Results can be found in the appendix, https://links.lww.com/HJH/C388). As a quality criterion for the RefBP, data sets were considered as valid and included in the analysis in case of less than 50% artefact time. The results of a sample participant are depicted as Fig. 1c (TestBP) and Fig. 1d (RefBP).
Evaluation of the relationship between CalibBP and TestBP valuesPrevious results from the VAST and other studies have shown that on average the TestBP device results in higher BP values than the RefBP device [12,13,23]. One hypothetical reason for this phenomenon is a decreased detection of BP changes by the TestBP device [23]. Considering that the BP values calculated by the cuffless system depend on the CalibBP, we calculated the difference between the systolic CalibBP and systolic mean 24 h, awake and sleep values (sCalibBP – s24hBP, sCalibBP – sAwakeBP, sCalibBP – sAsleepBP) for the RefBP and the TestBP, respectively, and for the diastolic CalibBP and diastolic mean 24 h, awake and sleep values (dCalibBP – d24hBP, dCalibBP – dAwakeBP, dCalibBP – dAsleepBP) for the RefBP and the TestBP, respectively (Fig. 1b,d). A larger positive difference therefore indicates a drop of the BP values in comparison to the CalibBP – in the sense of a white-coat effect, whereas a negative difference indicates an increase of the BP values in comparison to the CalibBP – in the sense of a masked hypertension effect. We interpret these differences as a surrogate marker for the extent of changes in the BP levels over 24 h that can be tracked by the devices after an initial CalibBP for the TestBP device, or after a first measurement for the RefBP device.
In order to investigate the influence of the BP level changes after the initial CalibBP on device agreement, we plotted the difference between CalibBP and the RefBP against the difference between the RefBP and the TestBP (Fig. 2).
 FIGURE 2:
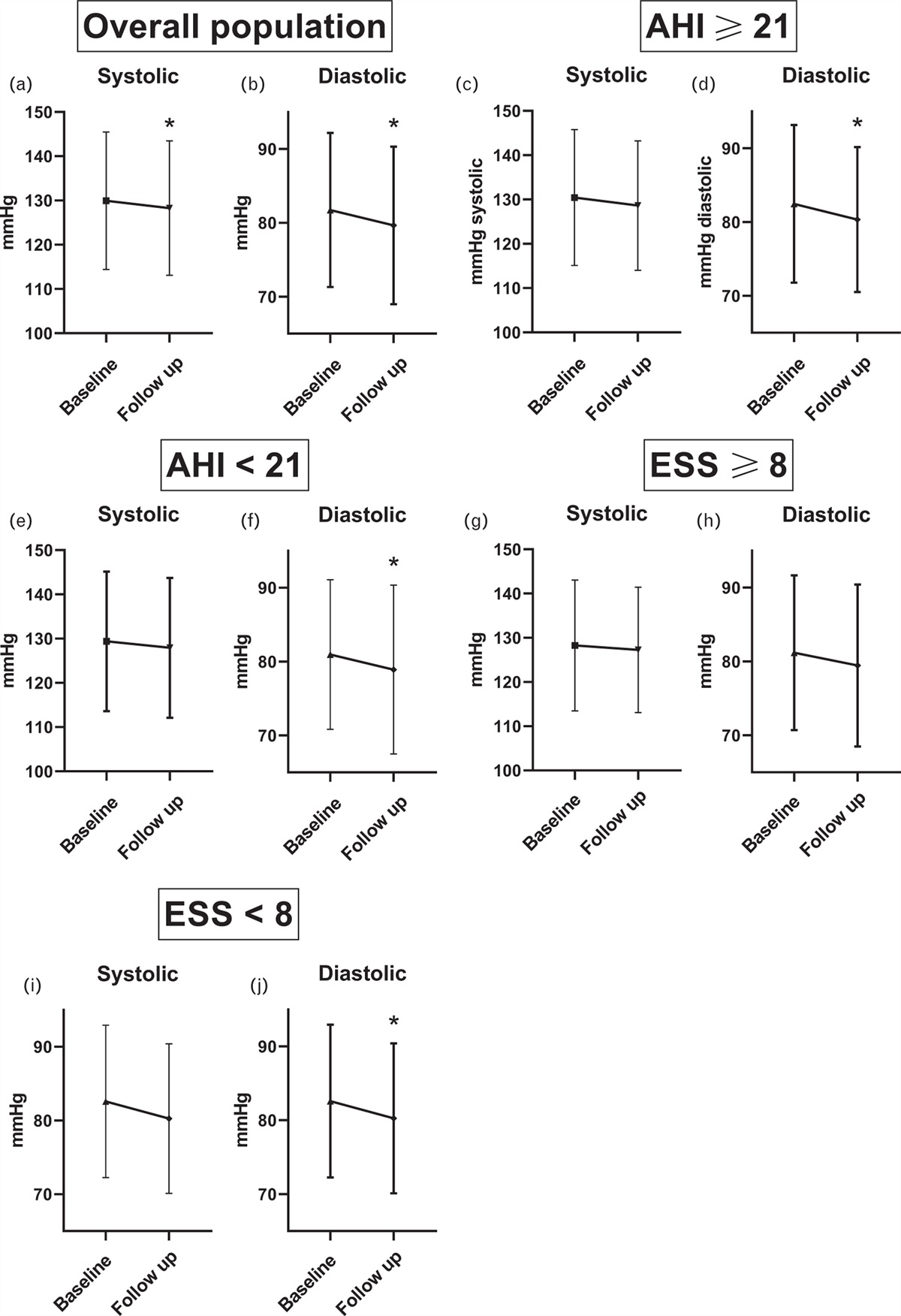
