
記住我
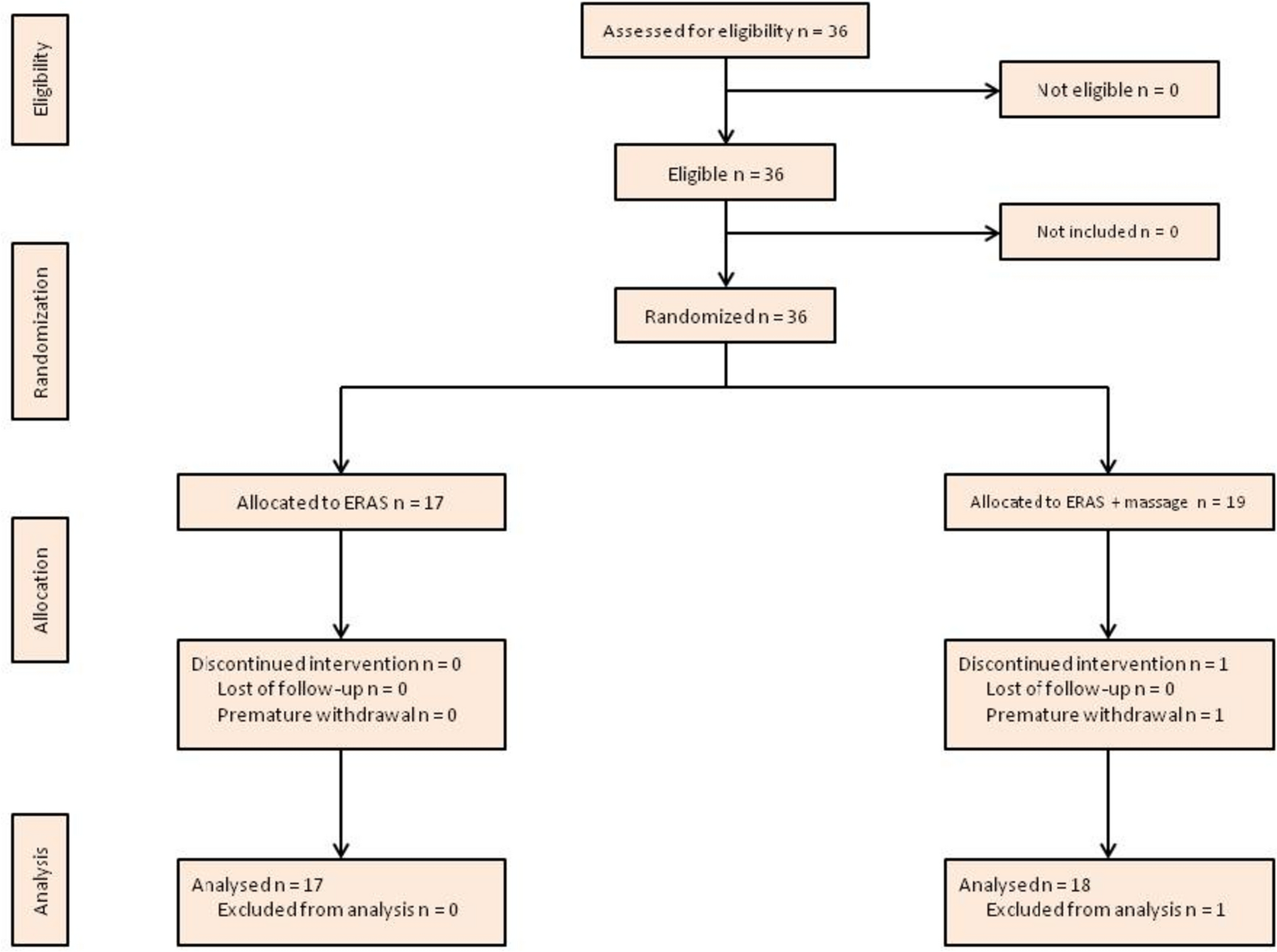
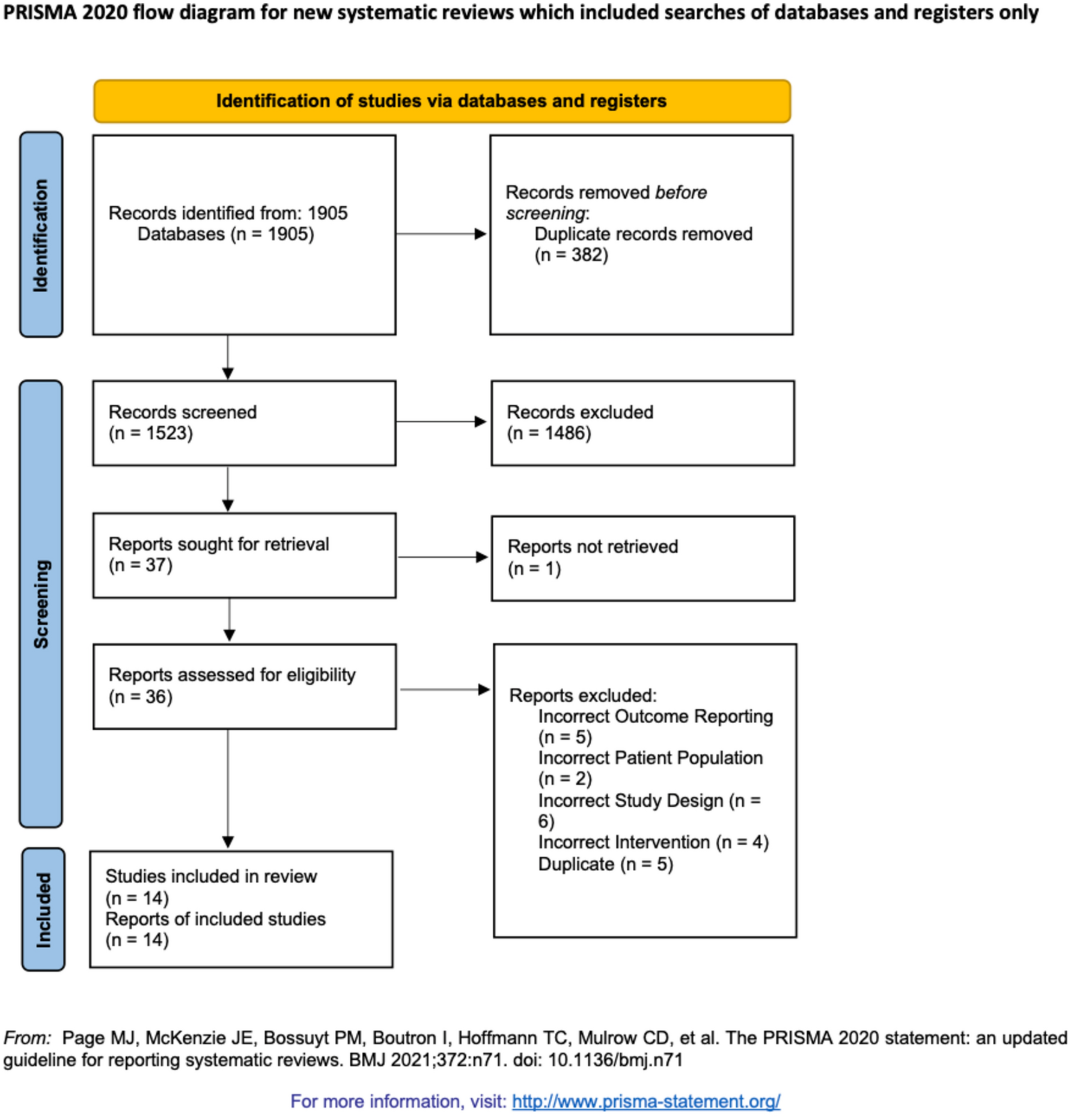
The literature search in MEDLINE (Ovid) and Embase (Ovid) returned 157 articles. One additional article was included from Google Scholar. Two additional relevant studies were identified through searches of ClinicalTrials.gov (ID NCT03797703 and NCT02130830), but these were not included as study results were not publicly available and were unable to be obtained by authors upon request. Sixty-nine duplicates were removed, and 82 records were excluded on title and abstract screening. Seven records were assessed in full text for eligibility, and all of these were included in the final analysis (Fig. 1).
Fig. 1
Flow chart of the literature search according to PRISMA guidelines
Study characteristicsAll studies provided information on study design and methods (Online Resource 2). All studies were parallel randomised controlled trials except one, which was a crossover trial [21]. The search identified no studies that used PNB for analgesia in haemorrhoid banding. In all studies, the intervention was LA at the area of the band: Four studies used bupivacaine injection [7, 22,23,24], one used lignocaine injection [10], one used lignocaine topical gel [25] and one used a cinchocaine-containing suppository [21]. Five studies used a non-placebo control [10, 22,23,24,25], and two studies used a placebo [7, 21] in addition or instead. The follow-up period for assessment of pain outcomes ranged from 2 h to 6 weeks. Five studies measured pain on a numerical scale: Four used a 10-point visual analogue scale [22,23,24,25] and one used a 100-point linear analogue scale [7]. The other two studies used a 4-point categorical scale [10] and a binary assessment (pain/no pain) [21].
Participant characteristicsThe total number of participants in included studies was 545. Of the reported participant characteristics, none varied significantly between control and intervention groups within or across studies (Table 1). Across the five studies that reported participant age and gender [7, 22,23,24,25], the mean age of participants in treatment groups was 37–56. Two studies reported pre-procedural pain and prior banding [24, 25]; 18–35% of participants experienced pain at baseline, and 8–17% of participants had undergone banding previously. Across the five studies that reported the number of bands applied intraoperatively [10, 22,23,24,25], most participants had > 1 band applied (70–100% of participants). No studies reported on participants’ regular analgesia use or specified whether any additional analgesia was administered intraoperatively (i.e. by the anaesthetist). One study reported the degree of haemorrhoids banded in study groups [22].