FIGURE 2: Explanations for comparison plots: (a) The green vertical line represents a hypothetical perfect correlation between TestBP and RefBP, the red line a hypothetical TestBP which is exactly equal to the CalibBP. (b) A hypothetical TestBP with a systematic error in comparison to the RefBP would be depicted in a horizontally displaced vertical line. (c) Shifting of a measurement point in a vertical direction depicts a difference between the CalibBP and the Reference BP with the upper half of the plot representing CalibBP values higher than the RefBP (white-coat pattern, at least as a tendency), and the lower half representing CalibBP values lower than the RefBP (masked pattern, at least as a tendency). (d) Shifting of a measurement point in a horizontal direction depicts a difference between TestBP and RefBP with the left side of the plot representing TestBP values higher than the RefBP and the right side of the plot representing TestBP values lower than the RefBP.
Statistical analysisContinuous data were presented as means ± standard deviation (SD) and categorical variables as counts (percentages). The differences between CalibBP and RefBP or CalibBP and TestBP were compared using a one-sided Wilcoxon signed-rank test by hypothesizing a minor BP difference between CalibBP and TestBP compared to CalibBP and RefBP. For the possible relationship between the difference of the CalibBP and the awake RefBP, we first tested visually for linearity in a scatter plot. Then, we applied a linear regression model. Following results include TestBPs evaluated by the Domino Light software (Domino Light V1.5; Somnomedics GmbH). Results for TestBPs evaluated by the optional Schiller Darwin 24h ECG software package (Medilog Darwin V.2.5.2.52) can be found in the appendix (Tables A1, A2, https://links.lww.com/HJH/C388 and Figures A2, A3, https://links.lww.com/HJH/C388). All statistical calculations and figures were performed using R version 4.1.3 and using the package ‘tidyverse’. A P value of less than 0.05 was prespecified to indicate statistical significance and a P value of less than 0.0001 as highly statistically significant.
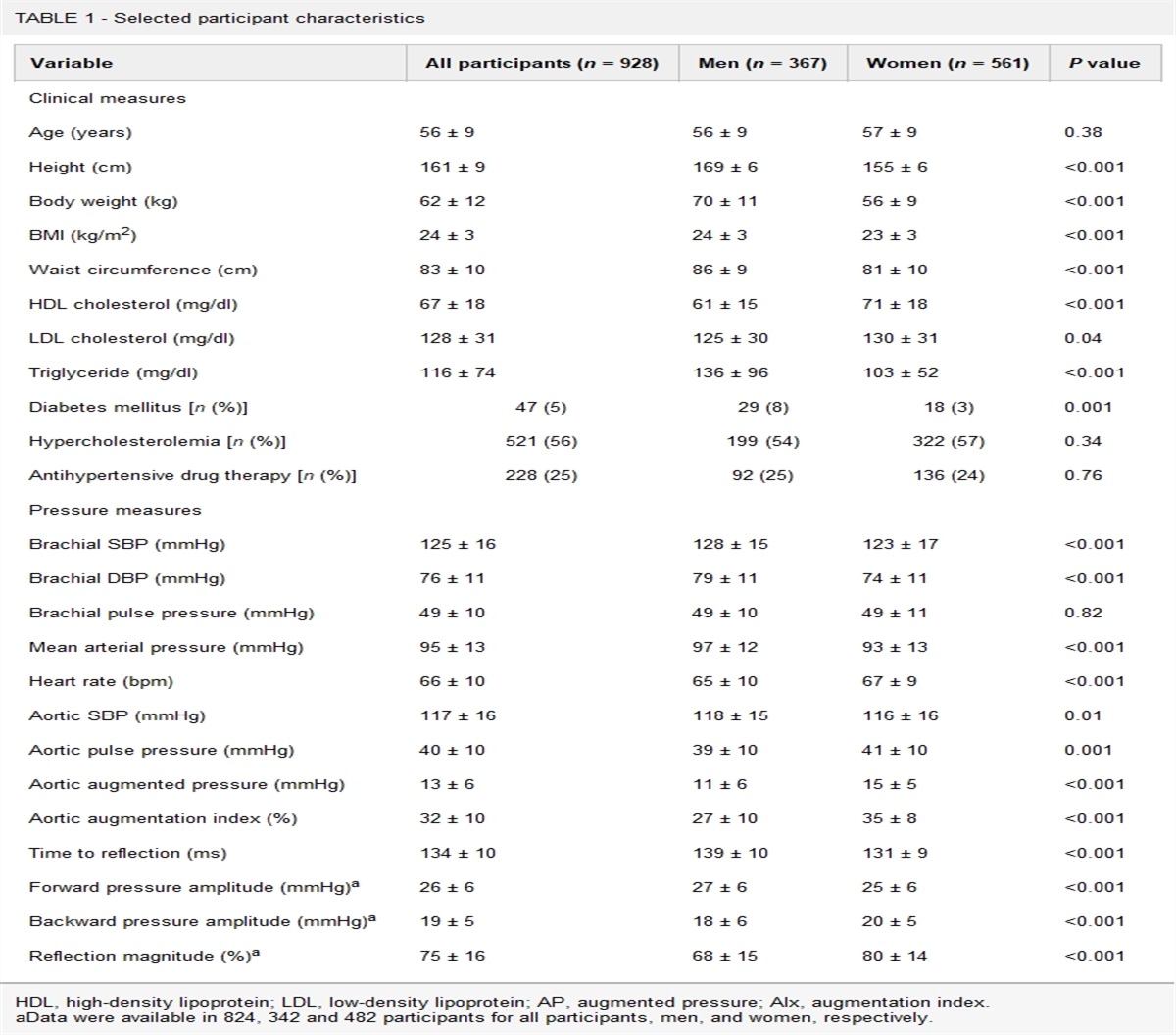
RESULTS Baseline characteristicsBetween May 2017 and February 2022, 198 participants were enrolled in total for the study (83 participants for the VAST study and 115 for the VAST prospective registry). As previously published, 12 out of 83 participants had to be excluded in the VAST study, mainly due to insufficient recording time or quality of the devices, resulting in a final cohort of 71 participants [12]. Twenty out of 115 participants were excluded from the VAST prospective registry due to insufficient recording quality of the TestBP device (n = 12) or missing data (n = 8). Finally, a total of 166 participants’ data (84%) were included for the present analysis. Baseline characteristics are summarized in Table 1. Mean age was 51.2 years, 53.0% of the study population were men and 55.4% received antihypertensive treatment at enrolment. Mean SBP and DBP (SD) of the CalibBP were 137.3 (18.2) and 86.0 (11.8) mmHg, respectively. Mean heart rate (SD) of the calibration measurement was 72.5 (12.4) bpm.
TABLE 1 - Baseline characteristics Characteristic Overall (n = 166) Sex (male), n (%) 88 (53.0) Age, years; mean (SD) 51.2 (15.1) Height, cm; mean (SD) 173.2 (10.0) Weight, kg; mean (SD) 81.0 (19.1) BMI, kg/m2; mean (SD) 26.9 (5.3) Arm circumference, cm; mean (SD) 30.4 (3.8) (n = 165) Nonsmoker, n (%) 102 (61.4) (n = 165) Previous smoker, n (%) 43 (25.9) (n = 165) Active smoker, n (%) 20 (12.0) (n = 165) Health perception; mean (SD) 81.5 (17.3) (n = 161) Diabetes, n (%) 18 (13.2) (n = 136) CAD, n (%) 10 (7.5) (n = 134) CVI/TIA, n (%) 4 (3.0) (n = 134) Antihypertensive treatment, n (%) 92 (55.4) Valid 24-h cuff-based BP readings; mean (SD); [range] 59.5 (6.6) [33–71] sCalibBP, mmHg; mean (SD); [range] 137.3 (18.2) [96–199] dCalibBP, mmHg; mean (SD); [range] 86.0 (11.8) [58–131] CalibHR, bpm; mean (SD); [range] 72.5 (12.4) [41–114]Data are mean (± standard deviation) [range] or counts (percentage), as appropriate.CAD, coronary artery disease; CalibBP, Calibration BP measurement; CVI, cerebrovascular insult; d, diastolic; HR, heart rate; s, systolic; TIA, transient ischemic attack.