Table 1 Summary of participant characteristics in included trialsPrimary outcomesRegarding the primary outcome of post-procedural pain scores at 1, 6 and 24 h, the results were in favour of LA at all timepoints, and the difference between groups was significant at one hour. Overall, the mean difference in post-procedural pain scores between.
study groups decreased over time (Fig. 2).
Fig. 2
Mean difference in pain scores between participants undergoing rubber band ligation with local anaesthetic or no local anaesthetic at 1 h, 6 h and 24 h post-procedure
A total of 342 participants were included in meta-analysis of the primary outcome at one hour post-procedure, of whom 175 received LA and 167 did not receive LA [7, 21,22,23,24]. At 1 h, the mean difference in patient-reported pain scores was -1.43 points on a 10-point analogue scale (95% CI -2.30 to -0.56, p < 0.01), favouring LA (Fig. 2). Mean pain scores ranged from 0.92 to 3.40 and 3.67 to 4.68 in the LA and no LA groups, respectively.
At 6 h post-procedure, 250 participants were included in the analysis (130 received LA, 120 did not) [7, 23, 25]. The mean difference in patient-reported pain scores at 6 h was -0.52 (95% CI -1.04 to 0.01, p = 0.05), favouring LA (Fig. 2). Mean pain scores ranged from 2.31 to 3.00 and 2.50 to 3.67 in the LA and no LA groups, respectively.
At 24 h post-procedure, 247 participants were included in the analysis (127 received LA, 120 did not) [7, 23, 24]. The mean difference in patient-reported pain scores at 24 h was -0.31 (95% CI -0.82 to 0.19, p = 0.86), favouring LA (Fig. 2). Mean pain scores ranged from 2.00 to 2.40 and 2.30 to 3.10 in the LA and no LA groups, respectively.
Two studies did not measure pain on a numerical scale and were therefore excluded from meta-analysis. Williams et al. reported the proportion of participants who had pain 24 h post procedure; 56% had pain in the no LA group vs 63% in the LA group [21]. Law et al. reported the proportion of participants who reported ‘no pain’, ‘slight pain’, ‘moderate pain’ and ‘severe pain’ over the 2 weeks following their RBL procedure [10]. Overall, 63% of participants in the LA group experienced slight or moderate pain compared to 49% of participants in the no LA group. No participants reported severe pain.
Secondary outcomesThe only surrogate marker of pain reported by studies was post-procedural analgesia use. Three studies reported the mean number of analgesia tablets used [10, 21, 23], with participants in the no LA group using 1.75–2.70 tablets, and participants in the LA group using 1.47–2.40 tablets. One study reported the proportion of participants who had new analgesia use 72 h post-procedure [25], with 7/17 participants in the no LA group and 9/18 participants in the LA group commencing analgesia in this time. No studies reported time-to-discharge post-procedurally.
Safety dataPost-procedural complications were reported by all studies except Williams et al. (Tab.2). Studies did not report the number of patients in each group that had at least one complication, precluding meta-analysis of overall complications. Four studies reported the overall incidence of rectal bleeding (4–53%) [7, 10, 22, 23] and vasovagal symptoms (11–40%) [7, 23,24,25], and two reported the overall incidence of infection/sepsis (0% and 0%) [10, 23], urinary retention (8% and 29%) [7, 23], nausea (9% and 32%) [7, 23] and tenesmus (25% and 1%) [10, 23]. Some studies reported outcomes by treatment group, with the incidence of rectal bleeding and tenesmus similar between groups; the incidence of urinary retention higher in intervention groups; and the comparative incidence of nausea varying across studies. Meta-analysis was undertaken for the incidence of vasovagal symptoms, with a risk ratio of 1.01 (95% CI 0.64–1.60) (Fig. 3).
Table 2 The incidence of complications following rubber band ligation of haemorrhoids with and without local anaestheticFig. 3
The risk of vasovagal symptoms in participants undergoing rubber band ligation of haemorrhoids with local anaesthetic and no local anaesthetic
Quality assessment and risk of biasIn our GRADE assessment of the primary outcome (pain scores), the quality of the cumulative evidence was rated down to ‘low’ based on inconsistency and imprecision (Online Resource 3). There was substantial heterogeneity in the pain scores of included studies: At 1 h, I2 was 74% (50–90%), and at 6 and 24 h, I2 was measured as 0% due to the difference crossing zero. Imprecision was rated as ‘serious’ or ‘very serious’ at all timepoints because of small sample sizes and wide confidence intervals. Using the RoB 2 tools for parallel and crossover trials, the overall risk of bias with respect to the primary outcome in both parallel [7, 10, 22,23,24,25] and crossover [21] studies was rated as ‘some concerns’, mostly pertaining to ‘selection of the reported result’ and ‘measurement of the outcome’, which was at times unclear but not serious enough to further downgrade the evidence (Online Resource 4). Only one study included a funding statement [24], with no funding declared.
留言 (0)