Mean systolic 24 h BP for RefBP and TestBP were 129.9 and 135.5 mmHg (P < 0.0001), respectively. Mean diastolic 24 h BP for RefBP and TestBP were 79.4 and 84.4 mmHg, respectively. Mean 24 h heart rate measurements for RefBP and TestBP were 70.3 and 74.2 bpm, respectively. Results for the comparison of awake and asleep BP values between the cuff-based and the TestBP device are summarized in Table 2. Regarding BP classification, 23% of participants were misclassified as having elevated mean systolic 24 h BP by the TestBP compared to RefBP, whereas 4% were misclassified as normal (Figure A1 a, Appendix, https://links.lww.com/HJH/C388). Results for mean diastolic 24 h BP as well as analysis for participants with and without antihypertensive medication are shown in Figure A1 b--f, https://links.lww.com/HJH/C388).
TABLE 2 - Comparison of RefBP and TestBP results RefBP TestBP P s24hBP, mmHg; mean (SD) 129.9 (14.4) 135.5 (9.8) <0.0001 sAwakeBP, mmHg; mean (SD) 133.8 (12.8) 139.3 (8.8) <0.0001 sAsleepBP, mmHg; mean (SD) 119.8 (10.8) 130.2 (7.2) <0.0001 d24hBP, mmHg; mean (SD) 79.4 (11.0) 84.4 (5.9) <0.0001 dAwakeBP, mmHg; mean (SD) 82.7 (9.5) 87.4 (4.4) <0.0001 dAsleepBP, mmHg; mean (SD) 70.9 (8.6) 80.3 (4.3) <0.0001 24hHR, bpm; mean (SD) 70.3 (10.5) 74.2 (14.3) <0.0001 AwakeHR, bpm; mean (SD) 73.6 (9.6) 78.8 (13.6) <0.0001 AsleepHR, bpm; mean (SD) 62.1 (5.9) 63.5 (8.3) <0.0001Data are mean (± standard deviation).BP, blood pressure; d, diastolic; HR, heart rate; RefBP, standard cuff-based BP measurement; s, systolic; TestBP, cuffless BP measurement.
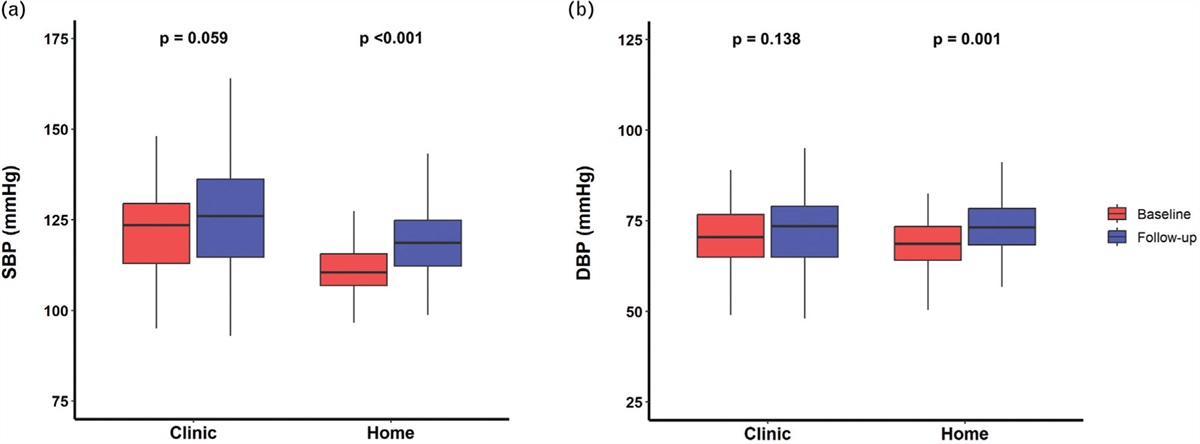
The mean difference between CalibBP and mean 24h, awake and asleep BP values, respectively, was significantly lower for the TestBP than the RefBP for both systolic and diastolic values (P < 0.0001 for all comparisons). Complete results, including mean, SD and ranges for the systolic and diastolic differences, are presented in Table 3. Boxplots comparing the difference between sCalibBP or dCalibBP during the different measurement periods of the TestBP and RefBP (Fig. 3a,b) show significantly different median BP values and visually wider interquartile ranges and whiskers of the cuff-based BP device (purple) compared with the cuffless BP device (orange).
TABLE 3 - Comparison of the differences between the CalibBP and the mean BP of the RefBP and TestBP device RefBP, mmHg; mean (SD) RefBP, mmHg; range TestBP, mmHg; mean (SD) TestBP, mmHg; range P sCalibBP -s24hBP 7.4 (13.2) -35 – +55 1.8 (8.3) -15 – +34 <0.0001 sCalibBP - sAwakeBP 3.5 (13.3) -33 – +51 -2.0 (7.6) -25 – +28 <0.0001 sCalibBP - sAsleepBP 17.5 (15.6) -41 – +65 7.1 (10.8) -14 – +39 <0.0001 dCalibBP - d24hBP 6.6 (6.8) -12 –+ 32 1.6 (5.8) -24 – +27 <0.0001 dCalibBP - dAwakeBP 3.3 (7.0) -12 – +29 -1.5 (5.1) -28 – +24 <0.0001 dCalibBP - dAsleepBP 15.1 (8.7) -15 – +41 5.7 (8.0) -20 – +35 <0.0001Data are mean (± standard deviation) or range.BP, blood pressure; CalibBP, calibration BP measurement; d, diastolic; RefBP, standard cuff-based BP measurement; s, systolic; TestBP, cuffless BP measurement.
 FIGURE 3:
FIGURE 3: Boxplots comparing the difference between the systolic (a) or diastolic (b) CalibBP and the systolic (a) or diastolic (b) 24h, awake and asleep RefBP (purple) / TestBP (orange) with P values generated by a one-sided Wilcoxon signed-rank test.
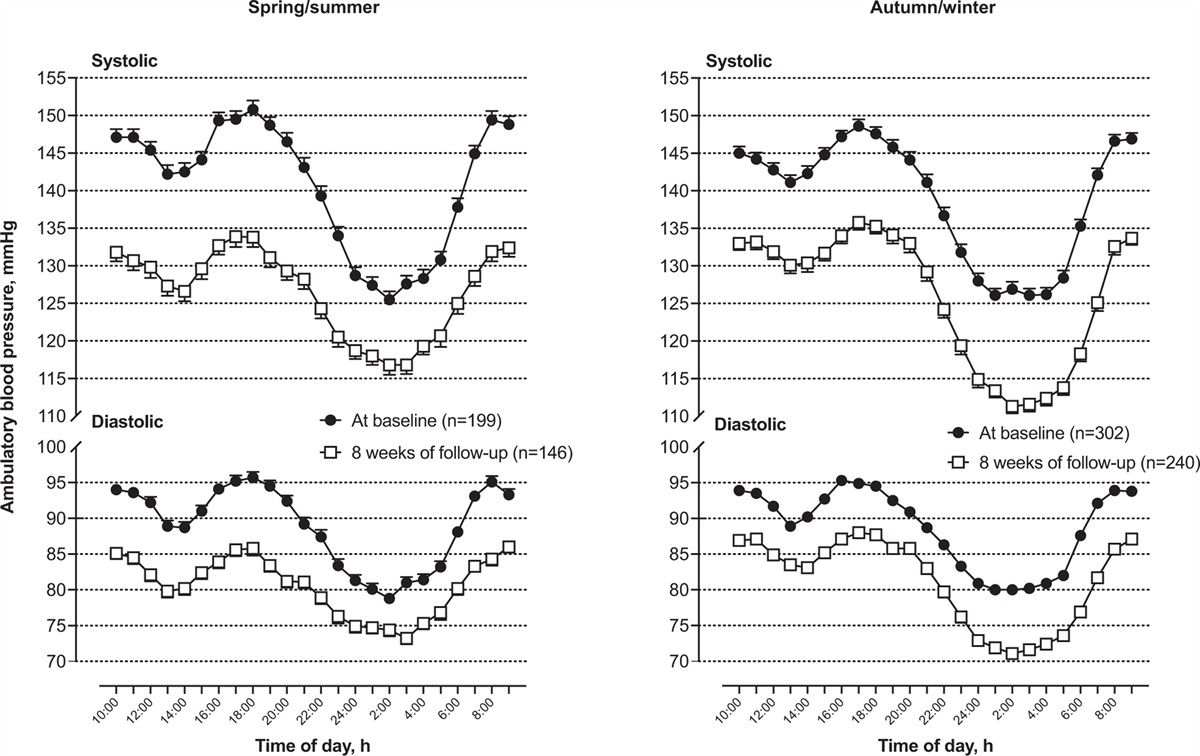
Influence of the difference between the CalibBP and the mean 24 h, awake and asleep RefBP on the agreement between the RefBP and TestBPAnalysing a possible relationship between the difference of the CalibBP and mean 24 h, awake and asleep RefBP, and the agreement between the RefBP and TestBP, we found a nearly linear inverse relationship, shown in Fig. 4a--f. In other words, a higher positive difference between CalibBP and mean 24 h RefBP (white-coat effect) is associated with a larger negative difference between RefBP and TestBP values (TestBP results in higher values than the RefBP) and vice versa (Fig. 4). This shows that the values calculated by the TestBP device stay closer to the CalibBP in case of a white-coat effect as well as a masked hypertension effect. This inverse linear relationship was seen for systolic (Fig. 4a, c, e) and diastolic (Fig. 4b, d, f) BP measurements. The blue line depicts the linear regression for the data. To increase readability, we have added a red and a green line to the Fig. 4 with the red line indicating the theoretical situation that TestBP follows CalibBP without any tracking of changes in BP levels and green line indicating the theoretical situation of an ideal agreement of RefBP and TestBP (see additional Figure 2).
 FIGURE 4:
FIGURE 4: Plots comparing the difference between systolic or diastolic CalibBP and 24h, awake and asleep systolic or diastolic RefBP on the y-axis and the difference between the 24h, awake and asleep systolic or diastolic RefBP and corresponding TestBP on the x-axis. Plots a, c, e are showing the SBP and plots b, d and f the DBP. BP blood pressure, CalibBP calibration BP measurement, d diastolic, RefBP standard cuff-based BP measurement, s systolic, TestBP cuffless BP measurement. Red line shows the assumption that TestBP follows CalibBP without changes, the blue line shows the generated linear regression for the data and the green line shows an ideal agreement between RefBP and TestBP.
DISCUSSIONThe present analysis is the first and largest study investigating the ability of a cuffless 24 h BPM device using PTT, namely the commercially available SOMNOtouch™ NIBP device, to track changes in BP levels after an initial calibration measurement during a 24 h BPM in comparison to standard cuff-based devices. As the device is intended for use by physicians, there are highest demands on device accuracy.
In line with previous studies, the mean BP values measured by the TestBP device were not interchangeable to the ones measured by the RefBP device [12,13,23]. The TestBP device usually results in higher BP values, however in some patients, namely the ones with an increase of the BP level after an initial calibration, it results in lower BP values. Our study now impressively adds that this is not due to a systematic overestimation of BP values.
Firstly, we could show that the ability of the cuffless BP device to track overall changes in the BP levels over 24 h was different compared to the standard cuff-based 24 h BPM device, especially in patients with a higher divergence of the overall BP levels from the CalibBP. This means that the cuffless BP device followed a limited range of overall BP changes after the initial CalibBP, as shown in Fig. 3. Due to our findings, we assume that the TestBP device may be less adequate to detect white-coat (WCE) or masked hypertension effects (MHE) in daily clinical practice and reflects less BP changes in patients, when a first BP measurement differs largely from the following measurements. In our cohort, the TestBP misclassified mean systolic or diastolic 24 h BP values, which were normal in the RefBP measurements, as elevated in approximately one out of five patients (Figure A1, Appendix, https://links.lww.com/HJH/C388).
Secondly and as the main result, this analysis showed an impressive near linear relationship of the difference between CalibBP and mean BP values measured by the RefBP device and the difference between the RefBP device and the TestBP device. In other words, the larger the difference between the CalibBP and the mean RefBP was, the worse the agreement between the two devices was found. This relationship illustrates again the missing ability of the TestBP device to track a falling or rising BP level in contrast to the CalibBP, as seen in patients with white coat or masked hypertension effects. Consequently, applied to clinical practice the TestBP device tend to overestimate BP in individuals with WCE and to underestimates BP in individuals with MHE effects, compared with standard devices.
To highlight these interrelations, we added the two reference lines into Fig. 4. The green line in Fig. 4 represents an ideal scenario with a vertical line crossing the x-axis at 0 mmHg, indicating a perfect agreement between the RefBP and the TestBP in all participants and patients. In case of a systematic overestimation or underestimation of BP values by the TestBP, the green line would be displaced in a parallel fashion to a positive or negative value on the x-axis (Fig. 4). In contrast, the red line indicates the hypothetical situation that the TestBP device replicates the CalibBP without any tracking or changes. When looking at the plots in Fig. 4, the blue regression line seems to be more closely related to the red line, than to the ideal green line or a systematic overestimation.
There had been studies showing a better ability to track BP changes with the PTT technique, but these were made under laboratory conditions, for example using dobutamine to modulate BP and comparing single PTT-derived BP values to intraarterial measurements [15,22]. Compared with these studies, we used a cruder surrogate marker for overall changes in BP after a CalibBP using mean values to reflect BP levels and, as stated in previous publications, we cannot accurately determine which BP measurement method is more accurate [12,13], for example compared with intra-arterial BP values. It may be possible, for example, that the lower number of measurements with the standard cuff-based device or the lack of individual measurements in phases of higher or lower BP may lead to a distortion of the mean values of the 24 h BP measurement and the cuffless device may better reflect the true BP values of a participant or patient over time. However, we have to keep in mind that all of the prognostic data for ambulatory blood pressure measurement (ABPM) regarding morbidity and mortality of patients with hypertension in general and with masked or white-coat hypertension in particular were collected with standard RefBP devices and standard measurement protocols as we used in our study [4,7,12,24,25].
The SOMNOtouch™ NIBP device and other cuffless BP devices have the potential to overcome limitations of traditional RefBP devices. Some patients poorly tolerate or accept the repeated cuff inflations, especially during night, when sleep can be interrupted, or cuff-inflations can induce BP changes [26–29]. Additional vital signs can be monitored, such as, in case of the SOMNOtouch™ NIBP device, a 24 h ECG, a pulse oximetry which may be used for screening of sleep related breathing disorders and an actigraphy. In accordance with the BP values, the TestBP device resulted in higher mean heart rates than the RefBP device, as already described by Lauder et al.[30] who found that cuff-based ABPM more commonly underestimated than overestimated HR compared with standard 24 h ECG recordings, although the difference in this study was smaller than in our cohort. Reasons for the difference between the devices may be the lower number of RefBP measurements especially during activity and the instruction of participants to keep their arm still and interrupt activities during cuff-based measurements.
Furthermore, ambulatory beat-to-beat BP monitoring has the potential to open a new field of dynamic BP evaluation, for example with regard to direct response to physical or emotional stress, or for the evaluation of symptom – BP correlation [8]. Cuffless devices may have the ability to track BP fluctuations over the whole measurement period, whereas cuff-based devices measure individual BP values even under ideal conditions only every 20 or 30 min and calculate a mean BP value over the measured period.
However, for all these advantages and questions [31–34], the data regarding PTT as well as PPG-devices are not yet sufficient, and recent studies like the Aurora Project or studies by Tan et al. [34] and Falter et al. [31] evaluating not PTT but PPG devices showed clear weaknesses of cuffless BPM to predict or accurately track BP changes. Accordingly, a consensus document of the European Society of Hypertension regarding cuffless BPM devices stated that they cannot be recommended for clinical use, until fundamental questions about accuracy, performance and implementation are carefully addressed [10].
Meanwhile, when using cuffless devices available on the market for clinical or research purposes, special attention should be made for a standardized CalibBP, as errors due to an insufficient CalibBP, for example due to short resting times or interaction with the patient during the measurement, can have a particular effect on the result of the cuffless BP measurement.
LimitationsIn our study, we focused on differences of the CalibBP to mean BP values for 24 h, awake and asleep periods of a 24 h BPM. We used this as a global surrogate marker for changes in the BP level of an individual patient. We could not examine the ability of the device to track directly short-time BP fluctuations, like it would, for example, be possible with a comparison to intra-arterial beat-to-beat measurements. However, we are convinced that this is also a strength of our work, as these mean values are used day by day for clinical decision making and therefore the awareness of differences between the measurement methods and devices is essential for the evaluation and treatment of a patient. The different devices were attached to contralateral arms with potential differences in BP values depending on arm positions or anatomic conditions. We tried to minimize this risk by screening all participants for a systolic interarm BP difference before participation in this study and we followed the manual of the cuffless device, which indicates to use the contralateral arm for the calibration measurements.
CONCLUSIONCuffless devices to monitor BP values over 24 h seem to be a promising tool to assess patients BP over a longer period in clinical practice. In our study, we showed that the tracked BP levels by a cuffless PTT device were not interchangeable with the BP values measured by the standard 24 h cuff-based devices. The cuffless device showed a lower ability to track mean changes of BP levels after an initial CalibBP compared with a standard cuff-based device.
In addition, the difference between the cuffless and the cuff-based device was nearly linearly associated with the difference between the CalibBP and the BP levels afterwards – the larger the BP change, the larger the difference between the two devices. For clinical practice, this means that the cuffless device may fail to detect white-coat or masked hypertension effects, compared with results of standard cuff-based devices.
ACKNOWLEDGEMENTSThe authors would like to thank all patients and volunteers for their participation in the study. In addition, we thank Simone Erne, Valerie Rincker-Junghänel and Irena Ferati for their help in patient and participants services.
Parts of this study were presented as oral presentation at the 32nd European Meeting on Hypertension and Cardiovascular Prevention (June 26th, Session Blood Pressure Measurement 2), taking place from June 23 to 26, 2023 at Milan, Italy.
This study was fully funded by the Medical Outpatient Department and Hypertension Clinic of the University Hospital Basel, Basel, Switzerland. There was no external funding.
Conflicts of interestA.S.V and T.B. have received funding for different BP measurement device studies from Centre Suisse d’Electronique et de Microtechnique (CSEM), Neuchatel Switzerland and Preventicus GmbH, Jena, Germany. There were no other conflicts of interest to disclose.
REFERENCES 1. Vasan RS, Larson MG, Leip EP, Evans JC, O’Donnell CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med 2001; 345:1291–1297. 2. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016; 387:957–967. 3. Stergiou GS, Palatini P, Asmar R, Ioannidis JP, Kollias A, Lacy P, et al. Recommendations and Practical Guidance for performing and reporting validation studies according to the Universal Standard for the validation of blood pressure measuring devices by the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO). J Hypertens 2019; 37:459–466. 4. Stergiou GS, Palatini P, Parati G, O’Brien E, Januszewicz A, Lurbe E, et al. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens 2021; 39:1293–1302. 5. Vischer AS, Burkard T. Principles of blood pressure measurement: current techniques, office vs ambulatory blood pressure measurement. Adv Exp Med Biol 2017; 956:85–96. 6. Whelton PK, Carey RM. The 2017 Clinical Practice Guideline for High Blood Pressure. JAMA 2017; 318:2073–2074. 7. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018; 39:3021–3104. 8. Lee HY, Burkard T. The advent of cuffless mobile device blood pressure measurement: remaining challenges and pitfalls. Korean Circ J 2022; 52:198–204. 9. Stergiou GS, Avolio AP, Palatini P, Kyriakoulis KG, Schutte AE, Mieke S, et al. European Society of Hypertension recommendations for the validation of cuffless blood pressure measuring devices: European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. J Hypertens 2023; 41:2074–2087. 10. Stergiou GS, Mukkamala R, Avolio A, Kyriakoulis KG, Mieke S, Murray A, et al. Cuffless blood pressure measuring devices: review and statement by the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. J Hypertens 2022; 40:1449–1460. 11. Mukkamala R, Yavarimanesh M, Natarajan K, Hahn JO, Kyriakoulis KG, Avolio AP, et al. Evaluation of the accuracy of cuffless blood pressure measurement devices: challenges and proposals. Hypertension 2021; 78:1161–1167. 12. Krisai P, Vischer AS, Kilian L, Meienberg A, Mayr M, Burkard T. Accuracy of 24h ambulatory blood pressure monitoring by a novel cuffless device in clinical practice. Heart 2019; 105:399–405. 13. Socrates T, Krisai P, Vischer AS, Meienberg A, Mayr M, Burkard T. Improved agreement and diagnostic accuracy of a cuffless 24h blood pressure measurement device in clinical practice. Sci Rep 2021; 11:1143. 14. Bilo G, Zorzi C, Ochoa Munera JE, Torlasco C, Giuli V, Parati G. Validation of the Somnotouch-NIBP noninvasive continuous blood pressure monitor according to the European Society of Hypertension International Protocol revision 2010. Blood Press Monit 2015; 20:291–294. 15. Gesche H, Grosskurth D, Kuchler G, Patzak A. Continuous blood pressure measurement by using the pulse transit time: comparison to a cuff-based method. Eur J Appl Physiol 2012; 112:309–315. 16. Callaghan FJ, Babbs CF, Bourland JD, Geddes LA. The relationship between arterial pulse-wave velocity and pulse frequency at different pressures. J Med Eng Technol 1984; 8:15–18. 17. Schiffrin EL. Vascular stiffening and arterial compliance. Implications for systolic blood pressure. Am J Hypertens 2004; 17:39S–48S. 18. Baumgart P, Kamp J. Accuracy of the SpaceLabs Medical 90217 ambulatory blood pressure monitor. Blood Press Monit 1998; 3:303–307. 19. Sarafidis PA, Lazaridis AA, Imprialos KP, Georgianos PI, Avranas KA, Protogerou AD, et al. A comparison study of brachial blood pressure recorded with Spacelabs 90217A and Mobil-O-Graph NG devices under static and ambulatory conditions. J Hum Hypertens 2016; 30:742–749. 20. Wei W, Tolle M, Zidek W, van der Giet M. Validation of the mobil-O-Graph: 24 h-blood pressure measurement device. Blood Press Monit 2010; 15:225–228. 21. Meng L, Zhao D, Pan Y, Ding W, Wei Q, Li H, et al. Validation of Omron HBP-1300-E professional blood pressure monitor based on auscultation in children and adults. BMC Cardiovasc Disord 2016; 16:9. 22. Patzak A, Mendoza Y, Gesche H, Konermann M. Continuous blood pressure measurement using the pulse transit time: comparison to intra-arterial measurement. Blood Press 2015; 24:217–221. 23. Nyvad J, Christensen KL, Buus NH, Reinhard M. The cuffless SOMNOtouch NIBP device shows poor agreement with a validated oscillometric device during 24h ambulatory blood pressure monitoring. J Clin Hypertens (Greenwich) 2021; 23:61–70. 24. O’Brien E, Parati G, Stergiou G, Asmar R, Beilin L, Bilo G, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens 2013; 31:1731–1768.
留言 (0)